
Abstract
Parent–child communication represents an important variable in clinical child and family psychology due to its association with a variety of psychosocial outcomes. To give an overview of instruments designed to measure the quality of parent–child communication from the child’s (8–21 years) perspective and to assess the psychometric quality of these instruments, we performed a systematic literature search in Medline and PsycInfo (last: February 25, 2022). Peer-reviewed journal articles published in English with a child-rated instrument measuring the quality of parent–child communication were included. Initial screening for eligibility and inclusion, subsequent data extraction, and quality assessment were conducted by couples of review team members. Based on the screening of 5115 articles, 106 studies reported in 126 papers were included. We identified 12 parent–child communication instruments across the studies. The Parent-Adolescent Communication Scale (PACS) was used in 75% of the studies. On average, the evidence for psychometric quality of the instruments was low. Few instruments were used in clinical and at-risk samples. Several instruments are available to rate parent–child communication from the child’s perspective. However, their psychometric evidence is limited and the theoretical foundation is largely undocumented. This review has limitations with regard to selection criteria and language bias.
Registration PROSPERO: CRD42021255264.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Parent–child communication is a fundamental component of family functioning, both from an empirical (e.g., Liu, 2003; Ochoa et al., 2007) and a conceptual perspective (e.g., Estlein, 2021; Papini et al., 1990; Stamp, 2004). Even before a child is born, parents respond to the child’s signals from the womb. This communication marks the start of an enduring interactional process in which children and parents mutually influence each other to create a relational bond that constitutes the child’s inner working model for social relations (Dixson, 1995). The quality of the parent–child communication has been found to influence multiple psychosocial outcomes. At the child level, these factors include socio-relational factors such as peer competence and conflict management (Branje, 2008; Carson et al., 1999), academic factors such as school readiness and performance (Noller & Feeney, 2004), socio-cognitive factors such as moral reasoning, self-esteem, self-development, and individuation (e.g., Arnett, 1999; Grotevant, 2001; McLean et al., 2007), resiliency, and happiness (e.g., Fitzpatrick & Koerner, 2005; Jackson et al., 1998); as well as psychosocial adjustment and mental health (e.g., Davidson & Cardemil, 2009; Houck et al., 2007; Park & Koo, 2009). There is also evidence of longitudinal effects, with a study showing that lack of parent–child communication at age 10 years predicted depression 20 years later (Lindeloew, 1999). Since parent–child communication influences these outcomes from birth to young adulthood, we use the term “child” in the current review with reference to the relationship to the parent, not to a specific age or developmental stage.
At the family level, factors associated with parent–child communication include family relationship quality (Barnes & Olson, 1985), family functioning, adaptability, and cohesion (Koerner & Fitzpatrick, 2002; Schrodt, 2005; Sillars et al., 2014), family satisfaction (Jackson et al., 1998), conflict avoidance (Koerner & Fitzpatrick, 1997), reticence (Kelly et al., 2002), and problem-solving (Olson et al., 1979). Whereas some of the relations between parent–child communication and other variables are assumed to be direct, parent–child communication is also proposed as a potential intermediate variable in predicting child mental health from other variables, such as maternal depressive symptoms (McCarty et al., 2003). Given the importance of parent–child communication for child outcomes, the field needs high-quality parent–child communication measures. The current study aims to provide a quality-based review of such measures.
In determining the optimal ways to measure parent–child communication, multiple methodological issues need to be considered. The first relates to how parent–child communication is conceptualized. The term “communication” represents a wide and varied construct that is difficult to define comprehensively across theories (Krauss & Fussell, 1996). Interpersonal communication composes both speech and non-speech-message aspects and includes a focus on interaction patterns and difficulties, social support, verbal confirmation, boundary management, speech accommodation, self-disclosure, nonverbal cues, and secrets (Vangelisti & Caughlin, 1997). As far as interpersonal communication in the family is concerned, it usually comprises verbal and nonverbal two-way interactions that express feelings, thoughts, values, and needs (Satir, 1988). This basic definition is the basis for multiple operational definitions. Parent–child communication has been conceptualized as an indicator of relationship quality (Huizinga et al., 2005), but also as a routine interaction that defines and shapes parent–child relationships (Dixson, 1995). Because parent–child communication is tightly associated with other psychosocial measures, some researchers may choose to examine parent–child communication through related terms such as relationship quality, attachment, or parenting styles (Feddern Donbaek & Elklit, 2014; Moilanen et al., 2018). The field needs clarification concerning what should be considered the core components of parent–child communication.
A second and related methodological issue is the theoretical basis for parent–child communication. Parent–child communication can be placed in multiple theoretical frameworks, such as social learning theory, attachment theory, family systems theory, role theory, and family process theory (Stamp, 2004). Theoretical plurality is beneficial to the field, and theory development is a constant process within child and family psychology. At the same time, increased awareness of the theoretical background of existing measures would help to bring clarity to the field and provide directions for future research and theory development.
