
Abstract
Purpose
To examine the effect of low and very low estradiol responses in oocyte donors receiving gonadotropins on clinical outcomes of donor in vitro fertilization (IVF) cycles and to identify possible mechanisms responsible for low estradiol response.
Methods
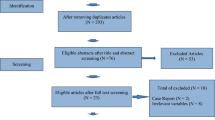
This is a retrospective cohort study of oocyte donors undergoing antagonist IVF cycles with progression to oocyte retrieval between January 2010 and December 2016 at a single urban academic fertility center. Oocyte yield, fertilization rate, blastocyst rate, percentage of normal embryos on preimplantation genetic screening (PGS), pregnancy outcomes, and follicular fluid steroid profiles were compared between donors with normal estradiol response and those with low estradiol response.
Results
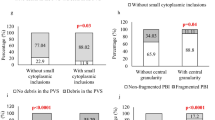
Three hundred sixty-six antagonist oocyte donor IVF cycles were identified: 42 cycles had a normal estradiol response (NE2), defined as peak serum estradiol (E2) of over 200 pg/mL per retrieved oocyte; 140 cycles had an intermediate estradiol response (iE2), defined as peak serum E2 between 100 and 200 pg/mL per retrieved oocyte; 110 cycles had a low estradiol response (LE2), defined as peak serum E2 between 50 and 100 pg/mL per retrieved oocyte; and 74 cycles had a very low estradiol response (vLE2), defined as peak serum E2 less than 50 pg/mL per retrieved oocyte. LE2 cycles resulted in a greater number of mature oocytes (22.4 vs. 13.6, p < 0.017), and fertilizations versus NE2 donors (18.5 vs. 10.7, p < 0.017), although the number of transferred or cryopreserved blastocysts were similar between groups (8.6, 6.9 vs. 4.8, p = 0.095, p = 1). The percentage of chromosomally normal embryos after PGS was similar between LE2, vLE2, and NE2 cycles (66.4, 71.8 vs. 63.1%, p = 0.99, p = 1). Pregnancy outcomes were similar between LE2, vLE2, and NE2 cycles. Serum AMH obtained on the day of peak E2 was similar to baseline serum AMH and did not differ between LE2 versus NE2 cycles. Follicular fluid E2 levels paralleled serum E2 levels and were lower in LE2 cycles versus NE2 cycles.
Conclusion
The prevalence of very low E2 responses in donors appears to be high (20.2%). In contrast to autologous IVF cycles, LE2 does not portend poor outcomes in oocyte donors.


