
Abstract
A prothrombotic state is reported with severe COVID-19 infection, which can manifest in venous and arterial thrombotic events. Coagulopathy is reflective of more severe disease and anticoagulant thromboprophylaxis is recommended in hospitalized patients. However, the prevalence of thrombosis on the intensive care unit (ICU) remains unclear, including whether this is sufficiently addressed by conventional anticoagulant thromboprophylaxis. We aimed to identify the rate of thrombotic complications in ICU-treated patients with COVID-19, to inform recommendations for diagnosis and management. A systematic review was conducted to assess the incidence of thrombotic complications in ICU-treated patients with COVID-19. Observational studies and registries reporting thrombotic complications in ICU-treated patients were included. Information extracted included patient demographics, use of thromboprophylaxis or anticoagulation, method of identifying thrombotic complications, and reported patient outcomes. In 28 studies including 2928 patients, thrombotic complications occurred in 34% of ICU-managed patients, with deep venous thrombosis reported in 16.1% and pulmonary embolism in 12.6% of patients, despite anticoagulant thromboprophylaxis, and were associated with high mortality. Studies adopting systematic screening for venous thrombosis with Duplex ultrasound reported a significantly higher incidence of venous thrombosis compared to those relying on clinical suspicion (56.3% vs. 11.0%, p < 0.001). Despite thromboprophylaxis, there is a very high incidence of thrombotic complications in patients with COVID-19 on the ICU. Systematic screening identifies many thrombotic complications that would be missed by relying on clinical suspicion and should be employed, with consideration given to increased dose anticoagulant thromboprophylaxis, whilst awaiting results of prospective trials of anticoagulation in this cohort.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Highlights
-
The risk of thrombotic complications increases with the severity of COVID-19.
-
Thromboprophylaxis is recommended for hospitalised patients, but the effectiveness of this, and the incidence of thrombotic events in patients managed in the intensive care unit (ICU) is unknown.
-
In 28 studies assessing 2928 critically-ill patients with COVID-19 on the ICU, the incidence of thrombotic events was 34%, but studies employing systematic screening reported a significantly higher incidence of venous thrombosis compared to those relying on clinical suspicion alone (56.3% vs. 11.0%, p < 0.001), despite anticoagulant thromboprophylaxis.
-
Consideration should be given to systematic screening and increased dose anticoagulant thromboprophylaxis in patients with COVID-19 on the ICU.
Introduction
A prothrombotic state, attributable to a cytokine storm induced by severe acute respiratory syndrome coronavirus 2 (SARS-Cov-2) and leading to activation of the coagulation cascade, is a recognised feature of severe Coronavirus disease 2019 (COVID-19) infection. This can manifest in venous thromboembolism (VTE), arterial thrombosis and disseminated intravenous coagulation (DIC) and coagulopathy is reflective of more severe disease and adverse prognosis [1]. A significant number of patients with COVID-19 require single or multiple organ support on the Intensive Care Unit (ICU), estimated to be between 12 and 17% of patients [2,3,4,5]. with the reported mortality in these cohorts between 25 and 40% [2, 6].
Recent international guidelines recommend that hospitalized patients with COVID-19 who are immobile, have respiratory failure or co-morbidities, as well as those requiring intensive care, should receive pharmacological prophylaxis against VTE, in the absence of contraindications [7,8,9]. However, studies have raised concern that despite anticoagulant thromboprophylaxis, patients with COVID-19 on the ICU are at high risk of thromboembolic events [10]. Currently the exact prevalence of thrombosis in ICU-admitted patients with COVID-19 remains uncertain and in particular, whether this is sufficiently addressed by pharmacological thromboprophylaxis. Other published reviews of thrombotic complications associated with COVID-19, to date, have not specifically examined the rate of thrombotic complications in ICU-treated patients with COVID-19, nor the role of systematic screening for VTE in this cohort [11,12,13,14,15,16,17]. The aim of this systematic review was to identify the rate of thrombotic complications in patients with COVID-19 admitted to ICU to inform recommendations for diagnosis and management.
Methods
The present systematic review was performed in accordance with the Cochrane Handbook for Systematic Reviews and Interventions [18], using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [19], and registered in the PROSPERO database (CRD42020192147).
Search strategy
The Pubmed/MEDLINE database was searched on 10th November 2020 for articles between 1 January 2020 and 10th November 2020 that included keywords related to COVID-19 (Wuhan coronavirus 2019, 2019-nCoV, 2019nCoV, COVID-19, SARS-CoV-2), venous thrombosis, arterial thrombosis, stroke, myocardial infarction and mesenteric ischaemia (search codes are shown in Supplementary eTable 3). Two authors (W.J. and R.K.) independently screened articles. Reference lists of included studies, relevant articles, and related systematic reviews were assessed. Eligible articles were reviewed in depth, and disagreements or queries were resolved by consensus (D.A.G., W.J., R.K.).