A third methodological issue when considering how to measure parent–child communication is whose perspective this variable should be measured from. At least three perspectives are relevant, i.e., the child, the parent, and potential observers. Empirical knowledge indicates that these perspectives tend to be moderately correlated at best (e.g., Guilamo-Ramos et al., 2006; Hartos & Power, 2000a, 2000b; Hadley et al., 2013). This does not imply that one perspective is more “correct” than the other, but rather reflects the fact that parent–child communication, like many other child psychosocial variables (e.g., mental health symptoms), looks different from different viewpoints (De los Reyes & Kazdin, 2005). This phenomenon is linked to attribution theory and actor-observer differences and should not be considered measurement error (De los Reyes & Kazdin, 2005). However, it is evident that practitioners and researchers need to carefully consider whose rater perspective is optimal for the concept they aim to examine. For example, measuring parent–child communication from an observer’s perspective may be useful if the aim is to identify objectively measurable communication components such as eye contact, gestures, and voice pitch. In contrast, the parental perspective may be of special interest if the parent’s perception of parent–child communication is assumed to relate to parental mental health. However, if the main aim is to examine how parent–child communication is related to the child’s psychosocial functioning, the child’s own perspective may be most useful due to common-rater variance (Achenbach et al., 1987). In the current review, we focus on child-rated measures. There are five main reasons for this. The first reason is related to theoretical perspectives concerning parent–child communication rater overlap. The generational stake theory (Acock & Bengtson, 1980) suggests that parents and children have different psychological needs and different investments in establishing the generational bond due to representing contrasting generations. Whereas parents may invest more in maximizing and maintaining intergenerational continuity, children may be more prone to seek separate identities and therefore emphasize and exaggerate conflicts and differences with parents more. Based on this theoretical perspective, focusing on the child perspective on parent–child communication may be particularly important. A second reason to focus on child-rated measures is that children’s subjective communication experience is likely to be more relevant to assess family functioning and other child-related psychosocial variables (Kapetanovic & Boson, 2022; Xiao et al., 2011). Third, the child perspective may also be more relevant for child-focused intervention planning, as observer-rated data may not converge with how family members assess the situation (Noller & Feeney, 2004). Reviews have shown that the child’s own perspective and children’s active involvement in research about their psychosocial situation is largely under-utilized (e.g., Facca et al., 2020; Larsson et al., 2018). Hence, a fourth reason to focus on child-rated measures is that this may promote the use of children as informants in research. The final reason relates to relevance for the practice field. Self-report questionnaires are more accessible and less resource-demanding to administer than observer-rated measures. Providing an overview of easy-to-administer child-rated measures will thus have high relevance for the practice field.
A fourth methodological issue to consider is the scope or focus of the parent–child communication measure. Definitions of parent–child communication are wide and varied (Vangelisti & Caughlin, 1997), which opens up several measurement angles. Measures can be focused on topics [e.g., sexuality (Sales et al., 2008), health behavior (Miller-Day & Kam, 2010), conflicts (Peterson, 1990)], and/or situations/settings [e.g., home, laboratory (Hadley et al., 2013)], and/or refer to the general quality of parent–child communication (Barnes & Olson, 1982). In addition, measures can address dyadic communication between the child and one parent or triadic communication between the child and both parents. Furthermore, measures can focus on communication quality, frequency, or a combination of these (Miller-Day & Kam, 2010; Xin et al., 2021). A related issue is the time perspective of the measure, i.e., concurrent, prospective, or retrospective. In the current review, our interest lies in measures of parent–child communication that are widely applicable, especially with regard to child mental health and development. Therefore, we focus on the quality of current general parent–child communication and, if subscales are provided, their specific features.
Finally, measures can be tailored for different populations. Whereas some measures are meant for the general population, others are tailored for ethnic groups, nationalities, or age groups. In the current review, we focus on measures for the general child population that can be applied to clinical and at-risk populations as well. “Clinical” indicates that the child has been diagnosed with a mental health or somatic disorder, whereas “at-risk” indicates that the sample was selected according to criteria that are considered as a transitory or continuous risk for child mental health such as being a minority or being bereaved.
The aim of the current study is to provide the field with an overview of existing instruments that measure the quality of parent–child communication from the child’s (8–21 years) perspective. We will consider the psychometric properties of the scales using criteria based on De los Reyes and Langer (2018). We investigated the following research questions: Which child-report questionnaires exist to measure parent–child communication, what kind of samples have they been applied to, and what is their psychometric quality? We will also consider the instruments’ availability, including translations and norms, to ease the decision-making processes for practitioners and researchers who aim to measure parent–child communication.
Methods
We conducted this systematic review according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2021). We searched the PROSPERO database initially to ensure that no similar studies had been started or planned and published a protocol for this study under the number: CRD42021255264.
Eligibility Criteria
The eligibility criteria were as follows: original, peer-reviewed journal articles published in English language and assessing the quality of general communication between parents and their children via multi-item scales for child self-report were included. In the context of this review, communication included verbal, nonverbal, cognitive, and affective aspects of the interaction between parents and their children, but not the physical ability to communicate. Studies assessing broader concepts such as general family communication or studies using single questions or ad-hoc measures to assess parent–child communication were excluded, just as studies on specific topics of communication such as health-related behaviors (e.g., sex, alcohol, tobacco use). Studies reporting only parent ratings were excluded.
The age range of the study population was set at 8 to 21 years of age, including older children, adolescents, and emerging adults. We included studies examining parent–child communication in general, clinical (both somatic and mental health), and at-risk populations. In terms of study design, we included all types of empirical studies (cross-sectional, longitudinal, interventional, validation studies). Qualitative studies and case reports were excluded.
Information Sources and Search Strategy
We conducted the main search and selection process between May 2021 and October 2021, identifying original studies by searching the electronic databases APA PsycInfo (Ovid) and MEDLINE (Ovid). On February 25, 2022, an updated search for papers published after the initial search was conducted and resulted in the addition of nine reports. The references of all selected publications were searched for additional studies. We included additional sources on psychometric data in our assessment of psychometric quality if it was referred to in one of the publications and available in English. Table 1 presents the search strategy used via the Ovid database. A librarian was consulted to develop and improve the search strategy.
