
Abstract
Background
Several studies have identified a specific fracture in the proximal diaphysis of the femur in patients treated with bisphosphonates. The fractures typically are sustained after a low-energy mechanism with the presence of an existing characteristic stress fracture. However, it is unclear whether these patients are best treated nonoperatively or operatively.
Questions/purposes
What is the likelihood of nonoperatively treated bisphosphonate-associated femoral stress fractures progressing to completion and during what time period? If prophylactic fixation is performed, do patients have a shorter hospital length-of-stay compared with patients having surgical fixation after fracture completion?
Patients and Methods
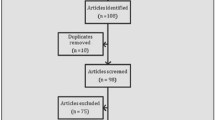
We retrospectively searched for patients older than 50 years receiving bisphosphonate therapy, with either incomplete, nondisplaced stress fractures or completed, displaced fractures in the proximal diaphysis of the femur between July 2002 and April 2009. After applying exclusion criteria, we identified 34 patients with a total of 40 bisphosphonate-associated fractures. The average duration of bisphosphonate use was 77 months. Twenty-eight of 40 (70%) fractures were completed, displaced fractures. Six of the 12 nondisplaced stress fractures initially were treated nonoperatively. The remaining six stress fractures were treated with prophylactic cephalomedullary nail fixation. The minimum followup was 12 months (mean, 36.5 months; range, 12–72 months).
Results
Five of the six stress fractures treated nonoperatively progressed to fracture completion and displacement at an average of 10 months (range, 3–18 months). The average hospital stay was 3.7 days for patients treated prophylactically and 6.0 days for patients treated after fracture completion.
Conclusions
Our data suggest nonoperative treatment of bisphosphonate-related femoral stress fractures is not a reliable way to treat these fractures as the majority progress to fracture completion. Prophylactic fixation of femoral stress fractures also reduces total hospital admission time.
Level of Evidence
Level IV, therapeutic study. See Guidelines for Authors for a complete description of levels of evidence.





Similar content being viewed by others


References
Advisory Task Force on Bisphosphonate-Related Osteonecrosis of the Jaws, American Association of Oral and Maxillofacial Surgeons. American association of oral and maxillofacial surgeons position paper on bisphosphonate-related osteonecrosis of the jaws. J Oral Maxillofac Surg. 2007;3:369–376.
Black DM, Kelly MP, Genant HK, Palermo L, Eastell R, Bucci-Rechtweg C, Cauley J, Leung PC, Boonen S, Santora A, de Papp A, Bauer DC; Fracture Intervention Trial Steering Committee; HORIZON Pivotal Fracture Trial Steering Committee. Bisphosphonates and fractures of the subtrochanteric or diaphyseal femur. N Engl J Med. 2010;362:1761–1771.
Black DM, Schwartz AV, Ensrud KE, Cauley JA, Levis S, Quandt SA, Satterfield S, Wallace RB, Bauer DC, Palermo L, Wehren LE, Lombardi A, Santora AC, Cummings SR; FLEX Research Group. Effects of continuing or stopping alendronate after 5 years of treatment: the Fracture Intervention Trial Long-term Extension (FLEX): a randomized trial. JAMA. 2006;296:2927–2938.
Cummings SR, Black DM, Thompson DE, Applegate WB, Barrett-Connor E, Musliner TA, Palermo L, Prineas R, Rubin SM, Scott JC, Vogt T, Wallace R, Yates AJ, LaCroix AZ. Effect of alendronate on risk of fracture in women with low bone density but without vertebral fractures: results from the Fracture Intervention Trial. JAMA. 1998;280:2077–2082.
Devas MB. Stress fractures of the femoral neck. J Bone Joint Surg Br. 1965;47:728–738.
Dijkman BG, Sprague S, Schemitsch EH, Bhandari M. When is a fracture healed? Radiographic and clinical criteria revisited. J Orthop Trauma. 2010;24(suppl 1):S76–80.
