
Abstract
Current treatment guidelines for sepsis claim an early goal-directed hemodynamic optimization including fluid resuscitation, use of vasopressors and inotropic agents. We investigated the correlation between the prominent treatment goal central venous saturation (ScvO2) and the frontal and the thenar regional oxygen saturation (rSO2) measured by near infrared spectroscopy. Secondary, we examined the value of ScvO2, lactate levels and rSO2 as surrogate markers of an impaired tissue oxygenation for outcome prediction in sepsis. This prospective, observational study was performed at the surgical intensive care unit of the University Hospital Giessen. A total of 50 patients with sepsis, severe sepsis or septic shock were included. ScvO2, rSO2 and lactate were measured at sepsis diagnosis (baseline), 24 and 48 h, thereafter. We investigated the predictive value of frontal and thenar rSO2 for a decreased SvcO2 under 70 %. For survivor and non-survivors ScvO2, rSO2 and lactate were analysed. Patients with ScvO2 >70 % showed a trend to higher levels of fontal rSO2 (62.81 ± 8.06 vs. 53.54 ± 15.48; p = 0.058). ROC-analysis revealed a minor prediction of a decreased ScvO2 by frontal rSO2 levels at baseline (AUC = 0.687; 95 % CI 0.511–0.863; p = 0.047). Combined measurements of lactate and ScvO2 showed significantly elevated mortality for patients with ScvO2 ≥70 % and lactate levels ≥2.5 mmol/l (log rank test p = 0.004). In the group with ScvO2 <70 % and lactate levels <2.5 mmol/l no patients died during the observation period. Frontal rSO2 correlates with ScvO2 but both frontal and thenar rSO2 do not exactly discriminate between patients with high or low ScvO2 in sepsis. The combination of elevated lactate >2.5 mmol/l and ScvO2 >70 % is highly associated with poor outcome in ICU patients with sepsis, severe sepsis and septic shock.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Severe sepsis is responsible for 6–15 % of admissions to the intensive care unit (ICU) [1–3]. In non-cardiac ICUs, sepsis is the second-leading cause for mortality with an estimated mortality rate of 30–50 %. Current treatment guidelines for sepsis, severe sepsis, and septic shock claim for early source control, antimicrobial treatment and hemodynamic stabilization including fluid resuscitation, use of vasopressors and inotropic agents [4]. Rivers et al. [5] showed that an early goal directed therapy including monitoring of the central venous oxygen saturation (ScvO2) is able to improve patients’ outcome in severe sepsis and septic shock. Cardiovascular failure in sepsis often induces disturbance in oxygen delivery. Following tissue hypoxia could lead to elevated lactate concentrations [6]. Numerous studies have demonstrated the use of lactate as a diagnostic and prognostic marker of global tissue hypoxia in critical ill and septic patients [7, 8] [9]. Current sepsis guidelines recommend an early goal directed approach including ScvO2 and lactate measurements [4].
Measurement of ScvO2 has been clinically approved to assess changes in oxygen delivery and consumption in various clinical settings [10]. Unfortunately this method requires frequent blood draws from a central venous catheter or the use of expensive spectrophotometric ScvO2 catheters. Non-invasive monitoring methods of tissue oxygenation may provide useful information about the state of tissue oxygenation and microcirculation. A potential gain of information may be offered by near-infrared spectroscopy (NIRS).
NIRS uses computer analysis of spectra in the near-infrared range (680–800 nm) to assign regional tissue haemoglobin (Hb) oxygen saturation (rSO2) [11]. It is used to determine cerebral and somatic tissue saturation rSO2 via sensors placed on patients’ forehead or somatic areas (thenar muscle, nephral tissue). Measurement of frontal rSO2 by NIRS has been correlated with central venous saturation in animals and children [12, 13]. Detection of rSO2 is also used as a surrogate for hemodynamic function [13, 14]. Even thenar rSO2 was shown to correlate with severity of illness and outcome in sepsis [14–17]. In a previous preliminary study, we found a significant correlation between frontal rSO2 and ScvO2 in patients with severe sepsis and septic shock. A ScvO2 <70 % was indicated by a rSO2 <56.5 % with a sensitivity and specificity of 75 and 100 %, respectively [18].
The aim of the study was to investigate the correlation between ScvO2 and rSO2. As secondary aim, we examined the value of ScvO2, lactate levels and rSO2 as surrogate markers of an impaired tissue oxygenation for outcome prediction in sepsis.