Selection Process
Bibliographical data were uploaded to Rayyan (rayyan.ai) for masked screening. Pairs of team members (HZ, KF, JB, SC, SO, YH) screened titles and abstracts. Full-texts retrieved after screening were checked for eligibility by the same pairs independently, again using Rayyan. Disagreements were resolved by discussion.
Data Collection Process and Data Items
Data items extracted from the studies were scale name, sample description, child sample age, sampling strategy, the focus of the paper, main method, relation of parent–child communication to other constructs, and main results about parent–child communication. To conduct the quality assessments, reported psychometric properties were also extracted (see results section). Multiple reports from a study/sample were treated as a single study. Data were extracted by KF, SO, SC, YH, and JB. All extracted data were completely cross-checked by HZ.
Quality Assessment
In our evaluation of instrument quality, we relied on the criteria set forward by Hunsley and Mash (2007, 2008, 2018), complemented by Youngstrom et al. (2017), and summarized in De los Reyes and Langer (2018). This system is used to rate the psychometric properties of assessment instruments across nine categories: (a) norms, (b) internal consistency, (c) interrater reliability, (d) test–retest reliability, (e) content validity, (f) construct validity, (g) validity generalization, (h) treatment sensitivity, and (i) clinical utility. Each category includes a description of the quality of evidence required for a rating of adequate (minimal level of scientific rigor), good (solid scientific support), or excellent (extensive, high-quality support). Youngstrom et al. (2017) later added repeatability, discriminative validity, and prescriptive validity to the original system. Since the original system was intended for clinical measures, not all categories apply to parent–child communication scales. Thus, in the current review, we rated the following nine quality categories: norms, internal consistency, test–retest reliability, content validity, construct validity, factorial structure, discriminative validity, validity generalization, and treatment sensitivity (See Supplement Table).
In terms of norms, there are no clear cut-offs for sample size, but we considered community samples N > 400 and clinical samples N > 100 as representative. In terms of reliability, the system applies the following criteria for Chronbach’s α: 0.70—0.79 is adequate, 0.80 to 0.89 is good, and > 0.90 is excellent, based on the median of reported numbers. The quality assessment was conducted by KF, SO, SC, YH, and JB, as well as cross-checked by SC and HZ. If members of the review team had co-authored a paper under consideration, the other team members did the quality assessment.
Results
Study Selection
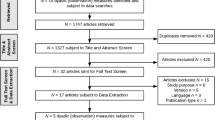
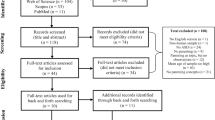
A total of 6147 hits were retrieved from the databases, and 1032 duplicates were removed. Based on the screening of the remaining 5115 titles and abstracts, 499 full-texts were retrieved. Based on these we included 118 papers. In addition, reference lists were searched for eligible literature, resulting in 32 papers of which 28 were retrieved. Eight additional papers were included, resulting in 126 papers in total. Figure 1 shows the corresponding PRISMA flow chart. Table 2 provides an overview of included articles.

PRISMA flow diagram according to Page et al. (2021)
Study Characteristics and Identified Instruments
Twelve different instruments were identified (see Table 3 for an overview and Table 4 for quality assessment). The Parent-Adolescent Communication Scale (PACS; Barnes & Olson, 1982) was used in 100 papers based on 85 studies. The Parent–Child Communication Scale (PCCS; McCarty, McMahon and Conduct Problems Prevention Research Group, 2003) was used in seven papers based on four studies. The Parent-Adolescent Communication Inventory (PACI; Bienvenu, 1969) and the Revised Family Communication Patterns Instrument (RFCP; Ritchie & Fitzpatrick, 1990) were used in three studies each. The Parent–Child Communication Questionnaire (PCCQ; Yang & Zou, 2008), the Parent–Child Communication Scale (PCCS; Loeber et al., 1998; also known under the name Revised Parent-Adolescent Communication Form (RPACF); Loeber et al., 1991), and the Parent–Child Communication Scale (PCCS; Krohn et al., 1992) were all used in two studies each. The Father-Adolescent/Mother-Adolescent Communication Scale (FACS/MACS; Shek et al., 2006), the Parent–Child Communication Scale (PCCS; Chi, 2011), the Perception of Parenting Communication Scale (COMPA; Portugal & Alberto, 2014), the Parent-Adolescent Communication Inventory (PACI; Schmidt et al., 2010), and the Family Communication Patterns Scale (FCP; McLeod et al., 1972) were all used in one study each.