Study selection
We included peer-reviewed observational studies and registries, both prospective and retrospective, which reported on thrombotic complications in patients with COVID-19 admitted to the ICU. Articles were only included if either the whole population or a subgroup of the main population were admitted to ICU, and the incidence of thrombosis in the ICU group was documented. Studies that reported on patients receiving extracorporeal membrane oxygenation (ECMO) were also included, given the specific consideration needed for thrombosis in these patients. Case reports or series, autopsy studies, articles not available in the English language, papers that repeated data already included in prior analysis and radiology studies which only selectively included those patients with radiological abnormalities, were excluded.
Data extraction
Full text articles of eligible studies were reviewed for data extraction by two authors (W.J., R.K.). Information extracted included patient demographics (age, gender, country of admitting centre, comorbidities), requirement for renal replacement therapy (RRT) or ECMO, thromboprophylaxis or anticoagulation upon admission to ICU (how many patients, what type and dose), method of identifying thrombotic complications (clinical suspicion or routine screening), incidence and type of venous or arterial thrombotic event, dates or duration of follow-up, and reported outcomes (hospital/ICU length of stay, mortality). In studies where a subgroup of ICU patients was included, only the results from this subgroup were included in data extraction.
Outcome measures
The primary outcome measure was the rate of occurrence of arterial or venous thrombotic complications. Secondary outcomes included the type of thrombosis including arterial or venous, hospital/ICU length of stay and mortality. Secondary analyses compared the rate of thrombotic complications between patients who were assessed with routine screening for VTE and those who were not.
Risk of bias within individual studies
The risk of bias (low, moderate, high or critical) of the included studies was assessed using the Cochrane Collaboration tool and based on the The Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I) assessment tool [20]. Given the limited number of publications and the recent interest in COVID-19, we did not assess the risk of publication bias as it is likely that both positive and negative findings would be published early in the course of the disease, although a bias in favour in publication of positive results cannot be excluded.
Statistical analysis
Continuous variables are presented as mean and standard deviation, or median and inter-quartile range (IQR) for normal and non-normal distributions. Dichotomous variables are presented as frequencies and percentages. The chi-squared test was used to assess differences. p < 0.05 was taken as statistically significant. All analyses were performed using IBM SPSS Statistics Version 26.
Results
Search results
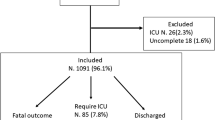
We identified 2429 articles on direct database search, with a further 15 records identified through other sources (Fig. 1). After de-duplication, screening article titles and abstracts, 2372 records were removed as not relevant to this review. The remaining 61 articles had assessment of the full text for eligibility. Of these, 32 were excluded; 14 due to absence of data on ICU patients, 6 because they only included a subgroup of patients who had undergone CT scans, 3 because they only included patients who had undergone ultrasound doppler, 2 because they repeated data from other studies, 2 because they were small case series, 2 that did not adequately quantify thrombotic outcomes, 2 because they only reported outcomes on patients who had a diagnosis of pulmonary embolism (PE) or stroke, and 1 because the article was not peer reviewed.

Flowchart of literature review
In total, 29 articles (28 studies) were included in the main analysis. Of these, 22 studies were specific to ICU patients, and 6 studies included a mixed population, with specific reporting on the subgroup of patients admitted to ICU. Two papers reported on the same patient group, with the second providing additional data to its predecessor [10, 21].
There was significant variation in the incidence of thrombotic events. Few studies reported all thrombotic event types (some only reported one type of thrombotic event); disease severity differed amongst studies with 4 studies reporting exclusively on patients on ECMO. Importantly, some studies used routine screening for thrombotic complications whilst others did not.
Study and patient characteristics
A total of 2928 patients were included and their clinical characteristics are shown in Tables 1. and 2. Where described (23 studies), mean patient age ranged from 45 to 70 years and 69% of subjects were male (24 studies). Although not all studies documented comorbidities, roughly a third of patients had diabetes, and there was a high prevalence of obesity, hypertension and cardiovascular disease. Nine studies documented use of ECMO. Eight studies documented use of RRT, which was employed in 18% of those patients.
Baseline VTE prophylaxis and anticoagulation
Twenty-four studies documented whether venous thromboprophylaxis or anticoagulation was used. Twenty-one studies described the use of anticoagulation, 20 studies documented prophylactic anticoagulation, and 8 defined the anticoagulant dose used. There was significant variability between studies on the type, dose and indication for prophylactic or therapeutic anticoagulation, and within some studies the thromboprophylaxis dosing policy changed during the analysis (Table 3).
Identification of thrombotic complications
Twenty-four studies described the method of identifying thrombotic complications. Of these, 8 studies involved systematic screening for VTE in all patients [22,23,24,25,26,27,28,29], one study performed selective VTE screening [30], whilst 20 studies did not utilise screening and relied on clinical suspicion to undertake tests for VTE. Two ECMO studies performed a thoraco-abdominopelvic CT on all new retrievals [23, 24].
