
Abstract
Background
Long-term bisphosphonate use has often been associated with atypical femoral fractures. These fractures evolve from incomplete femoral fractures. A previous study demonstrated that the presence of a radiolucent line in an incomplete fracture can indicate a high risk of progression to complete fracture.
Questions/Purposes
The aim of this study is to present a management strategy for symptomatic bisphosphonate-associated incomplete atypical femoral fractures. Specific study questions include the following: (1) Is there a difference in the prognosis of these fractures based on the presence or absence of a radiolucent fracture line? (2) Can treatment with teriparatide assist in clinical/radiographic healing of these incomplete fractures? (3) Is there a characteristic biochemical profile in these patients?
Patients and Methods
We retrospectively examined all femur radiographs ordered by the metabolic bone disease service at our hospital between July 1, 2006 and July 1, 2011 and identified 10 patients with a total of 14 incomplete fractures. Nine patients received bisphosphonates for a mean duration of 10 ± 5 years (range, 4–17). The mean follow-up since the time of diagnosis was 20 ± 11 months (range, 6–36 months).
Results
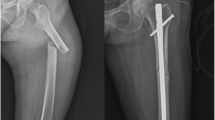
Five fractures did not have a radiolucent fracture line and were treated conservatively with partial weight-bearing restrictions and pharmacologic therapy. All five of these fractures healed with conservative management. Nine fractures had a radiolucent fracture line, and only two of these were treated successfully with conservative management including teriparatide. Six of the eight patients with a radiolucent line elected for surgical prophylaxis after 3 months of conservative management, whereas one patient underwent surgical prophylaxis without a trial of conservative management. Regarding the biochemical profiles, bone turnover markers for our patient cohort were in the lower quartile.
Conclusions
Fractures without a radiolucent line appear to respond to conservative management and not require surgical prophylaxis. Teriparatide treatment may hold promise in promoting healing of these fractures.




Similar content being viewed by others


References
Armamento-Villareal R, Napoli N, Diemer K, et al. Bone turnover in bone biopsies of patients with low-energy cortical fractures receiving bisphosphonates: A case series. Calcif Tissue Int. 2009;85(1):37–44.
Aspenberg P, Genant HK, Johansson T, et al. Teriparatide for acceleration of fracture repair in humans: A prospective, randomized, double-blind study of 102 postmenopausal women with distal radial fractures. J Bone Miner Res. 2010;25(2):404–414.
Banffy MB, Vrahas MS, Ready JE, Abraham JA. Nonoperative versus prophylactic treatment of bisphosphonate-associated femoral stress fractures. Clin Orthop Relat Res. 2011;469(7):2028–2034.
Black DM, Schwartz AV, Ensrud KE, et al. Effects of continuing or stopping alendronate after 5 years of treatment: The fracture intervention trial long-term extension (FLEX): A randomized trial. JAMA. 2006;296(24):2927–2938.
Boden BP, Osbahr DC, Jimenez C. Low-risk stress fractures. Am J Sports Med. 2001;29(1):100–111.
Bone HG, Hosking D, Devogelaer JP, et al. Ten years’ experience with alendronate for osteoporosis in postmenopausal women. N Engl J Med. 2004;350(12):1189–1199.
Burr DB, Forwood MR, Fyhrie DP, Martin RB, Schaffler MB, Turner CH. Bone microdamage and skeletal fragility in osteoporotic and stress fractures. J Bone Miner Res. 1997;12(1):6–15.
Capeci CM, Tejwani NC. Bilateral low-energy simultaneous or sequential femoral fractures in patients on long-term alendronate therapy. J Bone Joint Surg Am. 2009;91(11):2556–2561.
Cermak K, Shumelinsky F, Alexiou J, Gebhart MJ. Case reports: Subtrochanteric femoral stress fractures after prolonged alendronate therapy. Clin Orthop Relat Res. 2010;468(7):1991–1996.
Chesnut CH,3 rd, Silverman S, Andriano K, et al. A randomized trial of nasal spray salmon calcitonin in postmenopausal women with established osteoporosis: The prevent recurrence of osteoporotic fractures study. PROOF study group. Am J Med. 2000;109(4):267–276.
Das De S, Setiobudi T, Shen L, Das De S. A rational approach to management of alendronate-related subtrochanteric fractures. J Bone Joint Surg Br. 2010;92(5):679–686.
Deutsch AL, Coel MN, Mink JH. Imaging of stress injuries to bone. radiography, scintigraphy, and MR imaging. Clin Sports Med. 1997;16(2):275–290.
Dijkman BG, Sprague S, Schemitsch EH, Bhandari M. When is a fracture healed? radiographic and clinical criteria revisited. J Orthop Trauma. 2010;24 Suppl 1:S76-80.
Ellerington MC, Hillard TC, Whitcroft SI, et al. Intranasal salmon calcitonin for the prevention and treatment of postmenopausal osteoporosis. Calcif Tissue Int. 1996;59(1):6–11.
Goh SK, Yang KY, Koh JS, et al. Subtrochanteric insufficiency fractures in patients on alendronate therapy: A caution. J Bone Joint Surg Br. 2007;89(3):349–353.