Similar content being viewed by others

References
Fritz M, Speroff L. Clinical gynecologic endocrinology and infertility. 8th ed. Philadelphia: Lippincott Williams & Wilkins; 2011.
Mittal S, Gupta P, Malhotra N, Singh N. Serum estradiol as a predictor of success of in vitro fertilization. J Obstet Gynaecol India. 2014;64:124–9.
Hu X, Luo Y, Huang K, Li Y, Xu Y, Zhou C, et al. New perspectives on criteria for the determination of HCG trigger timing in GnRH antagonist cycles. Medicine. 2016;95:e3691.
Centers for Disease Control and Prevention, American Society for Reproductive Medicine, Society for Assisted Reproductive Technology. 2014 assisted reproductive technology national summary report: Atlanta; 2016.
Orvieto R, Zohav E, Scharf S, et al. The influence of estradiol/follicle and estradiol/oocyte ratios on the outcome of controlled ovarian stimulation for in vitro fertilization. Gynecol Endocrinol. 2007;23:72–5.
Yang J, Chen H, Lien Y, Chen S, Ho H, Yang Y. Elevated E2: oocyte ratio in women undergoing IVF and tubal ET. Correlation with a decrease in the implantation rate. J Reprod Med. 2001;46:434–8.
Vaughan DA, Harrity C, Sills ES, Mocanu EV. Serum estradiol:oocyte ratio as a predictor of reproductive outcome: an analysis of data from >9000 IVF cycles in the Republic of Ireland. J Assist Reprod Genet. 2016;33:481–8.
Haas J, Baum M, Meridor K, Hershko-Klement A, Elizur S, Hourvitz A, et al. Is severe OHSS associated with adverse pregnancy outcomes? Evidence from a case-control study. Reprod BioMed Online. 2014;29:216–21.
Raziel A, Friedler S, Schachter M, Strassburger D, Mordechai E, Ron-El R. Increased early pregnancy loss in IVF patients with severe ovarian hyperstimulation syndrome. Hum Reprod. 2002;17:107–10.
Karlsson MO, Wade JR, Loumaye E, Munafo A. The population pharmacokinetics of recombinant- and urinary-human follicle stimulating hormone in women. Br J Clin Pharmacol. 1998;45:13–20.
Kim J, Lee J, Chang H, Jee B, Suh C, Kim S. Anti-Mullerian hormone levels in the follicular fluid of the preovulatory follicle: a predictor for oocyte fertilization and quality of embryo. J Korean Med Sci. 2014;29:1266–70.
Seifer D, Maclaughlin D. Mullerian inhibiting substance is an ovarian growth factor of emerging clinical significance. Fertil Steril. 2007;88:539–46.
Vet AD, Laven J, Jong FD, Themmen A, Fauser B. Antimullerian hormone serum levels: a putative marker for ovarian aging. Fertil Steril. 2002;77:357–62.
Seifer D, MacLaughlin D, Christian B, Feng B, Shelder R. Early follicular serum mullerian-inhibiting substance levels are associated with ovarian response during assisted reproductive technology cycles. Fertil Steril. 2002;77:468–71.
van Rooij IA, Broekmans FJ, te Velde ER, et al. Serum anti-Mullerian hormone levels: a novel measure of ovarian reserve. Hum Reprod. 2002;17:3065–71.
Lee J, Kim S, Kim S, et al. Anti-Mullerian hormone dynamics during controlled ovarian hyperstimulation and optimal timing of measurement for outcome prediction. Hum Reprod. 2010;25:2597–604.
Silberstein T, MacLaughlin D, Shai I, et al. Mullerian inhibiting substance levels at the time of HCG administration in IVF cycles predict both ovarian reserve and embryo morphology. Hum Reprod. 2006;21:159–63.
Takahashi C, Fujito A, Kazuka M, Sugiyama R, Ito H, Isaka K. Anti-Mullerian hormone substance from follicular fluid is positively associated with success in oocyte fertilization during in vitro fertilization. Fertil Steril. 2008;89:586–91.
Fanchin R, Lozano DM, Frydman N, et al. Anti-Mullerian hormone concentrations in the follicular fluid of the preovulatory follicle are predictive of the implantation potential of the ensuing embryo obtained by in vitro fertilization. J Clin Endocrinol Metab. 2007;92:1796–802.
Li L, Ferin M, Sauer M, Lobo R. Dehydroepiandrosterone in follicular fluid is produced locally, and levels correlate negatively with in vitro fertilization outcomes. Fertil Steril. 2011;95:1830–2.
Li L, Ferin M, Sauer M, Lobo R. Serum and follicular fluid ghrelin levels negatively reflect human oocyte quality and in vitro embryo development. Fertil Steril. 2011;96:1116–20.
Foong S, Abbott D, Lesnick T, Session D, Walker D, Dumesic D. Diminished intrafollicular estradiol levels in in vitro fertilization cycles from women with reduced ovarian response to recombinant human follicle-stimulating hormone. Fertil Steril. 2005;83:1377–83.
de los Santos MJ, Garcia-Laez V, Beltran-Torregrosa D, et al. Hormonal and molecular characterization of follicular fluid, cumulus cells and oocytes from pre-ovulatory follicles in stimulated and unstimulated cycles. Hum Reprod. 2012;27:1596–605.
Rodgers RJ, Reid GD, Koch J, Deans R, Ledger WL, Friedlander M, et al. The safety and efficacy of controlled ovarian hyperstimulation for fertility preservation in women with early breast cancer: a systematic review. Hum Reprod. 2017;32:1033–45.
Bianchi PH, Gouveia GR, Costa EM, et al. Successful live birth in a woman with 17alpha-hydroxylase deficiency through IVF frozen-thawed embryo transfer. J Clin Endocrinol Metab. 2016;101:345–8.
Kitajima M, Miura K, Inoue T, et al. Two consecutive successful live birth in woman with 17alpha hydroxylase deficiency by frozen-thaw embryo transfer under hormone replacement endometrium preparation. Gynecol Endocrinol. 2017;34:1–4.
Acknowledgements
The authors would like to acknowledge Michel Ferin, Nancy Cotui, and Kimberly Hamroff for their expertise and assistance with conducting all serum and follicular fluid hormone assays. The authors also acknowledge the CUFC Embryology Division for their assistance in facilitating follicular fluid collection.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Electronic supplementary material
ESM 1
(DOCX 15 kb)
Rights and permissions
About this article

Cite this article
Palmerola, K.L., Rudick, B.J. & Lobo, R.A. Low estradiol responses in oocyte donors undergoing gonadotropin stimulation do not influence clinical outcomes. J Assist Reprod Genet 35, 1675–1682 (2018). https://doi.org/10.1007/s10815-018-1192-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10815-018-1192-7