The method of screening for deep venous thrombosis (DVT) included Duplex ultrasound of the limbs upon admission to ICU [22, 25, 26, 28, 29]. In 3 studies, a repeat ultrasound was performed in patients without DVT on the first ultrasound, between 2 and 7 days after the initial scan [25, 26, 31].
Occurrence of thrombotic complications
All studies quantified at least one type of thrombotic complication (Fig. 2 and Table 2). Thrombosis of any kind was reported in 996 patients (34%). Incidence of DVT was 16.1% (reported in 24 studies) and of PE 12.6% (22 studies). The incidence of arterial thrombotic events was 12% (9 studies), which included myocardial infarction (8%), ischaemic cerebrovascular accident (3%), limb or mesenteric infarction (2.5%).

Bar chart presenting percentage of patients with thrombotic complications by study. Panel background shows studies that employed routine screening for venous thrombosis (blue) and those that relied on clinical suspicion to investigate thrombotic complications (green). * Denotes those studies employing routine screening for venous thromboses. ✣ Denotes those studies employing routine screening for venous thromboses with computed tomography. # This study employed routine screening for venous thrombosis in only 51% of patients. † This study did not differentiate the types of arterial or venous thrombotic events, although reporting 7.6% venous thrombotic events (blue) and 5.6% arterial events (red). CVA cerebrovascular accident, DVT deep vein thrombosis, ECMO extracorporeal membrane oxygenator, MI myocardial infarction, PE pulmonary embolism
All studies concluded that the rate of thrombosis was high, and management of these patients ought to be specifically tailored to reduce thrombotic complications. Eleven studies suggested better risk assessment for thrombosis, with the use of D-dimer and improved diagnostic strategies [10, 21, 26,27,28, 30, 32,33,34,35,36], whilst 7 suggested increasing the dose of anticoagulation administered, as thrombotic events were high despite pharmacological thromboprophylaxis [10, 25, 26, 32, 34, 35, 37]. Some papers recommended routine systematic anticoagulation for all [25], while one group recommended a higher dose of thromboprophylaxis [37], which had already been adopted at that centre.
Routine screening vs. clinical suspicion to investigate thrombosis
Studies employing routine screening reported a much higher rate of thrombotic complications than studies without routine screening (Tables 2 and 3 and Fig. 2). The pooled incidence of DVT was 11% in studies without systematic screening, whereas studies employing routine screening reported a rate of 56.3% (p < 0.001). The incidence of PE ranged from 3 to 35%. With the exception of two studies which only reported on patients on ECMO, none of the studies adopted routine screening for PE with CT pulmonary angiography.
Thrombotic complications of patients receiving ECMO
Five studies described thrombotic events in patients receiving ECMO [23, 24, 38,39,40]. In the one study which performed screening, all 13 patients developed thromboembolism during ECMO, with 85% developing DVT, 23% developing PE, one a thrombotic occlusion of the centrifugal pump and one oxygenator thrombosis [24]. Amongst 51 ECMO patients where screening CT was performed, the incidence of PE was 35% [23], whilst another study reported ECMO-related thrombosis in 64% of patients, a significantly higher prevalence than that in non-COVID-19 controls [40]. Another study reported a 33% rate of thrombotic complications, including 17% mortality related to thrombotic complications [39].
Thrombotic complications and in-hospital mortality
Of the 28 studies, 20 reported in-hospital mortality, ranging from 9 to 54% (eTable 1). Nine studies reported on the differential mortality between those with and without thrombotic complications. One cohort study of 184 patients showed that patients with VTE had higher mortality than patients without thromboembolism [10, 21]. However, a subsequent larger study of 829 ICU patients showed similar mortality rate between those who developed any thrombotic event (59.8%) and those who did not (52.1%) [41]. At the point of analysis, 14 studies reported that patients remained in hospital, ranging from 6 to 83% of patients. Eight studies reported the number of patients who had been discharged from hospital, ranging from 0 to 79% of patients. The length of hospital stay and duration of follow up were only documented in a few studies (eTable 1).
Risk of bias within individual studies
The risk of bias in the included studies was assessed using the Cochrane Collaboration tool (eTable 4). Thirteen studies showed a high risk of bias, notably selection bias secondary to early reporting of results, without a set follow-up period. There is also significant reporting bias, due to limited reporting of all thromboembolic complications.
Discussion
This review demonstrates a very high incidence of thrombotic complications in patients with COVID-19 admitted to ICU, despite anticoagulant thromboprophylaxis. Secondly, it is clear that thrombotic complications are frequently undetected in the ICU setting, as evidenced by the very high incidence in studies that employed systematic screening for thrombotic complications, compared to those that relied on clinical suspicion to trigger investigation.