2 Materials and methods
2.1 Study population
This prospective observational study was performed at the surgical ICU of the University Hospital of Giessen (Trial registration: DRKS00003327). Ethical approval for this study (ethics proposal number AZ 57/12) was obtained from the Ethics Committee of the Faculty of Medicine at the Justus-Liebig-University Giessen, Giessen, Germany (Chairman Prof. H. Tillmanns) on 12 June 2012. Patients or their legal representative gave written informed consent before study inclusion. We enrolled 50 patients within the first 6 h after onset of sepsis, severe sepsis or septic shock, defined according to the definition of the International Sepsis Definitions conference [19]. Exclusion criteria were age <18 years, history of cerebral bleeding or stroke. All patients received standardized treatment including source control, fluid infusion, catecholamine infusion, glucose control and organ failure support or replacement therapy according to the surviving sepsis guidelines [4]. Thus, the early resuscitation was goal-directed to achieve a heart rate (HR) <100/min, a mean arterial pressure (MAP) ≥60 mmHg, a central venous pressure of 8 to 12 mmHg, a urinary output ≥0.5 ml/kg/hour, and a ScvO2 ≥70 %.
2.2 Measurements
For all enrolled patients we obtained and calculated values at baseline (T1) (baseline), 24 h (T2), and 48 h (T3) after inclusion. Recorded variables were age, ICU and hospital mortality, length of stay in ICU and hospital, septic focus, acute physiology and chronic health evaluation II score (APACHE II), sequential organ failure (SOFA) score, simplified acute physiology II score (SAPS II), ventilator parameters, norepinephrine dosage, HR, MAP, arterial and ScvO2, Hb, arterial and venous lactate, arterial and blood gas values, and Horowitz-Index.
The INVOS 5100C oximeter (Somanetics, Troy, MI, USA) was used to obtain frontal and thenar rSO2 measurements. The principle of clinical used NIRS is the non-invasive measurement of the attenuation of light by Hb, where the emitted light is in a wavelength range longer than visible light [20, 21]. Near-infrared spectroscopy wavelengths approximately 700–850 nm are generated by a light source of the sensor and penetrate the skin and the bone. Within the brain tissue in 2.5 cm depth the light is either absorbed or reflected to the sensor. Therefore, NIRS provides the total tissue oxy- and deoxyhemoglobin in a quantitative and qualitative manner to obtain oxygen supply and demand [20]. The measured results were expressed as a percentage of oxygen at the corresponding monitor.
The oxymetric sensors were placed after cleaning the forehead and thenar skin with alcoholic pads. Following a 5-min stabilization period, we assessed the rSO2.
2.3 Statistical analysis
Descriptive statistics were performed for demographics, clinical characteristics, hemodynamic values and laboratory findings. Continuous variables are presented as means and standard deviations or medians with interquartile ranges, and categorical variables as numbers and percentages. Comparisons between groups were analysed by t test. Comparisons of categorical variables were generated by the Pearson χ2 test. The predictive value of rSO2 for SvcO2 was calculated using receiver operator characteristic (ROC) curves and the area under the curve (AUC) was computed. Mortality analysis where performed by using Kaplan–Meier-Curves. A logistic regression analysis was performed to investigate predictors for mortality. Probability p values ≤0.05 were considered statistically significant. The entire statistical analysis was performed with SPSS®, version 19.0.0 (SPSS Inc., IBM, Chicago, Illinois).
3 Results
3.1 Baseline characteristics
A total number of 50 consecutive patients with severe sepsis or septic shock were enrolled in this study. Baseline characteristics of the study population are shown in Table 1. Patients’ mean age was 68.02 ± 13.52 years. The population was characterized by a significant morbidity reflected by high APACHE II Score (25.24 ± 6.76). The majority of patients required a norepinephrine therapy (84 %) to achieve an adequate circulatory status (Table 2). Almost 60 % of the patients suffered from septic shock at the time of inclusion. In the vast majority of patients, intra-abdominal or pulmonary infections were the cause of sepsis. The observed hospital mortality was 52 %. The mean rSO2 measured at baseline (T1) was 60.4 ± 11.1 %. At least, 25 % of patients included did not achieve a ScvO2 above 70 %. At baseline, 13 (26 %) patients represented ScvO2 below 70 %. Surprisingly, the number of patients with a decreased ScvO2 increased at the two following days compared to the initial stabilization phase (T2: 17 (43.6 %), T3: 10 (32.3 %)) (Table 2). In about 42 % of patients the measured arterial lactate was higher than 2.5 mmol/l.
At baseline, frontal rSO2 was significantly higher than the thenar rSO2 (Table 3). Nevertheless, higher rSO2 thenar values were found in 24 % of the patients at T1. At baseline and for the pooled study data (T1-T3), we revealed a moderate correlation between frontal and thenar rSO2 (T1: Pearson r = 0.451, p = 0.001; T1–T3: r = 0.442, p < 0.001).
Survivors and non-survivors represented no significant differences between their frontal and thenar rSO2 values (p = 0.24). Also the proportion of patients who revealed greater thenar than frontal rSO2 did not differ.
3.2 Relationship between rSO2 and ScvO2
We further stratified patients according to their ScvO2 to investigate the relationship between rSO2 and SvcO2 (Table 4). Patients were divided into patients with a ScvO2 <70 % and patients with a ScvO2 ≥70 %. We found no significant differences in APACHE II, SAPS II, SOFA, thenar rSO2, arterial lactate, venous lactate, SaO2, blood pressure, dose of norepinephrine, FiO2, positive end-expiratory pressure (PEEP), Horowitz Index and central venous pressure (CVP) between the groups. Patient characteristics solely differ in body weight (74.11 ± 18.4 vs. 99.54 ± 36.0; p = 0.028, data not shown). Patients with ScvO2 ≥70 % showed a trend towards higher levels of a frontal rSO2 (62.81 ± 8.06 vs. 53.54 ± 15.48; p = 0.058).