The Parent–Adolescent Communication Scale (PACS)
The PACS (Barnes & Olson, 1982) was the most widely used instrument and has been translated from English into nine other languages (Spanish, Dutch, Chinese, French, Malay, Italian, Khmer, Korean, and Swedish). The instrument comprises two subscales (open communication and communication problems, 10 items each). Items are measured on a 5-point Likert scale, and parent and children versions are identical apart from changing referents (my mother/father/daughter/son). For the quality assessment, Barnes and Olson's (1982) study was considered as source in addition to the studies retrieved by the systematic literature search. In terms of content validity, the original authors specified the conceptual foundation within the framework of the circumplex model of family functioning: parent–child communication was conceptualized as an additional dimension facilitating adaptive change in family functioning (Barnes & Olson, 1985). However, in most studies found in this review, the PACS was used as a stand-alone measure of dyadic parent–child communication. The factorial structure found in the initial study (Barnes & Olson, 1982) was corroborated by a principal component analysis in a Dutch study (Jackson et al., 1998). In a Spanish sample, however, three factors were found in another principle component analysis (open communication, communication problems, and avoidant communication; Estevez et al., 2005). In an American sample, only one factor was found in exploratory and confirmatory factor analyses, with two items from the problem scale not loading on the same factor as the other items (Wu & Chao, 2011). The PACS has shown good internal consistency in most of its’ versions. The means and standard deviations are available for large samples (i.e., n > 400) in six versions (see Table 2). For the English version of the PACS, some evidence on test–retest reliability and treatment sensitivity was found. The included studies did not report sufficiently on construct and discriminative validity. The PACS has been published originally in Barnes and Olson (1982) and is available online (for example: https://scales.arabpsychology.com/s/parent-adolescent-communication-scale-pacs/).
The Parent–Child Communication Scale (PCCS McCarty)
The PCCS (McCarty, McMahon and Conduct Problems Prevention Research Group, 2003) was the second most widely used instrument. It has been translated from English into Norwegian and Khmer. Parent and child versions are different; the child version consists of 10 items (parents 20 items) in the original version and is based on a 5-point Likert scale. For quality assessment, Pek (2006) was considered as additional source. With regard to content validity, the instrument is intended to assess the parent’s openness to communication (Pek, 2006), but the conceptual foundation is not specified further. In later analyses, only eight items fit the subscales parent and child communication (five and three items, respectively). This factorial structure was corroborated by confirmatory factor analyses in a Norwegian study (Orm et al., 2022). Internal consistency is between low and adequate. For the English version, norm values of a large sample exist (Pek, 2006), means and standard deviations for an at-risk sample can be found in Orm et al. (2021, 2022). There was no sufficient evidence with regard to test–retest reliability, construct, and discriminative validity, but for treatment sensitivity. The PCCS is available from the website of the Fast Track Project (https://fasttrackproject.org/data-instruments). The questionnaire is not included in the original reference publication (McCarty et al., 2003).
The Parent–Adolescent Communication Inventory (PACI Bienvenu)
The PACI (Bienvenu, 1969) is explicitly recommended for children older than 13 years. According to Carson et al. (1999) and Green and Vosler (1992), it consists of 40 items, whereas the original author claims it to be a 36-item scale. No subscales are hypothesized nor has a factorial structure been reported. The original article (Bienvenu, 1969) was considered as an additional source for quality assessment. Psychometric data on test–retest reliability have been presented (Bienvenu, 1969). Green and Vosler (1992) reported treatment sensitivity with regard to the parent, but not the child scale. Internal consistency is less than adequate. In the present sample of studies, there was no information on content, discriminative, and construct validity for the PACI. A 21-item version of the scale is available in the original publication (Bienvenu, 1969).
The Revised Family Communication Patterns Instrument (RFCP)
The RFCP (Ritchie & Fitzpatrick, 1990) consists of 26 items and has two subscales: conformity and conversation orientation (11 and 15 items). For the quality assessment, Ritchie and Fitzpatrick's (1990) study was considered as an additional source. The factorial structure has not been explored and there is no information on treatment sensitivity. Internal consistency is good, and test–retest reliability is adequate. In the present sample of studies, there was no information on content, discriminative, and construct validity for the RFCP. The RFCP is available online (http://dx.doi.org/10.13140/RG.2.2.15136.64000) and also included in the original publication (Ritchie & Fitzpatrick, 1990).
Further Instruments
With regard to the remaining instruments, the PCCS (Chi, 2011) and the PCCQ consist of two and four subscales, respectively. The COMPA is recommended for ages seven to 18 and has five subscales: Parental availability to communication, children confidence/sharing, emotional support/affective expression, meta-communication, and negative communication patterns (Portugal & Alberto, 2014). The factor structures have not been established for the PCCS (Chi), the PCCQ, or the COMPA. The means and standard deviations in larger samples (i.e., n > 400) were only reported for the FACS/MACS (Shek et al., 2006) and for the PCCS (Chi, 2011). The internal consistencies ranged from less than adequate (COMPA; Portugal & Alberto, 2014) over adequate (FCP; McLeod et al., 1972; PCCQ; & Zou, 2008; PCCS; Krohn et al., 1992; PCCS; Loeber et al., 1998) and good (PACI; Schmidt et al., 2010; PCCS; Chi, 2011) to excellent (FACS/MACS; Shek et al., 2006). Test–retest reliability, content validity, construct validity, factorial structure, discriminative validity, and treatment sensitivity were not reported in any of the included studies. To our knowledge, complete original items are only available for COMPA and PCCS (Krohn) in Portugal and Alberto (2014) and Krohn et al. (1992), respectively.
Synthesis: Psychometric Evidence of Parent–Child Communication Measures
We extracted the available psychometric data from all publications. We included additional sources on psychometric data in our assessment of the psychometric quality for four measures (i.e., PACS, PCCS (McCarty), PACI, (Bienvenu), RFCP; i.e., Barnes & Olson, 1982, 1985; Bienvenu, 1969; Ritchie & Fitzpatrick, 1990; Pek, 2006). Most instruments showed at least adequate internal consistency. Means and standard deviations that can be considered as normative information (community samples N > 400 and clinical samples N > 100) were reported for almost half of the existing measures (Table 4). The conceptual and theoretical background of the instruments were often not specified clearly. Additional psychometric information is scarce, and construct and discriminative validity were not stated in an explicit way for any of the instruments. However, means (Table 2) indicate that PACS and PCCS (McCarty) can detect differences in the quality of parent–child communication between community, at-risk, and clinical samples.