Gomberg SJ, Wustrack RL, Napoli N, Arnaud CD, Black DM. Teriparatide, vitamin D, and calcium healed bilateral subtrochanteric stress fractures in a postmenopausal woman with a 13-year history of continuous alendronate therapy. J Clin Endocrinol Metab. 2011;96(6):1627–1632.
Ha YC, Cho MR, Park KH, Kim SY, Koo KH. Is surgery necessary for femoral insufficiency fractures after long-term bisphosphonate therapy? Clin Orthop Relat Res. 2010;468(12):3393–3398.
Ingle BM, Hay SM, Bottjer HM, Eastell R. Changes in bone mass and bone turnover following distal forearm fracture. Osteoporos Int. 1999;10(5):399–407.
Jobke B, Pfeifer M, Minne HW. Teriparatide following bisphosphonates: Initial and long-term effects on microarchitecture and bone remodeling at the human iliac crest. Connect Tissue Res. 2009;50(1):46–54.
Koh JS, Goh SK, Png MA, Kwek EB, Howe TS. Femoral cortical stress lesions in long-term bisphosphonate therapy: A herald of impending fracture? J Orthop Trauma. 2010;24(2):75–81.
Kwek EB, Goh SK, Koh JS, Png MA, Howe TS. An emerging pattern of subtrochanteric stress fractures: A long-term complication of alendronate therapy? Injury. 2008;39(2):224–231.
Lenart BA, Neviaser AS, Lyman S, et al. Association of low-energy femoral fractures with prolonged bisphosphonate use: A case control study. Osteoporos Int. 2009;20(8):1353–1362.
Leung F, Lau TW, To M, Luk KD, Kung AW. Atypical femoral diaphyseal and subtrochanteric fractures and their association with bisphosphonates. BMJ Case Rep. 2012; in press.
Liberman UA, Weiss SR, Broll J, et al. Effect of oral alendronate on bone mineral density and the incidence of fractures in postmenopausal osteoporosis. the alendronate phase III osteoporosis treatment study group. N Engl J Med. 1995;333(22):1437–1443.
Lyles KW, Colon-Emeric CS, Magaziner JS, et al. Zoledronic acid in reducing clinical fracture and mortality after hip fracture. N Engl J Med. 2007;357:nihpa40967.
Martin BR. The role of bone remodeling in preventing or promoting stress fractures. In: Burr DB, Milgrom C, eds. Musculoskeletal fatigue and stress fractures. Boca Raton: CRC; 2001:183–202.
Neviaser AS, Lane JM, Lenart BA, Edobor-Osula F, Lorich DG. Low-energy femoral shaft fractures associated with alendronate use. J Orthop Trauma. 2008;22(5):346–350.
Odvina CV, Levy S, Rao S, Zerwekh JE, Rao DS. Unusual mid-shaft fractures during long-term bisphosphonate therapy. Clin Endocrinol (Oxf). 2010;72(2):161–168.
Odvina CV, Zerwekh JE, Rao DS, Maalouf N, Gottschalk FA, Pak CY. Severely suppressed bone turnover: A potential complication of alendronate therapy. J Clin Endocrinol Metab. 2005;90(3):1294–1301.
Peichl P, Holzer LA, Maier R, Holzer G. Parathyroid hormone 1–84 accelerates fracture-healing in pubic bones of elderly osteoporotic women. J Bone Joint Surg Am. 2011;93(17):1583–1587.
Schaffler MB. Bone fatigue and remodeling in the development of stress fractures. In: Burr DB, Milgrom C, eds. Musculoskeletal fatigue and stress fractures. Boca Raton: CRC; 2001:161–182.
Shane E, Burr D, Ebeling PR, et al. Atypical subtrochanteric and diaphyseal femoral fractures: Report of a task force of the american society for bone and mineral research. J Bone Miner Res. 2010;25(11):2267–2294.
Sloan AV, Martin JR, Li S, Li J. Parathyroid hormone and bisphosphonate have opposite effects on stress fracture repair. Bone. 2010;47(2):235–240.
Spitz DJ, Newberg AH. Imaging of stress fractures in the athlete. Radiol Clin North Am. 2002;40(2):313–331.
Tervonen O, Junila J, Ojala R. MR imaging in tibial shaft fractures. A potential method for early visualization of delayed union. Acta Radiol. 1999;40(4):410–414.
Visekruna M, Wilson D, McKiernan FE. Severely suppressed bone turnover and atypical skeletal fragility. J Clin Endocrinol Metab. 2008;93(8):2948–2952.
Disclosures
Each author certifies that he or she has no commercial associations (e.g., consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article.
Each author certifies that his or her institution has approved the reporting of this case, that all investigations were conducted in conformity with ethical principles of research.
Author information
Authors and Affiliations
Corresponding author
Additional information
Level of evidence
Level IV, therapeutic study. See Guidelines for Authors for a complete description levels of evidence.
Rights and permissions
About this article
Cite this article
Saleh, A., Hegde, V.V., Potty, A.G. et al. Management Strategy for Symptomatic Bisphosphonate-Associated Incomplete Atypical Femoral Fractures. HSS Jrnl 8, 103–110 (2012). https://doi.org/10.1007/s11420-012-9275-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11420-012-9275-y