The rate of thrombotic complications appears significantly higher than that seen in patients with non-COVID-19 sepsis or pneumonia admitted to ICU. One of the studies included in our review compared COVID-19 patients with matched non-COVID-19 patients with ARDS on the ICU and showed a much higher rate of thrombotic complication with COVID-19 (11.7% vs. 4.8%) [38]. Similarly, Poissy et al. reported a much higher rate of thrombotic complications in patients admitted to ICU with COVID-19 than in ICU-admitted patients with influenza (20.6% vs 6.1%) [34]. A report on 198 hospitalised patients with COVID-19 receiving thromboprophylaxis (75 of whom were treated on ICU), showed the incidence of thrombotic complications increased over time and was related to increased mortality [30].
Clinically, thrombotic complications are often difficult to recognise in intubated patients, particularly in patients with COVID-19, where any deterioration in lung function due to PE or pulmonary thrombosis may be assumed to be part of the clinical progression of the ARDS. Furthermore, CT imaging may be less frequently performed due to the challenges and risks associated with moving critically unwell ventilated patients to a scanner, complicated further by the necessity to limit intra-hospital COVID-19 transmission. However, the high incidence of thrombotic complications in studies using systematic screening implies that clinical suspicion alone results in significant under-detection of thromboembolic events on ICU. This is supported by autopsy studies which show high rates of thrombosis at the macrovascular and microvascular level [42].
A prothrombotic state is an emerging hallmark of severe COVID-19 and elevations in D-dimer and prothrombin time are well documented and related to increased mortality [43], with severe coagulation abnormalities reported in almost all patients with severe disease [44, 45]. However, measurement of D-dimer level is generally not helpful in predicting thrombotic complications in ICU-treated patients, in particular given the significant baseline elevations in this cohort [46], supporting the case for systematic imaging in this cohort.
The importance of anticoagulant thromboprophylaxis in patients hospitalised with COVID-19 is well recognised. In March, the International Society on Thrombosis and Haemostasis (ISTH) and the American Society of Haematology recommended that all hospitalized COVID-19 patients should receive prophylactic-dose low molecular weight heparin (LMWH) unless contraindicated [47, 48]. The American College of Chest Physicians (CHEST) expert panel guideline, published on June 2, 2020 [7] recommends standard dose anticoagulant thromboprophylaxis in ICU patients, and does not advocate addition of mechanical prophylaxis (i.e. intermittent pneumatic compression) to pharmacological thromboprophylaxis. On the other hand, the latest ISTH consensus statement published on May 27, 2020 [8] whilst recommending routine thromboprophylaxis in COVID-19 patients on the ICU with preferably standard-dose LMWH or unfractionated heparin, recommended that patients with obesity should be considered for a 50% increase in the dose of thromboprophylaxis and multi-modal thromboprophylaxis with mechanical methods should be considered. Furthermore, intermediate-dose LMWH for ICU patients was advocated by up to 50% of ISTH respondents. This is supported by an analysis of 2,733 hospitalised patients with COVID-19 in New York which reported that anticoagulation improved survival, and subgroup analysis indicated that use of treatment-dose anticoagulation (received by 28% of patients) may be associated with improved survival compared to no-anticoagulation or prophylactic-dose anticoagulation, particularly in patients receiving mechanical ventilation [49]. A retrospective evaluation of 3480 patients with COVID-19 of whom 18% required ICU, showed the benefit of anticoagulation in reducing mortality appeared to be dose-dependent, with the greatest impact in those with critical illness [50].
The current anticoagulant thromboprophylaxis employed by the majority of studies reported here appears insufficient in patients with COVID-19 managed on the ICU. There may be a number of possible explanations for this. Firstly, the prothrombotic state in severe COVID-19 sepsis may be much more profound than previously appreciated, and more severe than in patients with severe sepsis of other aetiology. Further, owing to viral adhesion occuring on the ACE2 receptor on endothelial cells, the degree of endothelial dysfunction through viral replication, inflammatory cell infiltration and apoptosis may be greater [46]. Secondly, because of the difficulty in detecting VTE on the ICU, it is possible that in some patients thrombotic complications developed before admission to ICU and perhaps even before thromboprophylaxis was instituted. Thirdly, obesity is highly prevalent amongst this cohort and it is possible that the dose of thromboprophylaxis may have been insufficient for those with extreme BMI.
This review also highlights the high incidence of arterial thrombotic events, corroborated by other studies [60, 61]. In the setting of COVID-19, myocardial injury, defined by an increased troponin level, is predominantly attributable to non-ischaemic myocardial processes. Thus, whilst many early reports in patients with COVID-19 equated a troponin rise with myocardial infarction, typically this is more like to be related to sepsis and associated systemic inflammatory response, pro-coagulant status, and myocarditis. Without regular screening with cardiac biomarkers, in the absence of major ECG changes, myocardial injury in patients with COVID-19 can be frequently missed and yet is associated with an increased mortality [62, 63]. Likewise, stroke can be very challenging to recognise in patients who are intubated and ventilated, due to masking of clinical signs and symptoms with sedation and neuromuscular blockade. Unlike the case with the use of anticoagulation for thromboprophylaxis of venous thrombotic events, there are no convincing data that use of antiplatelet agents (or indeed anticoagulation) can reduce the frequency of arterial thrombotic events in patients with COVID-19 on the ICU.