Discussion
The aim of this review was to identify instruments that measure parent-child communication from the child’s perspective as well as which samples they have been applied to and to assess the psychometric quality of these instruments. We identified twelve instruments across 106 studies. The PACS had been used in most studies (k = 85) by far. This means there are relatively few multiple-item and general (i.e., not topic-specific) child-rated parent–child communication instruments, given that we included > 100 studies in this review. On the one hand, this indicates some unification in the field, with a strong PACS dominance. Given that the other instruments were used in four studies each or less, with five instruments having only been used in single studies, a potential conclusion could be that the PACS should be considered the “gold standard” for child-reported parent–child communication quality. However, frequency does not ensure quality, which will be elaborated on below.
Before addressing samples and psychometric quality, however, it is important to consider that the existing instruments measure quite different aspects of parent–child communication, ranging from communication problems, openness or conformity and conversation orientation over problem-solving oriented, or avoidant communication to meta-communication. This variety reflects the complexity of communication and points to the fact that doing research on communication also should entail conceptual consideration. In addition to using measures with adequate psychometric properties, researchers and/or clinicians should be aware that they can aim at measuring quite different aspects of parent–child communication.
In terms of theoretical foundation, the information on most instruments was scarce. Considering that multiple studies were excluded due to using single-item measures (e.g., how would you rate the communication between you and your father/mother) or topic-specific measures (e.g., about alcohol, drugs, sex), there seems to be relatively little theory-based consensus in the field concerning how to conceptualize “parent–child communication” in a child-rated instrument. The two most dominating dimensions concern how open and/or problematic the communication is considered. However, the range of existing subscales indicates that there may be additional relevant dimensions of parent–child communication. In addition, the theoretical background of openness and communication problems also needs further clarification, since, for example, openness can be considered as a matter of openness for different perspectives or as openness for expressing emotions. Hence, a synthesis of previous models of parent–child communication, as has been attempted for the variable family communication (Murphy et al., 2017), would be desirable. Up to now, the field lacks standards for measuring other dimensions of parent–child communication.
The samples used ranged from general community samples via at-risk samples to clinical samples, with a dominance for community samples. More than half the studies were conducted in the North Americas (USA and Canada), with an even number of European and Asian studies in “second place,” followed by only a handful of studies from Middle and South America or Australia, and only one study from Africa. Although the USA samples included a mix of White, Black, Asian, and Hispanic Americans, there is clearly a need to examine and validate parent–child communication measures cross-culturally. Only the PACS has been used in clinical, at-risk, and community samples. The COMPA, PACI, RFCP, PCCS (Loeber), and PCCS (McCarty) instruments have been used in at-risk and community samples. The PACS and PCCS (McCarty) instruments can detect the differences in the quality of parent–child communication between these samples.
In terms of psychometric quality, the evidence backing most of the scales was insufficient. Our evaluation of this was based both on original publications of the instruments, as well as the synthesized data across studies that have used the instruments. Generally, little is known about most instruments, and even the English version of the PACS reached only 11 of 27 possible points in our quality assessment based on information from 51 publications. Adequate evidence for psychometric core aspects such as test–retest reliability or factorial structure was found for less than a handful of instruments. Across the studies, construct and discriminative validity have hardly been evaluated in the included studies. In addition, little information was available regarding convergent validity with regard to other measures such as observer-based (Hadley et al., 2013) or parent-based reports (Hartos & Power, 2000a, 2000b). However, it is important to note that while our main overall goal was to assess the psychometric properties of parent–child communication measures, this was not the goal of the reviewed studies. Rather, most of the included studies considered various research questions, of which parent–child communication was one of the several. At best, the results of some of the individual studies can be interpreted as preliminary/emerging evidence for construct and discriminative validity for one measure in one sample. However, when considered combined in this review, overall systematic evidence for the psychometric properties of even widely used scales (e.g., the PACS) must be said to be severely lacking.
We also aimed to consider availability of the instruments. Various abbreviations for the different instruments were often used inconsistently in the literature. Further confusion is added since some of the instruments are based on each other: The PACS has been used as one of several sources for the PCCS (Loeber), which, in turn, was used for the PCCS (McCarty) and the PCCS (Krohn). It is also noteworthy that the original PCCS (McCarty) instrument (child version) contains six items from the PACS almost literally, only the grammar has been changed from first to second person. The parent communication subscale of the PCCS (McCarty) consists of five items, with four from the PACS (three from the open, one from the problem subscale). The child communication subscale comprises three items with only one from the PACS. However, the two remaining items are fairly close to other PACS items. This leads to confusion about the measures and underlines the importance of indicating correct sources, number of items, scale range, and example items. In terms of availability, the instruments had been translated and used in a total of twelve languages.
Limitations
To our knowledge, this review is the first to give a comprehensive and systematic summary of parent–child communication measures and their psychometric properties. However, there are some limitations. The review did not include observational or parent report measures. The selection criteria limited the search down to published peer-review articles but did not consider other publications, unless they were cited as a source for psychometric information in the included papers. In that case, they were considered in the quality assessment. If publications such as dissertations would have been included, other information regarding conceptual considerations and psychometric evidence might have been found. In terms of age, our search was limited to ages 8–21 years. Hence, the psychometric evidence for single instruments may differ with regard to emerging adults. Even though we searched for instruments in any language, we only considered publications in English, leading to a certain bias between English and non-English instruments. For that reason, the quality assessment does not allow for an exact comparison between instruments of different languages. Last but not least, since genuine psychometric studies were hardly found, we decided to not use the EMPRO tool (Valderas et al., 2008) to conduct the quality assessment as initially planned. Instead, we decided to gather psychometric information with an adapted tool that was more apt to also consider information found in a huge number of non-psychometric study reports.