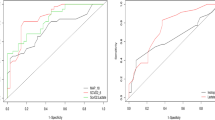
ROC-analysis revealed just a minor prediction of a decreased ScvO2 by frontal rSO2 levels at baseline (AUC = 0.687; 95 % CI 0.511–0.863; p = 0.047) (Fig. 1). Even after the combined analyses of the data from T1, T2 and T3, the prediction of ScvO2 by frontal rSO2 could not be improved (AUC 0.687; 95 % CI 0.512–0.721; p = 0.039). Regarding the pooled data we could only measure a weak correlation between thenar rSO2 and ScvO2 (Pearson: r = 0.223; p = 0.015) (Fig. 3).

Receiver operating characteristics for the prediction of ScvO2 <70 % by rSO2. ROC-Analysis for the prediction of ScvO2 <70 by frontal rSO2 at time T1 (n = 50) (black line). AUC 0.687 (95 % CI 0.511–0.863; p = 0.047). No significant prediction of ScvO2 <70 by thenar rSO2 at time T1 (n = 50) (grey line)

Kaplan–Meier-analysis for in-hospital mortality depending on lactate and central venous saturation. Kaplan–Meier-analysis for in-hospital mortality depending on lactate (mmol/l) and central venous saturation (ScvO2)(%) (black line: ScvO2 <70 % und Lactat <2.5 mmol/l; black broken line: ScvO2 <70 % und Lactate ≥2.5 mmol/l; gray line: ScvO2 ≥70 % und Lactate <2.5 mmol/l; gray broken line: ScvO2 ≥70 % und Lactate ≥2.5 mmol/l) (Log Rank p = 0.004)

Pearson correlation between frontal rSO2 and ScvO2. Pearson correlation between frontal rSO2 (%) and ScvO2 (%) using the pooled study data from each observation point (n = 110) (Pearson: r = 0.223; p = 0.015)
However, multivariate logistic regression analysis revealed frontal rSO2 as an independent predictor for a ScvO2 <70 % (OR 0.867; 95 % CI 0.784–0.958); p = 0.005). Other parameters did not show any significant relationship (Table 5).
3.3 Explorative analysis of survivors and non-survivors
Regarding the differences between survivors and non-survivors, we revealed a raised APACHE II Score (22.04 ± 5.61 vs. 28.19 ± 6.46; p = 0.001), and SAPS II Score (44.79 ± 14.21 vs. 56.00 ± 14.24; p = 0.008), lower MAP (T1) (mmHg) (84.50 ± 14.86 vs. 71.12 ± 11.55; p = 0.001), and therefore higher doses of norepinephrine (μg/kg/min) (0.18 ± 0.18 vs. 0.37 ± 0.4; p = 0.04) (Table 6). In addition, in the group of non-survivors, we detected higher (arterial and venous) lactate levels (mmol/l) (arterial 2.14 ± 2.16 vs. 5.86 ± 5.70; p = 0.004), and also surprisingly significantly raised ScvO2 (71.10 ± 8.09 vs. 76.41 ± 8.37; p = 0.027) at T1. Nevertheless, there was no difference in rSO2 levels according patient’s outcome.
ROC analysis revealed the best prediction for mortality by APACHE II Score (0.777; 95 % CI 0.648–0.907; p = 0.001) and arterial lactate (T1) (0.748; 95 % CI 0.612–0.883; p = 0.003). Also MAP (T1) (0.748; 95 % CI 0.610–0.886; p = 0.003), SAPS II Score (0.708; 95 % CI 0.565–0.852; p = 0.012), and ScvO2 (T1) levels (0.683; 95 % CI 0.535–0.832; p = 0.026) were predictive for mortality. Measurements of frontal rSO2 (T1) and SOFA Score did not serve for outcome prediction in this analysis (Table 7).
Referring the fact of increased mortality in patients with ScvO2 ≥70 % and lactate <2.5 mmol/l a four-field analysis for ScvO2 and lactate levels with the cut-off values according to the clinical outcomes were performed. Combining the measurements of lactate level and ScvO2, we detected the highest mortality (80 %) for patients with ScvO2 ≥70 % and lactate levels ≥2.5 mmol/l (Table 6), which is confirmed by the Kaplan–Meier analysis (log rank test p = 0.004) (Fig. 2). Surprisingly, no person of the septic population with ScvO2 <70 % and lactate levels <2.5 mmol/l died in this observation.