Limitations
There is inherent bias in all observational cohort studies. Selection bias may favour the identification and publication of case cohorts with high rates of thrombotic complications. The retrospective nature of many studies will add bias. Differences between studies will add to bias, including variation in the ICU population studied (some including the highest risk patients on ECMO and RRT, others including lower risk patients requiring non-invasive ventilation), differential methods of diagnosing COVID-19 (whether by nasopharyngeal swab or antibody testing), variation in type and dose of anticoagulant thromboprophylaxis and differential thresholds for investigating thrombotic complications. Some papers report only one type of thrombosis, whilst others report all available thrombosis data. Furthermore, differences in follow-up between studies will underestimate rates of thromboses, with varilable proportions of the study population remaining in hospital, on ICU, or even on ECMO at the point of publishing [39]. We compared studies that used systematic screening to those depending on clinical suspicion to diagnose thrombotic complications. In addition, differences in patient cohorts, both in terms of characteristics reported (such as age, obesity, diabetes, country/type of healthcare where study was undertaken) and those not reported, such as other co-morbidities, medications and ethnicity, the latter in particular is highly pertinent as black, Asian and minority ethnic (BAME) groups have been reported to be adversely affected by COVID-19.
Conclusion
Despite anticoagulant thromboprophylaxis, there is a very high incidence of thrombotic complications in patients with COVID-19 admitted to ICU, and systematic screening identifies many thrombotic complications that would be missed by relying on clinical suspicion to trigger investigation. Systematic screening for VTE is therefore recommended in this cohort, and higher dose thromboprophylaxis should be considered, whilst awaiting the results of prospective studies to guide anticoagulation in patients with severe COVID-19 disease.
Abbreviations
- BMI:
-
Body mass index
- COVID-19:
-
Corona virus disease 2019
- DIC:
-
Disseminated intravascular coagulation
- DVT:
-
Deep venous thrombosis
- ECMO:
-
Extra-corporeal membrane oxygenation
- ICU:
-
Intensive care unit
- LMWH:
-
Low molecular weight heparin
- PE:
-
Pulmonary embolism
- RRT:
-
Renal replacement therapy
- SARS-Cov-2:
-
Severe acute respiratory syndrome coronavirus 2
- VTE:
-
Venous thromboembolism
References
Tang N, Li D, Wang X, Sun Z (2020) Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J Thromb Haemost 18:844–847. https://doi.org/10.1111/jth.14768
(2020) Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19)
Remuzzi A, Remuzzi G (2020) COVID-19 and Italy: what next? Heal Policy www.thelancet.com 395:1225–1228. https://doi.org/https://doi.org/10.1016/S0140-6736(20)30627-9
Grasselli G, Pesenti A, Cecconi M (2020) Critical care utilization for the COVID-19 outbreak in lombardy, italy: early experience and forecast during an emergency response. JAMA 323:1545–1546. https://doi.org/10.1001/jama.2020.4031
Docherty AB, Harrison EM, Green CA et al (2020) Features of 20 133 UK patients in hospital with covid-19 using the ISARIC WHO clinical characterisation protocol: prospective observational cohort study. BMJ 369:m1985. https://doi.org/10.1136/bmj.m1985
Richardson S, Hirsch JS, Narasimhan M et al (2020) Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City Area. JAMA 323:2052–2059. https://doi.org/10.1001/jama.2020.6775
Moores LK, Tritschler T, Brosnahan S et al (2020) Prevention, diagnosis, and treatment of VTE in patients with coronavirus disease 2019: CHEST guideline and expert panel report. Chest 158:1143–1163. https://doi.org/10.1016/j.chest.2020.05.559
Spyropoulos AC, Levy JH, Ageno W et al (2020) Scientific and standardization committee communication: clinical guidance on the diagnosis, prevention, and treatment of venous thromboembolism in hospitalized patients with COVID-19. J Thromb Haemost 18:1859–1865. https://doi.org/10.1111/jth.14929
Bikdeli B, Madhavan MV, Jimenez D et al (2020) COVID-19 and thrombotic or thromboembolic disease: implications for prevention, antithrombotic therapy, and follow-up: JACC state-of-the-art review. J Am Coll Cardiol 75:2950–2973. https://doi.org/10.1016/j.jacc.2020.04.031