Implications and Conclusions
This review has implications for practice and research. For researchers and practitioners interested in examining parent–child communication from the child’s perspective, there are several child-rated instruments to choose from in English, Chinese, and some European languages. We have provided availability information for the four most-used child-rated parent–child communication scales in the methods section. The most widely used scale is the PACS (Barnes & Olson, 1982), which considers the degree of openness and problems in communication, and with some evidence of factor structure and other psychometric properties. However, the PACS should not necessarily be the default choice due to frequency alone. Upon choosing which instrument to apply, practitioners and researchers should take active and informed choices about which aspect of parent–child communication they aim to assess, as the instruments focus on different dimensions of parent–child communication. For example, whereas the PACS concerns openness and communication problems, the RFCP measures conformity and conversation orientation.
In terms of research implications, there is a need for more studies assessing the psychometric properties of parent–child communication scales, and when choosing an instrument, also conceptual and cross-cultural aspects should be carefully considered. To avoid confusion, instruments should be reported with correct sources, number of items, scale range, and example items. Future research should also consider triangulating child and parent reports as well as observational measures.
Data Availability
No new data were created during the study.
References
*References included in review
Achenbach, T. M., McConaughy, S. H., & Howell, C. T. (1987). Child/adolescent behavioral and emotional problems: Implications of cross-informant correlations for situational specificity. Psychological Bulletin, 101(2), 213–232. https://doi.org/10.1037/0033-2909.101.2.213
Acock, A., & Bengtson, V. (1980). Socialization and attribution processes: Actual versus perceived similarity among parents and youth. Journal of Marriage and Family, 42, 501–515. https://doi.org/10.2307/351895
*Acuña, M. A., & Kataoka, S. (2017). Family communication styles and resilience among adolescents. Social Work, 62(3), 261–269.https://doi.org/10.1093/sw/swx017.
Arnett, J. J. (1999). Adolescent storm and stress, reconsidered. American Psychologist, 54, 317–326. https://doi.org/10.1037/0003-066X.54.5.317
*Asfour, L., Huang, S., Ocasio, M. A., Perrino, T., Schwartz, S. J., Feaster, D. J. et al. (2017). Association between socio-ecological risk factor clustering and mental, emotional, and behavioral problems in Hispanic adolescents. Journal of Child and Family Studies, 26(5), 1266–1273.https://doi.org/10.1007/s10826-016-0641-0.
*Bandura, A., Caprara, G. V., Barbaranelli, C., Regalia, C., & Scabini, E. (2011). Impact of family efficacy beliefs on quality of family functioning and satisfaction with family life. Applied Psychology, 60(3), 421–448.https://doi.org/10.1111/j.1464-0597.2010.00442.x.
Barnes, H., & Olson, D. H. (1982). Parent-adolescent communication scale. In D. H. Olson, H. McCubbin, H. Barnes, A. Larsen, M. Muxen, & W. Wilson (Eds.), Family inventories: Inventories used in a national survey of families across the family life cycle (pp. 33–48). Family Social Science, University of Minnesota.
Barnes, H. L., & Olson, D. H. (1985). Parent–adolescent communication and the circumplex model. Child Development, 56(2), 438–447. https://doi.org/10.2307/1129732
*Bartlett, R., Johnson, A., Randolph, I., & McCoy, T. P. (2016). Communication and bonding between African-American middle school girls and their maternal figures. Journal of National Black Nurses’ Association, 27(1), 18–23.
*Berzonsky, M. D., Branje, S. J. T., & Meeus, W. (2007). Identity-processing style, psychosocial resources, and adolescents’ perceptions of parent-adolescent relations. The Journal of Early Adolescence, 27(3), 324–345.https://doi.org/10.1177/0272431607302006.
Bienvenu, M. J. (1969). Measurement of parent-adolescent communication. Family Coordinator, 18(2), 117–121. https://doi.org/10.2307/582224
*Bireda, A. D., & Pillay, J. (2018). Perceived parent–child communication and well-being among Ethiopian adolescents. International Journal of Adolescence and Youth, 23(1), 109–117.https://doi.org/10.1080/02673843.2017.1299016.
*Blanc, A., Navas, M., Calderón, S., & Sánchez-Castelló, M. (2022). The importance of family in acculturation process of adolescents of Moroccan origin in Spain. International Journal of Psychology, 57(2), 240–250.https://doi.org/10.1002/ijop.12804.
*Brage, D., Meredith, W. M., & Woodward, J. (1993). Correlates of loneliness among Midwestern adolescents. Adolescence, 28(111), 685–694.
*Branje, S. J. T. (2008). Conflict management in mother-daughter interactions in early adolescence. Behaviour, 145, 1627–1651.https://doi.org/10.1163/156853908786131315.
*Cai, J., Wang, Y., Wang, F., Lu, J., Li, L., & Zhou, X. (2021). The association of parent-child communication with internet addiction in left-behind children in China: A cross-sectional study. International Journal of Public Health, 66, 630700. https://doi.org/10.3389/ijph.2021.630700.