4 Discussion
In this prospective observational study, we performed repeated rSO2 measurements in 50 surgical ICU patients with sepsis to investigate the correlation between rSO2 and ScvO2. A secondary aim was to evaluate the value of rSO2, ScvO2 and lactate for outcome prediction in sepsis. We revealed just a weak predictive value for ScvO2 by frontal rSO2 measurement. Surprisingly, septic patients with “normal” ScvO2 ≥70 % and elevated lactate levels (≥ 2.5 mmol/l) showed the highest mortality.
In a primary preliminary analysis of 16 septic ICU patients we found that the frontal rSO2 could be predictive for a depressed ScvO2 <70 % (AUC = 0.844; p = 0.045). A ScvO2 <70 % was indicated by cerebral rSO2 <56.5 with a sensitivity and a specificity of 75 and 100 %, respectively [18]. The data from this larger prospective study indicate a lower predictive value for ScvO2 (AUC 0.617; 95 % CI 0.512–0.721; p = 0.039). Furthermore, patients representing ScvO2 ≥70 % showed a trend towards a higher hospital mortality (59.5 % vs. 30.8 %, p = 0.07) compared to patients with ScvO2 <70 %. Stratifying the study group for mortality, non-survivors represented significantly raised ScvO2 values, higher APACHE II scores, SAPS II scores, and elevated lactate values, respectively. We observed a significant overall mortality in the study population (52 %) as predicted by high mean APACHE II and SAPS II scores whereas the observed mean SOFA score just predict a mortality of 15 %.
In our study we investigated patients with sepsis regarding three observation points at our surgical ICU. Patients were treated according to the guidelines of the Surviving Sepsis campaign including early resuscitation, source control and empirical anti-infective treatment [4]. Various studies already used NIRS in different settings to evaluate the severity of sepsis, for mortality prediction in sepsis and as a marker of local tissue oxygenation [18, 22–25]. Thereby, many studies focused on the vascular reactivity through changes during vascular occlusion maneuver and time or therapy related changes [23, 24, 26]. Sepsis is characterized by pathological changes in vasomotor reactivity and microcirculation leading to cellular hypoxia [27]. Early hemodynamic stabilization represents the main target of modern therapy in septic patients to achieve adequate supply of oxygen [5]. Guidelines also recommend the use of advanced hemodynamic monitoring in septic patients even though its benefit for mortality reduction is still not proved [4, 28]. ScvO2 reflects global balance of oxygen supply and consumption in case of stabile respiratory conditions [29]. Further, lactate levels constitute a surrogate for impaired peripheral oxygen supply [30–32]. In order to this fact early hemodynamic stabilization in patients with sepsis should be proved by a decrease in lactate under a cut cut-off level of 2.5 mmol/l. Continuous measurement of therapeutic goals could be an opportunity to improve therapeutic efficiency but is also associated with higher costs. Moreover, continuous ScvO2 measurement is not associated with outcome improvement [33]. NIRS could be an additional monitoring tool for continuous, non-invasive assessment of tissue oxygenation in patients with impaired cardiac function [34–36].
In this prospective study we focused on rSO2 baseline measurements and found a limited association between frontal rSO2 and ScvO2. However, patients with ScvO2 <70 % did not have significantly lower rSO2 values. Nevertheless, multivariate regression analysis revealed frontal rSO2 at T1 as predictive for ScvO2 (p = 0.005). According to previous studies in patients with severe sepsis and septic shock we also found only a weak correlation between thenar rSO2 and ScvO2 [14, 23, 37, 38]. Comparably, Mesquida et al. [39] showed the ability to predict ScvO2 values in septic patients by the thenar rSO2 and found a moderate correlation between both parameters (Pearson: r = 0.39; p = 0.017). Interestingly, Podbregar et al. [37] showed that thenar rSO2 does not estimate SvO2 in patients with severe left heart failure and additional severe sepsis or septic shock. But in patients with severe left heart failure without additional severe sepsis or septic shock, rSO2 values could be used to provide estimation of SvO2. That fact implicates that peripheral static measurements may not broadly present overall tissue oxygenation compared with frontal rSO2 measurements in septic patients. That fact could be caused by local mismatch of oxygen supply and consumption. Also vasopressor therapy induces vasoconstriction in lower extremities and could influence diagnostic efficiency of thenar rSO2 measurements.
Frontal rSO2 measurement also shows some technical limitations. Because of the short effective measurement range of 2.5 cm NIRS cannot definitely reflect cerebral parenchyma in every single case. Magnetic resonance imaging showed that because of the limited penetration depth cerebral parenchyma in patients with cerebral atrophy could not be reached [40]. It was also shown that high total bilirubin concentrations were independently associated with artificial rSO2 values below 50 % [41, 42].