Klok FA, Kruip MJHA, van der Meer NJM et al (2020) Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb Res 191:145–147. https://doi.org/10.1016/J.THROMRES.2020.04.013
Di Minno A, Ambrosino P, Calcaterra I, Di Minno MND (2020) COVID-19 and venous thromboembolism: a meta-analysis of literature studies. Semin Thromb Hemost 46:763–771. https://doi.org/10.1055/s-0040-1715456
Al-Ani F, Chehade S, Lazo-Langner A (2020) Thrombosis risk associated with COVID-19 infection. A scoping review Thromb Res 192:152–160. https://doi.org/10.1016/j.thromres.2020.05.039
Chi G, Lee JJ, Jamil A et al (2020) Venous thromboembolism among hospitalized patients with COVID-19 undergoing thromboprophylaxis: a systematic review and meta-analysis. J Clin Med 9:2489. https://doi.org/10.3390/jcm9082489
Wang C, Zhang H, Zhou M, et al (2020) Prognosis of COVID-19 in patients with vein thrombosis: a systematic review and meta-analysis. Eur Rev Med Pharmacol Sci 24:10279–10285. https://doi.org/https://doi.org/10.26355/eurrev_202010_23252
Porfidia A, Valeriani E, Pola R et al (2020) Venous thromboembolism in patients with COVID-19: Systematic review and meta-analysis. Thromb Res 196:67–74. https://doi.org/10.1016/j.thromres.2020.08.020
Roncon L, Zuin M, Barco S et al (2020) Incidence of acute pulmonary embolism in COVID-19 patients: systematic review and meta-analysis. Eur J Intern Med. https://doi.org/10.1016/j.ejim.2020.09.006
Jiménez D, García-Sanchez A, Rali P et al (2020) Incidence of VTE and bleeding among hospitalized patients with coronavirus disease 2019: a systematic review and meta-analysis. Chest. https://doi.org/10.1016/j.chest.2020.11.005
Higgins J, Green S (2011) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0
McInnes MDF, Moher D, Thombs BD et al (2018) Preferred reporting items for a systematic review and meta-analysis of diagnostic test accuracy studies: the PRISMA-DTA statement. JAMA 319:388–396. https://doi.org/10.1001/jama.2017.19163
Sterne JA, Hernán MA, Reeves BC, et al (2016) The Risk Of Bias In Non-randomised Studies of Interventions (ROBINS-I) assessment tool
Klok FA, Kruip MJHA, van der Meer NJM et al (2020) Confirmation of the high cumulative incidence of thrombotic complications in critically ill ICU patients with COVID-19: an updated analysis. Thromb Res 191:148–150. https://doi.org/10.1016/J.THROMRES.2020.04.041
Longchamp A, Longchamp J, Manzocchi-Besson S et al (2020) Venous thromboembolism in critically Ill patients with COVID-19: Results of a screening study for deep vein thrombosis. Res Pract Thromb Haemost 4:842–847. https://doi.org/10.1002/rth2.12376
Mak SM, Mak D, Hodson D et al (2020) Pulmonary ischaemia without pulmonary arterial thrombus in COVID-19 patients receiving extracorporeal membrane oxygenation: a cohort study. Clin Radiol 75:795.e1-795.e5. https://doi.org/10.1016/j.crad.2020.07.006
Parzy G, Daviet F, Puech B et al (2020) Venous thromboembolism events following venovenous extracorporeal membrane oxygenation for severe acute respiratory syndrome coronavirus 2 based on CT scans. Crit Care Med 48:e971–e975. https://doi.org/10.1097/CCM.0000000000004504
Nahum J, Morichau-Beauchant T, Daviaud F et al (2020) Venous thrombosis among critically Ill patients with coronavirus disease 2019 (COVID-19). JAMA Netw Open 3:e2010478. https://doi.org/10.1001/jamanetworkopen.2020.10478
Llitjos J-F, Leclerc M, Chochois C et al (2020) High incidence of venous thromboembolic events in anticoagulated severe COVID-19 patients. J Thromb Haemost 18:1743–1746. https://doi.org/10.1111/jth.14869
Voicu S, Delrue M, Chousterman B et al (2020) Imbalance between procoagulant factors and natural coagulation inhibitors contributes to hypercoagulability in the critically ill COVID-19 patient: clinical implications. Eur Rev Med Pharmacol Sci 27:9161–9168
Ren B, Yan F, Deng Z et al (2020) Extremely high incidence of lower extremity deep venous thrombosis in 48 patients with severe COVID-19 in Wuhan. Circulation 142:181–183. https://doi.org/10.1161/CIRCULATIONAHA.120.047407
Criel M, Falter M, Jaeken J et al (2020) Venous thromboembolism in SARS-CoV-2 patients: only a problem in ventilated ICU patients, or is there more to it? Eur Respir J. https://doi.org/10.1183/13993003.01201-2020
Middeldorp S, Coppens M, van Haaps TF et al (2020) Incidence of venous thromboembolism in hospitalized patients with COVID-19. J Thromb Haemost 18:1995–2002. https://doi.org/10.1111/jth.14888
Voicu S, Bonnin P, Stépanian A et al (2020) High prevalence of deep vein thrombosis in mechanically ventilated COVID-19 patients. J Am Coll Cardiol 76:480–482. https://doi.org/10.1016/j.jacc.2020.05.053