*Caprara, G. V., Pastorelli, C., Regalia, C., Scabini, E., & Bandura, A. (2005). Impact of adolescents' filial self‐efficacy on quality of family functioning and satisfaction. Journal of Research on Adolescence, 15(1), 71–97.https://doi.org/10.1111/j.1532-7795.2005.00087.x.
*Carbonero, M. A., Martín-Antón, L. J., Otero, L., & Monsalvo, E. (2017). Program to promote personal and social responsibility in the secondary classroom. Frontiers in Psychology, 8, 809.https://doi.org/10.3389/fpsyg.2017.00809.
*Carson, D. K., Chowdhury, A., Perry, C. K., & Pati, C. (1999). Family characteristics and adolescent competence in India: Investigation of youth in southern Orissa. Journal of Youth and Adolescence, 28(2), 211-233.https://doi.org/10.1023/A:1021653415366.
*Chen, X., Xie, Q., & Yang, Y. (2019). Adolescent smoking behavior and communication with parents: Depression as a mediator and gender as a moderator. Social Behavior and Personality: An International Journal, 47(10), 1–9.https://doi.org/10.2224/sbp.8262.
Chi, L.-P. (2011). A three-level model of parent-child communication: Theory, scale and application in Chinese 5th and 6th graders [Chinese]. Psychological Development and Education, 2, 140–150.
*Cho, I. Y., Kim, J. S., & Kim, J. O. (2018). Factors influencing adolescents’ self-control according to family structure. Journal of Child and Family Studies, 27, 3520–3530.https://doi.org/10.1007/s10826-018-1175-4.
*Clark, R. D., & Shields, G. (1997). Family communication and delinquency. Adolescence, 32(125), 81–93.
*Collins, W. E., Newman, B. M., & McKenry, P. C. (1995). Intrapsychic and interpersonal factors related to adolescent psychological well-being in stepmother and stepfather families. Journal of Family Psychology, 9(4), 433–445.https://doi.org/10.1037/0893-3200.9.4.433.
*Cordova, D., Huang, S., Lally, M., & Estrada, Y., Prado, G. (2014). Do parent–adolescent discrepancies in family functioning increase the risk of Hispanic adolescent HIV risk behaviors. Family Process, 53(2), 348–363. https://doi.org/10.1111/famp.12067.
*Cornell, D. G., Callahan, C. M., & Loyd, B. H. (1991). Socioemotional adjustment of adolescent girls enrolled in a residential acceleration program. Gifted Child Quarterly, 35(2), 58–66.https://doi.org/10.1177/001698629103500202.
*Daley, T. C. (2006). Perceptions and congruence of symptoms and communication among second-generation Cambodian youth and parents: A matched-control design. Child Psychiatry and Human Development, 37(1), 39–53.https://doi.org/10.1007/s10578-006-0018-5.
*Davidson, T. M., & Cardemil, E. V. (2009). Parent–child communication and parental involvement in Latino adolescents. Journal of Early Adolescence, 29(1), 99–121.https://doi.org/10.1177/0272431608324480.
*de la Moral Rubia, J., & Ortiz Morales, H. (2012). Risk and protective factors of dissocial behavior in a probability sample. The Spanish Journal of Psychology, 15(2), 736–747.https://doi.org/10.5209/rev_SJOP.2012.v15.n2.38885.
De Los Reyes, A., & Kazdin, A. E. (2005). Informant discrepancies in the assessment of childhood psychopathology: A critical review, theoretical framework, and recommendations for further study. Psychological Bulletin, 131(4), 483–509. https://doi.org/10.1037/0033-2909.131.4.483
De Los Reyes, A., & Langer, D. A. (2018). Assessment and the Journal of Clinical Child and Adolescent Psychology’s evidence base updates series: Evaluating the tools for gathering evidence. Journal of Clinical Child & Adolescent Psychology, 47(3), 357–365. https://doi.org/10.1080/15374416.2018.1458314
*De Los Reyes, A., Ohannessian, C. M., & Laird, R. D. (2016). Developmental changes in discrepancies between adolescents’ and their mothers’ views of family communication. Journal of Child and Family Studies, 25(3), 790–797.https://doi.org/10.1007/s10826-015-0275-7.
*Dickerson, A. D., & Crase, S. J. (2005). Parent-adolescent relationships: The influence of multi-family therapy group on communication and closeness. The American Journal of Family Therapy, 33(1), 45–59.https://doi.org/10.1080/01926180590889194.
Dixson, M. D. (1995). Models and perspectives of parent-child communication. In T. Socha & G. Stamp (Eds.), Parents, children, and communication: Frontiers of theory and research (pp. 43–62). Erlbaum.
*Estévez, E., Musitu, G., & Herrero, J. (2005). The influence of violent behavior and victimization at school on psychological distress: The role of parents and teachers. Family Therapy, 32(3), 143.
Estlein, R. (2021). Parenting as a communication process: Integrating interpersonal communication theory and parenting styles conceptualization. Journal of Family Theory & Review, 13(1), 21–33. https://doi.org/10.1111/jftr.12407
Facca, D., Gladstone, B., & Teachman, G. (2020). Working the limits of “giving voice” to children: A critical conceptual review. International Journal of Qualitative Methods, 19, 1609406920933391. https://doi.org/10.1177/1609406920933391
*Farrell, M. P., & Barnes, G. M. (1993). Family systems and social support: A test of the effects of cohesion and adaptability on the functioning of parents and adolescents. Journal of Marriage and the Family, 55(1) 119-132.https://doi.org/10.2307/352963.