In addition to the protocol of Rivers et al. [5] for an early goal directed therapy in sepsis, measurements of lactate levels as marker of tissue hypoxia are also recommended [4, 33]. It has also been demonstrated that a significant lag of lactate clearance is associated with increased mortality [9]. These data were confirmed by the findings of this prospective study. In addition, we investigated that septic patients representing increased lactate ≥2.5 mmol/l and ScvO2 ≥70 % had significantly higher mortality (p = 0.004) than patients with normal lactate. Interestingly, at baseline ScvO2 values of the non-survivors were significant increased compared to the survivors. In order to this fact patients representing increased lactate levels and increased ScvO2 represented the highest mortality rate in the study group (80 %). Regarding these findings, the use of ScvO2 as a goal in Rivers early hemodynamic treatment has to be scrutinized. The ProCESS trial revealed in a large randomized, controlled, multicenter study that protocol-based EGDT in patients with septic shock, diagnosed in the emergency department, did not improve outcome [43]. In his editorial, Lilly however claimed early recognition of sepsis, early administration of antibiotics, early adequate volume resuscitation, and clinical assessment of the adequacy of circulation to reduce mortality in patients with sepsis and septic shock [44]. These findings lead to the question if patients really benefit from reaching the target of ScvO2 ≥70 % or if they simply benefit from early source control and treatment of impaired circulatory function in sepsis. Additionally, Asfar et al. [45] found that targeting a higher mean arterial pressure of 80 to 85 mmHg as compared to 65–70 mmHg in patients with septic shock undergoing resuscitation did not reduce mortality. But in a subgroup of patients with hypertension high MAP target decreased the risk of renal injury and the need for renal-replacement therapy [45]. In our study population patients with normal and decreased ScvO2 did not differ according their mean MAP at T1 and reached a relatively high value of about 79 mmHg. However, non-survivor showed significantly lower MAPs than survivor.
The relationship between ScvO2 and lactate has become goal of high interest as a marker of impaired tissue oxygenation. In case of impaired oxygen delivery or increased extraction, consumption becomes delivery dependent and tissues produce lactate according to their transition to anaerobic metabolism. Blood lactate level has been associated with the occurrence of shock and associated organ failure using several organ failure scales and is potentially a reliable marker of persistent occult hypoperfusion [46]. Even Jansen and colleagues claimed lactate as a marker of outcome after severe shock, especially in multiple organ dysfunction syndrome [47]. According to the analysis of Soga et al. [25] who revealed a significant correlation between NIRS-derived variables and the lactate concentration, we doubt that ScvO2 should be the primary therapeutic goal during early resuscitation in sepsis. Even Perz et al. [48] detected that low and also supra-normal ScvO2 values (>77.4 %) in patients undergoing cardiac surgery were associated with raised perioperative complications. In addition, the study revealed that increased lactate level were also associated with low and supra-normal ScvO2 values. The authors concluded that high and low ScvO2 could be under-recognized warning signs for impaired tissue oxygenation. Pope et al. [49] found that in patients with suspected sepsis in the emergency department both abnormally low and high ScvO2 values were associated with increased mortality. Supra-normal ScvO2 in sepsis or systemic inflammation may be a result of disrupted oxygen utilization caused by mitochondrial dysfunction [50, 51]. Nevertheless, even other mechanism beside decreased tissue oxygenation could produce elevated lactate level [52]. Especially increased glycolysis may reflect an important cause of lactate rising. Even inotropic therapy with β-mimetics could cause significant lactate increments [53]. In order to these reasons this observational study may only provide limited mechanistic statements. Also, the power-analysis was performed for the primary aim, the correlation between ScvO2 and rSO2, but not for the value of lactate levels as surrogate for outcome prediction in sepsis. Non-survivor and survivor groups were similar in respiratory conditions, hemoglobin concentration and epinephrine doses. In consideration of these facts we would propose that septic patients representing raised lactate and supra-normal ScvO2 are at high risk for tissue hypoxia and associated raised mortality.
5 Conclusion
In summary, our data revealed that frontal rSO2 correlates with ScvO2 but both frontal and thenar rSO2 do not exactly discriminate between patients with high or low ScvO2 in sepsis. The combination of elevated lactate >2.5 mmol/l and ScvO2 >70 % is highly associated with poor outcome in ICU patients with sepsis, severe sepsis and septic shock.
References
Angus DC, Wax RS. Epidemiology of sepsis: an update. Crit Care Med. 2001;29:S109–16.
Brun-Buisson C, Doyon F, Carlet J, Dellamonica P, Gouin F, Lepoutre A, Mercier JC, Offenstadt G, Regnier B. Incidence, risk factors, and outcome of severe sepsis and septic shock in adults. A multicenter prospective study in intensive care units. French ICU Group for Severe Sepsis. JAMA. 1995;274:968–74.
Pittet D, Rangel-Frausto S, Li N, Tarara D, Costigan M, Rempe L, Jebson P, Wenzel RP. Systemic inflammatory response syndrome, sepsis, severe sepsis and septic shock: incidence, morbidities and outcomes in surgical ICU patients. Intensive Care Med. 1995;21:302–9.
Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, Sevransky JE, Sprung CL, Douglas IS, Jaeschke R, Osborn TM, Nunnally ME, Townsend SR, Reinhart K, Kleinpell RM, Angus DC, Deutschman CS, Machado FR, Rubenfeld GD, Webb S, Beale RJ, Vincent JL, Moreno R. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock, 2012. Intensive Care Med. 2013;39:165–228. doi:10.1007/s00134-012-2769-8.
Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A, Knoblich B, Peterson E, Tomlanovich M. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345:1368–77. doi:10.1056/NEJMoa010307.
Weigand MA, Bardenheuer HJ, Bottiger BW. Clinical management of patients with sepsis. Anaesthesist. 2003;52:3–22. doi:10.1007/s00101-002-0436-0.
Huckabee WE. Abnormal resting blood lactate. I. The significance of hyperlactatemia in hospitalized patients. Am J Med. 1961;30:840–8.
Cowan BN, Burns HJ, Boyle P, Ledingham IM. The relative prognostic value of lactate and haemodynamic measurements in early shock. Anaesthesia. 1984;39:750–5.
Nguyen HB, Rivers EP, Knoblich BP, Jacobsen G, Muzzin A, Ressler JA, Tomlanovich MC. Early lactate clearance is associated with improved outcome in severe sepsis and septic shock. Crit Care Med. 2004;32:1637–42.
Reinhart K, Kuhn HJ, Hartog C, Bredle DL. Continuous central venous and pulmonary artery oxygen saturation monitoring in the critically ill. Intensive Care Med. 2004;30:1572–8. doi:10.1007/s00134-004-2337-y.
Myers DE, Anderson LD, Seifert RP, Ortner JP, Cooper CE, Beilman GJ, Mowlem JD. Noninvasive method for measuring local hemoglobin oxygen saturation in tissue using wide gap second derivative near-infrared spectroscopy. J Biomed Opt. 2005;10:34017. doi:10.1117/1.1925250.
Abdul-Khaliq H, Troitzsch D, Schubert S, Wehsack A, Bottcher W, Gutsch E, Hubler M, Hetzer R, Lange PE. Cerebral oxygen monitoring during neonatal cardiopulmonary bypass and deep hypothermic circulatory arrest. Thorac Cardiovasc Surg. 2002;50:77–81. doi:10.1055/s-2002-26698.
Boushel R, Langberg H, Olesen J, Gonzales-Alonzo J, Bulow J, Kjaer M. Monitoring tissue oxygen availability with near infrared spectroscopy (NIRS) in health and disease. Scand J Med Sci Sport. 2001;11:213–22.
Mulier KE, Skarda DE, Taylor JH, Myers DE, McGraw MK, Gallea BL, Beilman GJ. Near-infrared spectroscopy in patients with severe sepsis: correlation with invasive hemodynamic measurements. Surg Infect. 2008;9:515–9. doi:10.1089/sur.2007.091.
Shapiro NI, Arnold R, Sherwin R, O’Connor J, Najarro G, Singh S, Lundy D, Nelson T, Trzeciak SW, Jones AE. The association of near-infrared spectroscopy-derived tissue oxygenation measurements with sepsis syndromes, organ dysfunction and mortality in emergency department patients with sepsis. Crit Care. 2011;15:R223. doi:10.1186/cc10463.
Baulig W, Dullenkopf A, Kobler A, Baulig B, Roth HR, Schmid ER. Accuracy of continuous central venous oxygen saturation monitoring in patients undergoing cardiac surgery. J Clin Monit Comput. 2008;22:183–8. doi:10.1007/s10877-008-9123-2.
Bhutta AT, Ford JW, Parker JG, Prodhan P, Fontenot EE, Seib PM, Stroope BI, Frazier EA, Schmitz ML, Drummond-Webb JJ, Morrow WR. Noninvasive cerebral oximeter as a surrogate for mixed venous saturation in children. Pediatr Cardiol. 2007;28:34–41. doi:10.1007/s00246-006-1379-z.
Lichtenstern C, Koch C, Rohrig R, Rosengarten B, Henrich M, Weigand MA. Near-infrared spectroscopy in sepsis therapy : predictor of a low central venous oxygen saturation. Anaesthesist. 2012;61:883–91. doi:10.1007/s00101-012-2087-0.
Levy MM, Fink MP, Marshall JC, Abraham E, Angus D, Cook D, Cohen J, Opal SM, Vincent JL, Ramsay G. 2001 SCCM/ESICM/ACCP/ATS/SIS international sepsis definitions conference. Crit Care Med. 2003;31:1250–6. doi:10.1097/01.CCM.0000050454.01978.3B.
Wariar R, Gaffke JN, Haller RG, Bertocci LA. A modular NIRS system for clinical measurement of impaired skeletal muscle oxygenation. J Appl Physiol. 2000;88:315–25.
Wahr JA, Tremper KK, Samra S, Delpy DT. Near-infrared spectroscopy: theory and applications. J Cardiothorac Vasc Anesth. 1996;10:406–18.
De Backer D, Ospina-Tascon G, Salgado D, Favory R, Creteur J, Vincent JL. Monitoring the microcirculation in the critically ill patient: current methods and future approaches. Intensive Care Med. 2010;36:1813–25. doi:10.1007/s00134-010-2005-3.