Goh SK, Yang KY, Koh JS, Wong MK, Chua SY, Chua DT, Howe TS. Subtrochanteric insufficiency fractures in patients on alendronate therapy: a caution. J Bone Joint Surg Br. 2007;89:349–353.
Ha YC, Cho MR, Park KH, Kim SY, Koo KH. Is surgery necessary for femoral insufficiency fractures after long-term bisphosphoante therapy? Clin Orthop Relat Res. 2010;468:3393–3398.
Haentjens P, Autier P, Barette M, Boonen S; Belgian Hip Fracture Study Group. The economic cost of hip fractures among elderly women: a one-year, prospective, observational cohort study with matched-pair analysis. Belgian Hip Fracture Study Group. J Bone Joint Surg Am. 2001;83:493–500.
Kwek EB, Goh SK, Koh JS, Png MA, Howe TS. An emerging pattern of subtrochanteric stress fractures: a long-term complication of alendronate therapy? Injury. 2008;39:224–231.
Lenart BA, Lorich DG, Lane JM. Atypical fractures of the femoral diaphysis in postmenopausal women taking alendronate. N Engl J Med. 2008;358:1304–1306.
Luckman SP, Hughes DE, Coxon FP, Graham R, Russell G, Rogers MJ. Nitrogen-containing bisphosphonates inhibit the mevalonate pathway and prevent post-translational prenylation of GTP-binding proteins, including Ras. J Bone Miner Res. 1998;13:581–589.
Mashiba T, Hirano T, Turner CH, Forwood MR, Johnston CC, Burr DB. Suppressed bone turnover by bisphosphonates increases microdamage accumulation and reduces some biomechanical properties in dog rib. J Bone Miner Res. 2000;15:613–620.
Neviaser AS, Lane JM, Lenart BA, Edobor-Osula F, Lorich DG. Low-energy femoral shaft fractures associated with alendronate use. J Orthop Trauma. 2008;22:346–350.
Nieves JW, Bilezikian JP, Lane JM, Einhorn TA, Wang Y, Steinbuch M, Cosman F. Fragility fractures of the hip and femur: incidence and patient characteristics. Osteoporos Int. 2010;21:399–408.
Odvina CV, Zerwekh JE, Rao DS, Maalouf N, Gottschalk FA, Pak CY. Severely suppressed bone turnover: a potential complication of alendronate therapy. J Clin Endocrinol Metab. 2005;90:1897–1899.
Orthopaedic Trauma Association Committee for Coding and Classification. Fracture and dislocation compendium. J Orthop Trauma. 1996;10(suppl 1):v–ix, 1–154.
Physicians’ Desk Reference. 63rd Ed. Montvale, NJ: Thomson Reuters; 2009: 2005, 2341.
Ross JR, Saunders Y, Edmonds PM, Patel S, Broadley KE, Johnston SR. Systematic review of role of bisphosphonates on skeletal morbidity in metastatic cancer. BMJ. 2003;327:469.
Sayed-Noor AS, Sjoden GO. Case reports: two femoral insufficiency fractures after long-term alendronate therapy. Clin Orthop Relat Res. 2009;467:1921–1926.
Schneider JP. Bisphosphonates and low-impact femoral fractures: current evidence on alendronate-fracture risk. Geriatrics. 2009;64:18–23.
Shane E. Evolving data about subtrochanteric fractures and bisphosphonates. N Engl J Med. 2010;362:1825–1827.
Author information
Authors and Affiliations
Corresponding author
Additional information
Each author certifies that he or she has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
Each author certifies that his or her institution has approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
This work was performed at Massachusetts General Hospital and Brigham and Women’s Hospital.
About this article
Cite this article
Banffy, M.B., Vrahas, M.S., Ready, J.E. et al. Nonoperative versus Prophylactic Treatment of Bisphosphonate-associated Femoral Stress Fractures. Clin Orthop Relat Res 469, 2028–2034 (2011). https://doi.org/10.1007/s11999-011-1828-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-011-1828-8