
Abstract
Background
Death after endoscopy is rare, under-reported, and has variable causes. This study aimed to evaluate the incidence and causes of fatal endoscopic adverse events (AEs) across two academic medical centers and to identify patient-, procedure-, and sedation-related risk factors.
Methods
This is a retrospective cohort study of fatal adverse events causally related to endoscopy at Denver Health Medical Center and the University of Colorado Hospital from 2011 to 2020. Fatal AEs were retrieved from the physician-reported database. Electronic medical records were then reviewed to determine medical history, procedure details, subsequent treatments, and time and cause of death.
Results
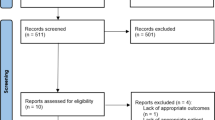
From January 2011 to January 2020, 146,010 GI endoscopy procedures were performed. Median patient age was 70 [51–78] and 57% were male. Thirty-one deaths were identified, 28 of which were attributed to endoscopy, yielding a procedure-related fatality rate of 0.018%. Procedures included 11 EGDs, one colonoscopy, two flexible sigmoidoscopies, six ERCPs, seven upper EUS, and one PEG-J tube placement. Specific causes of death included aspiration in four patients (14%); cardiac arrest or myocardial infarction in seven patients (25%); perforation in nine patients (32%); bleeding in four patients (14%); cholangitis or sepsis without perforation in three patients (11%); and acute pancreatitis in one patient (3.6%).
Conclusions
Fatal endoscopic AEs were rare but tended to occur in older patients with major comorbidities. Most deaths occurred from aspiration pneumonia, cardiac arrest, or perforation-related sepsis within 1 week of the procedure.



Similar content being viewed by others


References
Ben-Menachem T, Decker GA, Early DS et al. Adverse events of upper GI endoscopy. Gastrointest Endosc. 2012;76:707–718.
Kothari ST, Huang RJ, Shaukat A et al. ASGE review of adverse events in colonoscopy. Gastrointest Endosc. 2019;90:863–876.e33.
Early DS, Acosta RD, Chandrasekhara V et al. Adverse events associated with EUS and EUS with FNA. Gastrointest Endosc. 2013;77:839–843.
Talukdar R. Complications of ERCP. Best Pract Res Clin Gastroenterol. 2016;30:793–805.
Eisen GM, Baron TH, Dominitz JA et al. Role of endoscopy in enteral feeding. Gastrointest Endosc. 2002;55:794–797.
Ko CW, Dominitz JA. Complications of colonoscopy: magnitude and management. Gastrointest Endosc Clin N Am. 2010;20:659–671.
Masci E, Toti G, Mariani A et al. Complications of diagnostic and therapeutic ERCP: a prospective multicenter study. Am J Gastroenterol. 2001;96:417–423.
tenBerge J, Hoffman BJ, Hawes RH et al. EUS-guided fine needle aspiration of the liver: indications, yield, and safety based on an international survey of 167 cases. Gastrointest Endosc. 2002;55:859–862.
Zhu H, Jiang F, Zhu J et al. Assessment of morbidity and mortality associated with endoscopic ultrasound-guided fine-needle aspiration for pancreatic cystic lesions: a systematic review and meta-analysis. Dig Endosc. 2017;29:667–675.
Sharma VK, Nguyen CC, Crowell MD et al. A national study of cardiopulmonary unplanned events after GI endoscopy. Gastrointest Endosc. 2007;66:27–34.
Christensen M, Matzen P, Schulze S et al. Complications of ERCP: a prospective study. Gastrointest Endosc. 2004;60:721–731.
Fugazza A, Sethi A, Trindade AJ et al. International multicenter comprehensive analysis of adverse events associated with lumen-apposing metal stent placement for pancreatic fluid collection drainage. Gastrointest Endosc. 2020;91:574–583.
Drossman DA, Brandt LJ, Sears C et al. A preliminary study of patients’ concerns related to GI endoscopy. Am J Gastroenterol. 1996;91:287–291.
Hedenbro JL, Lindblom A. Patient attitudes to sedation for diagnostic upper endoscopy. Scand J Gastroenterol. 1991;26:1115–1120.
Zubarik R, Eisen G, Mastropietro C et al. Prospective analysis of complications 30 days after outpatient upper endoscopy. Am J Gastroenterol. 1999;94:1539–1545.
Zubarik R, Fleischer DE, Mastropietro C et al. Prospective analysis of complications 30 days after outpatient colonoscopy. Gastrointest Endosc. 1999;50:322–328.
Sieg A, Hachmoeller-Eisenbach U, Eisenbach T. Prospective evaluation of complications in outpatient GI endoscopy: a survey among German gastroenterologists. Gastrointest Endosc. 2001;53:620–627.
Gress FG, Hawes RH, Savides TJ et al. Endoscopic ultrasound-guided fine-needle aspiration biopsy using linear array and radial scanning endosonography. Gastrointest Endosc. 1997;45:243–250.
Eloubeidi MA, Tamhane A, Varadarajulu S et al. Frequency of major complications after EUS-guided FNA of solid pancreatic masses: a prospective evaluation. Gastrointest Endosc. 2006;63:622–629.
Siddiqui AA, Adler DG, Nieto J et al. EUS-guided drainage of peripancreatic fluid collections and necrosis by using a novel lumen-apposing stent: a large retrospective, multicenter U.S. experience (with videos). Gastrointest Endosc. 2016;83:699–707.
Sealock RJ, Othman M, Das K. Endoscopic diagnosis and treatment of gastrointestinal trauma. Clin Gastroenterol Hepatol. 2021;19:14–23.
Wichmann D, Stüker D, Schempf U et al. Endoscopic negative pressure therapy with open-pore film drainage and open-pore polyurethane sponge drainage for iatrogenic perforation of the esophagus. Endoscopy. 2020;52:377–382.
Freeman ML, Nelson DB, Sherman S et al. Complications of endoscopic biliary sphincterotomy. N Engl J Med. 1996;335:909–919.
Higa JT, Choe J, Tombs D et al. Optimizing duodenoscope reprocessing: rigorous assessment of a culture and quarantine protocol. Gastrointest Endosc. 2018;88:223–229.
Rahman MR, Perisetti A, Coman R et al. Duodenoscope-associated infections: update on an emerging problem. Dig Dis Sci. 2019;64:1409–1418. https://doi.org/10.1007/s10620-018-5431-7.
Thaker AM, Muthusamy VR, Sedarat A et al. Duodenoscope reprocessing practice patterns in U.S. endoscopy centers: a survey study. Gastrointest Endosc. 2018;88:316–322.e2.
Kochar B, Akshintala VS, Afghani E et al. Incidence, severity, and mortality of post-ERCP pancreatitis: a systematic review by using randomized, controlled trials. Gastrointest Endosc. 2015;81:143–149.e9.
Funding
This study received no internal or external funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Formal consent
For this type of (retrospective) study, formal consent is not required.
Animal contact
This article does not contain any studies with animals performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Swei, E., Heller, J.C., Scott, F. et al. Adverse Event Fatalities Related to GI Endoscopy. Dig Dis Sci 67, 1753–1760 (2022). https://doi.org/10.1007/s10620-021-06981-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-021-06981-9