Creteur J, Carollo T, Soldati G, Buchele G, De Backer D, Vincent JL. The prognostic value of muscle StO2 in septic patients. Intensive Care Med. 2007;33:1549–56. doi:10.1007/s00134-007-0739-3.
Pareznik R, Knezevic R, Voga G, Podbregar M. Changes in muscle tissue oxygenation during stagnant ischemia in septic patients. Intensive Care Med. 2006;32:87–92. doi:10.1007/s00134-005-2841-8.
Soga T, Sakatani K, Yagi T, Kawamorita T, Yoshino A. The relationship between hyperlactatemia and microcirculation in the thenar eminence as measured using near-infrared spectroscopy in patients with sepsis. Emerg Med J. 2013;. doi:10.1136/emermed-2013-202703.
Skarda DE, Mulier KE, Myers DE, Taylor JH, Beilman GJ. Dynamic near-infrared spectroscopy measurements in patients with severe sepsis. Shock. 2007;27:348–53. doi:10.1097/01.shk.0000239779.25775.e4.
Henrich M, Gruß M, Weigand MA. Hämodynamische Veränderungen in der Sepsis. Anaesthesie Intensivmed. 2012;53:19–32.
Shepherd SJ, Pearse RM. Role of central and mixed venous oxygen saturation measurement in perioperative care. Anesthesiology. 2009;111:649–56. doi:10.1097/ALN.0b013e3181af59aa.
Maddirala S, Khan A. Optimizing hemodynamic support in septic shock using central and mixed venous oxygen saturation. Crit Care Clin. 2010;26:323–33. doi:10.1016/j.ccc.2009.12.006.
Maillet J-M, Le Besnerais P, Cantoni M, Nataf P, Ruffenach A, Lessana A, Brodaty D. Frequency, risk factors, and outcome of hyperlactatemia after cardiac surgery. Chest. 2003;123:1361–6.
Pölönen P, Ruokonen E, Hippeläinen M, Pöyhönen M, Takala J. A prospective, randomized study of goal-oriented hemodynamic therapy in cardiac surgical patients. Anesth Analg. 2000;90:1052–9.
Smith I, Kumar P, Molloy S, Rhodes A, Newman PJ, Grounds RM, Bennett ED. Base excess and lactate as prognostic indicators for patients admitted to intensive care. Intensive Care Med. 2001;27:74–83.
Reinhart K, Brunkhorst FM, Bone HG, Bardutzky J, Dempfle CE, Forst H, Gastmeier P, Gerlach H, Grundling M, John S, Kern W, Kreymann G, Kruger W, Kujath P, Marggraf G, Martin J, Mayer K, Meier-Hellmann A, Oppert M, Putensen C, Quintel M, Ragaller M, Rossaint R, Seifert H, Spies C, Stuber F, Weiler N, Weimann A, Werdan K, Welte T (2010) Prevention, diagnosis, therapy and follow-up care of sepsis: 1st revision of S-2 k guidelines of the German Sepsis Society (Deutsche Sepsis-Gesellschaft e.V. (DSG)) and the German Interdisciplinary Association of Intensive Care and Emergency Medicine (Deut. Ger Med Sci 8:Doc14. doi: 10.3205/000103.
Casati A, Fanelli G, Pietropaoli P, Proietti R, Tufano R, Danelli G, Fierro G, Fierro G, De Cosmo G, Servillo G. Continuous monitoring of cerebral oxygen saturation in elderly patients undergoing major abdominal surgery minimizes brain exposure to potential hypoxia. Anesth Analg. 2005;101:740–7. doi:10.1213/01.ane.0000166974.96219.cd.
Janelle GM, Mnookin S, Gravenstein N, Martin TD, Urdaneta F. Unilateral cerebral oxygen desaturation during emergent repair of a DeBakey type 1 aortic dissection: potential aversion of a major catastrophe. Anesthesiology. 2002;96:1263–5.
Murkin JM, Adams SJ, Novick RJ, Quantz M, Bainbridge D, Iglesias I, Cleland A, Schaefer B, Irwin B, Fox S. Monitoring brain oxygen saturation during coronary bypass surgery: a randomized, prospective study. Anesth Analg. 2007;104:51–8. doi:10.1213/01.ane.0000246814.29362.f4.
Podbregar M, Mozina H. Skeletal muscle oxygen saturation does not estimate mixed venous oxygen saturation in patients with severe left heart failure and additional severe sepsis or septic shock. Crit Care. 2007;11:R6. doi:10.1186/cc5153.
Leone M, Blidi S, Antonini F, Meyssignac B, Bordon S, Garcin F, Charvet A, Blasco V, Albanese J, Martin C. Oxygen tissue saturation is lower in nonsurvivors than in survivors after early resuscitation of septic shock. Anesthesiology. 2009;111:366–71. doi:10.1097/ALN.0b013e3181aae72d.