Longhitano Y (2020) Venous thromboembolism in critically ill patients affected by ARDS related to COVID-19 in Northern-West Italy. Eur Rev Med Pharmacol Sci 24:9154–9160
Cui S, Chen S, Li X et al (2020) Prevalence of venous thromboembolism in patients with severe novel coronavirus pneumonia. J Thromb Haemost 18:1421–1424. https://doi.org/10.1111/jth.14830
Poissy J, Goutay J, Caplan M et al (2020) Pulmonary embolism in COVID-19 patients: awareness of an increased prevalence. Circulation 142:184–186. https://doi.org/10.1161/CIRCULATIONAHA.120.047430
Hékimian G, Lebreton G, Bréchot N et al (2020) Severe pulmonary embolism in COVID-19 patients: a call for increased awareness. Crit Care 24:274. https://doi.org/10.1186/s13054-020-02931-5
Piazza G, Campia U, Hurwitz S et al (2020) Registry of arterial and venous thromboembolic complications in patients with COVID-19. J Am Coll Cardiol 76:2060–2072. https://doi.org/10.1016/j.jacc.2020.08.070
Thomas W, Varley J, Johnston A et al (2020) Thrombotic complications of patients admitted to intensive care with COVID-19 at a teaching hospital in the United Kingdom. Thromb Res 191:76–77. https://doi.org/10.1016/j.thromres.2020.04.028
Helms J, Tacquard C, Severac F et al (2020) High risk of thrombosis in patients with severe SARS-CoV-2 infection: a multicenter prospective cohort study. Intensive Care Med 46:1089–1098. https://doi.org/10.1007/s00134-020-06062-x
Beyls C, Huette P, Abou-Arab O et al (2020) Extracorporeal membrane oxygenation for COVID-19-associated severe acute respiratory distress syndrome and risk of thrombosis. Br J Anaesth. https://doi.org/10.1016/j.bja.2020.04.079
Bemtgen X, Zotzmann V, Benk C et al (2020) Thrombotic circuit complications during venovenous extracorporeal membrane oxygenation in COVID-19. J Thromb Thrombol. https://doi.org/10.1007/s11239-020-02217-1
Bilaloglu S, Aphinyanaphongs Y, Jones S et al (2020) Thrombosis in hospitalized patients with COVID-19 in a New York City Health System. JAMA 324:799–801. https://doi.org/10.1001/jama.2020.13372
Ackermann M, Verleden SE, Kuehnel M et al (2020) Pulmonary vascular endothelialitis, thrombosis, and angiogenesis in Covid-19. N Engl J Med 383:120–128. https://doi.org/10.1056/NEJMoa2015432
Zhou F, Yu T, Du R et al (2020) Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet (London, England) 395:1054–1062. https://doi.org/10.1016/S0140-6736(20)30566-3
Huang C, Wang Y, Li X et al (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet (London, England) 395:497–506. https://doi.org/10.1016/S0140-6736(20)30183-5
Chen N, Zhou M, Dong X et al (2020) Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet (London, England) 395:507–513. https://doi.org/10.1016/S0140-6736(20)30211-7
Connors JM, Levy JH (2020) COVID-19 and its implications for thrombosis and anticoagulation. Blood 135:2033–2040. https://doi.org/10.1182/blood.2020006000
Thachil J, Tang N, Gando S et al (2020) ISTH interim guidance on recognition and management of coagulopathy in COVID-19. J Thromb Haemost 18:1023–1026. https://doi.org/10.1111/jth.14810
Baumann Kreuziger L, Lee A, Garcia D, et al (2020) COVID-19 and VTE/Anticoagulation: Frequently Asked Questions
Paranjpe I, Fuster V, Lala A et al (2020) Association of treatment dose anticoagulation with in-hospital survival among hospitalized patients with COVID-19. J Am Coll Cardiol 76:122–124. https://doi.org/10.1016/j.jacc.2020.05.001
Ionescu F, Jaiyesimi I, Petrescu I et al (2020) Association of anticoagulation dose and survival in hospitalized COVID-19 patients: A retrospective propensity score-weighted analysis. Eur J Haematol. https://doi.org/10.1111/ejh.13533
Yuriditsky E, Horowitz JM, Merchan C et al (2020) Thromboelastography profiles of critically Ill patients with coronavirus disease 2019. Crit Care Med 48:1319–1326. https://doi.org/10.1097/CCM.0000000000004471
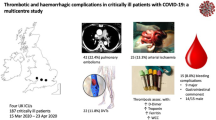
Shah A, Donovan K, McHugh A et al (2020) Thrombotic and haemorrhagic complications in critically ill patients with COVID-19: a multicentre observational study. Crit Care 24:561. https://doi.org/10.1186/s13054-020-03260-3
Lodigiani C, Iapichino G, Carenzo L et al (2020) Venous and arterial thromboembolic complications in COVID-19 patients admitted to an academic hospital in Milan, Italy. Thromb Res 191:9–14. https://doi.org/10.1016/j.thromres.2020.04.024