Mesquida J, Masip J, Gili G, Artigas A, Baigorri F. Thenar oxygen saturation measured by near infrared spectroscopy as a noninvasive predictor of low central venous oxygen saturation in septic patients. Intensive Care Med. 2009;35:1106–9. doi:10.1007/s00134-009-1410-y.
Zanatta P, Forti A. Effectiveness of NIRS to sample the frontal brain cortex in all cardiac surgery patients. Minerva Anestesiol. 2011;77:1124–5.
Madsen PL, Skak C, Rasmussen A, Secher NH. Interference of cerebral near-infrared oximetry in patients with icterus. Anesth Analg. 2000;90:489–93.
Song J-G, Jeong S-M, Shin W-J, Jun I-G, Shin K, Huh I-Y, Kim Y-K, Hwang G-S. Laboratory variables associated with low near-infrared cerebral oxygen saturation in icteric patients before liver transplantation surgery. Anesth Analg. 2011;112:1347–52. doi:10.1213/ANE.0b013e318214b2b0.
Yealy DM, Kellum JA, Huang DT, Barnato AE, Weissfeld LA, Pike F, Terndrup T, Wang HE, Hou PC, LoVecchio F, Filbin MR, Shapiro NI, Angus DC. A randomized trial of protocol-based care for early septic shock. N Engl J Med. 2014;370:1683–93. doi:10.1056/NEJMoa1401602.
Lilly CM. The process trial—a new era of sepsis management. N Engl J Med. 2014;370:1750–1. doi:10.1056/NEJMe1402564.
Asfar P, Meziani F, Hamel J-F, Grelon F, Megarbane B, Anguel N, Mira J-P, Dequin P-F, Gergaud S, Weiss N, Legay F, Le Tulzo Y, Conrad M, Robert R, Gonzalez F, Guitton C, Tamion F, Tonnelier J-M, Guezennec P, Van Der Linden T, Vieillard-Baron A, Mariotte E, Pradel G, Lesieur O, Ricard J-D, Hervé F, du Cheyron D, Guerin C, Mercat A, Teboul J-L, Radermacher P. High versus low blood-pressure target in patients with septic shock. N Engl J Med. 2014;370:1583–93. doi:10.1056/NEJMoa1312173.
Bakker J, Gris P, Coffernils M, Kahn RJ, Vincent JL. Serial blood lactate levels can predict the development of multiple organ failure following septic shock. Am J Surg. 1996;171:221–6. doi:10.1016/S0002-9610(97)89552-9.
Jansen TC, van Bommel J, Woodward R, Mulder PGH, Bakker J. Association between blood lactate levels, sequential organ failure assessment subscores, and 28-day mortality during early and late intensive care unit stay: a retrospective observational study. Crit Care Med. 2009;37:2369–74. doi:10.1097/CCM.0b013e3181a0f919.
Perz S, Uhlig T, Kohl M, Bredle DL, Reinhart K, Bauer M, Kortgen A. Low and “supranormal” central venous oxygen saturation and markers of tissue hypoxia in cardiac surgery patients: a prospective observational study. Intensive Care Med. 2011;37:52–9. doi:10.1007/s00134-010-1980-8.
Pope JV, Jones AE, Gaieski DF, Arnold RC, Trzeciak S, Shapiro NI. Multicenter study of central venous oxygen saturation (ScvO2) as a predictor of mortality in patients with sepsis. Ann Emerg Med. 2010;55(40–46):e1. doi:10.1016/j.annemergmed.2009.08.014.
Ince C, Sinaasappel M. Microcirculatory oxygenation and shunting in sepsis and shock. Crit Care Med. 1999;27:1369–77.
Crouser ED. Mitochondrial dysfunction in septic shock and multiple organ dysfunction syndrome. Mitochondrion. 2004;4:729–41. doi:10.1016/j.mito.2004.07.023.
Bakker J, Coffernils M, Leon M, Gris P, Vincent JL. Blood lactate levels are superior to oxygen-derived variables in predicting outcome in human septic shock. Chest. 1991;99:956–62.
Levy B. Lactate and shock state: the metabolic view. Curr Opin Crit Care. 2006;12:315–21. doi:10.1097/01.ccx.0000235208.77450.15.
Conflict of interest
The authors declare that they have no conflict of interest. Authors did not receive funding or any other kind of financial support.
Ethical standard
Ethical approval for this study (ethics proposal number AZ 57/12) was obtained from the Ethics Committee of the Faculty of Medicine at the Justus-Liebig-University Giessen, Giessen, Germany (Chairman Prof. H. Tillmanns) on 12 June 2012. Patients or their legal representative gave written informed consent before study inclusion.
Author information
Authors and Affiliations
Corresponding author
Additional information
Trial registration: www.germanctr.de identifier: DRKS00003327.
Rights and permissions
About this article

Cite this article
Koch, C., Röhrig, R., Monz, T. et al. Prospective evaluation of regional oxygen saturation to estimate central venous saturation in sepsis. J Clin Monit Comput 29, 443–453 (2015). https://doi.org/10.1007/s10877-015-9683-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10877-015-9683-x