Fraissé M, Logre E, Pajot O et al (2020) Thrombotic and hemorrhagic events in critically ill COVID-19 patients: a French monocenter retrospective study. Crit Care 24:275. https://doi.org/10.1186/s13054-020-03025-y
Al-Samkari H, Karp Leaf RS, Dzik WH et al (2020) COVID and Coagulation: bleeding and thrombotic manifestations of SARS-CoV2 infection. Blood 136:489–500. https://doi.org/10.1182/blood.2020006520
Maatman TK, Jalali F, Feizpour C et al (2020) Routine venous thromboembolism prophylaxis may be inadequate in the hypercoagulable state of severe coronavirus disease 2019. Crit Care Med 48:e783–e790. https://doi.org/10.1097/CCM.0000000000004466
Desborough MJ, Doyle AJ, Griffiths A et al (2020) Image-proven thromboembolism in patients with severe COVID-19 in a tertiary critical care unit in the United Kingdom. Thromb Res 193:1–4. https://doi.org/10.1016/j.thromres.2020.05.049
Contou D, Pajot O, Cally R et al (2020) Pulmonary embolism or thrombosis in ARDS COVID-19 patients: a French monocenter retrospective study. PLoS ONE 15:e0238413. https://doi.org/10.1371/journal.pone.0238413
Hippensteel JA, Burnham EL, Jolley SE (2020) Prevalence of venous thromboembolism in critically ill patients with COVID-19. Br J Haematol 190:e126–e156. https://doi.org/10.1111/bjh.16908
Avula A, Nalleballe K, Toom S et al (2020) Incidence of thrombotic events and outcomes in COVID-19 patients admitted to intensive care units. Cureus 12:e11079. https://doi.org/10.7759/cureus.11079
de Roquetaillade C, Chousterman BG, Tomasoni D, Zeitouni M, Houdart E, Guedon A, Reiner P, Bordier R, Gayat E, Montalescot G, Metra M, Mebazaa A (2021) Unusual arterial thrombotic events in Covid-19 patients. Int J Cardiol 323:281–284
Hinton J, Mariathas M, Grocott MP, Curzen N (2020) High sensitivity troponin measurement in critical care: flattering to deceive or ‘never means nothing’? J Intensive Care Soc 21(3):232–240
Giustino G, Croft LB, Stefanini GG, Bragato R, Silbiger JJ, Vicenzi M, Danilov T, Kukar N, Shaban N, Kini A, Camaj A, Bienstock SW, Rashed ER, Rahman K, Oates CP, Buckley S, Elbaum LS, Arkonac D, Fiter R, Singh R, Li E, Razuk V, Robinson SE, Miller M, Bier B, Donghi V, Pisaniello M, Mantovani R, Pinto G, Rota I, Baggio S, Chiarito M, Fazzari F, Cusmano I, Curzi M, Ro R, Malick W, Kamran M, Kohli-Seth R, Bassily-Marcus AM, Neibart E, Serrao G, Perk G, Mancini D, Reddy VY, Pinney SP, Dangas G, Blasi F, Sharma SK, Mehran R, Condorelli G, Stone GW, Fuster V, Lerakis S, Goldman ME (2020) Characterization of myocardial injury in patients with COVID-19. J Am Coll Cardiol 76(18):2043–2055
Funding
None.
Author information
Authors and Affiliations
Author notes
William J. Jenner and Rahim Kanji are joint first authors.
Despite thromboprophylaxis, there is a very high incidence of thrombotic complications in patients with COVID-19 on the ICU, affecting up to 85-92% patients. Systematic screening with ultrasonography identifies many venous thrombotic complications that could be missed by relying on clinical suspicion, and is recommended, with consideration of increased dose anticoagulatant thromboprophylaxis.
Contributions
WJ: design, analysis and interpretation of data, drafting of the manuscript. RK: design, analysis and interpretation of data, drafting of the manuscript. SM: interpretation and critical review. YG: analysis and interpretation of data. SP: interpretation and critical review. SP: interpretation and critical review. DG: concept, design and analysis and interpretation of data, critical revision for important intellectual content, final approval of the manuscript submitted.
Corresponding author
Ethics declarations
Conflict of interest
The author declares that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Impact
Despite thromboprophylaxis, there is a very high incidence of thrombotic complications in patients with COVID-19 on the ICU, affecting up to 85-92% patients. Systematic screening with ultrasonography identifies many venous thrombotic complications that could be missed by relying on clinical suspicion, and is recommended, with consideration of increased dose anticoagulatant thromboprophylaxis.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Jenner, W.J., Kanji, R., Mirsadraee, S. et al. Thrombotic complications in 2928 patients with COVID-19 treated in intensive care: a systematic review. J Thromb Thrombolysis 51, 595–607 (2021). https://doi.org/10.1007/s11239-021-02394-7
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11239-021-02394-7