Feddern Donbaek, D., & Elklit, A. (2014). A validation of the Experiences in Close Relationships-Relationship Structures scale (ECR-RS) in adolescents. Attachment & Human Development, 16(1), 58–76. https://doi.org/10.1080/14616734.2013.850103
*Finan, L. J., Ohannessian, C. M., & Gordon, M. S. (2018). Trajectories of depressive symptoms from adolescence to emerging adulthood: The influence of parents, peers, and siblings. Developmental Psychology, 54(8), 1555.https://doi.org/10.1037/dev0000543.
*Fite, P. J., Rubens, S. L., Preddy, T. M., Raine, A., & Pardini, D. A. (2014). Reactive/proactive aggression and the development of internalizing problems in males: The moderating effect of parent and peer relationships. Aggressive Behavior, 40(1), 69–78.https://doi.org/10.1002/ab.21498.
*Fitzpatrick, M. A., & Ritchie, L. D. (1994). Communication schemata within the family. Human Communication Research, 20(3), 275–301.https://doi.org/10.1111/j.1468-2958.1994.tb00324.x.
Fitzpatrick, M. A., & Koerner, A. F. (2005). Family communication schemata: effects on children’s resiliency. In S. Dunwoody, L. B. Becker, D. McLeod, & G. Kosicki (Eds.), The evolution of key mass communication concepts: Honoring Jack M. McLeod (pp. 115–139). Hampton.
*Fjermestad, K., Pat, P., Dearozet, S., Vatne, T., Hafting, M., & Jegannathan, B. (2020). Manual-based group intervention for siblings and parents of children with neurodevelopmental disorders in Cambodia. Journal of Developmental and Physical Disabilities.https://doi.org/10.1007/s10882-020-09777-3.
*Fredriksen, T., Marie Vatne, T., Bjartveit Haukeland, Y., Tudor, M., & Fjermestad, K. W. (2021). Siblings of children with chronic disorders: Family and relational factors as predictors of mental health. Journal of Child Health Care.https://doi.org/10.1177/13674935211052157.
*Gosselin, J., & David, H. (2007). Risk and resilience factors linked with the psychosocial adjustment of adolescents, stepparents and biological parents. Journal of Divorce & Remarriage, 48(1–2), 29–53.https://doi.org/10.1300/J087v48n01_02.
*Green, R. G., & Vosler, N. R. (1992). Issues in the assessment of family practice: An empirical study. Journal of Social Service Research, 15(3–4), 1–19.https://doi.org/10.1300/J079v15n03_01.
Grotevant, H. D. (2001). Developing new insights from a process approach to adolescent development. Human Development, 44, 55–58. https://doi.org/10.1159/000057041
Guilamo-Ramos, V., Jaccard, J., Dittus, P., & Bouris, A. M. (2006). Parental expertise, trustworthiness, and accessibility: Parent-adolescent communication and adolescent risk behavior. Journal of Marriage and Family, 68, 1229–1246. https://doi.org/10.1111/j.1741-3737.2006.00325.x
*Hadley, W., Stewart, A., Hunter, H. L., Affleck, K., Donenberg, G., DiClemente, R. et al. (2013). Reliability and validity of the dyadic observed communication scale (DOCS). Journal of Child and Family Studies, 22(2), 279–287.https://doi.org/10.1007/s10826-012-9577-1.
*Hartos, J. L., & Power, T. G. (1997). Mothers’ awareness of their early adolescents’ stressors: Relation between awareness and adolescent adjustment. The Journal of Early Adolescence 17(4), 371–389https://doi.org/10.1177/0272431697017004002.
*Hartos, J. L., & Power, T. G. (2000a). Association between mother and adolescent reports for assessing relations between parent–adolescent communication and adolescent adjustment. Journal of Youth and Adolescence, 29(4), 441–450.https://doi.org/10.1023/A:1005158425861.
*Hartos, J. L., & Power, T. G. (2000b). Relations among single mothers’ awareness of their adolescents’ stressors, maternal monitoring, mother-adolescent communication, and adolescent adjustment. Journal of Adolescent Research, 15(5), 546–563.https://doi.org/10.1177/0743558400155002.
*Haukeland, Y. B., Czajkowski, N. O., Fjermestad, K. W., Silverman, W. K., Mossige, S., & Vatne, T. M. (2020). Evaluation of “SIBS”, an Intervention for siblings and parents of children with chronic disorders. Journal of Child and Family Studies, 29(8), 2201–2217.https://doi.org/10.1007/s10826-020-01737-x.
*Haukeland, Y. B., Vatne, T. M., Mossige, S., & Fjermestad, K. (2021). Psychosocial functioning in siblings of children with rare disorders compared to controls. The Yale Journal of Biology and Medicine, 94, 537–544.
*Heller, S. R., Robinson, L. C., Henry, C. S., & Plunkett, S. W. (2006). Gender differences in adolescent perceptions of parent-adolescent openness in communication and adolescent empathy. Marriage & Family Review, 40(4), 103-122.https://doi.org/10.1300/J002v40n04_06.
*Henry, C. S., & Lovelace, S. G. (1995). Family resources and adolescent family life satisfaction in remarried family households. Journal of Family Issues, 16(6), 765–786.https://doi.org/10.1177/019251395016006005.
*Herrero, J., Estévez, E., & Musitu, G. (2006). The relationships of adolescent school-related deviant behaviour and victimization with psychological distress: Testing a general model of the mediational role of parents and teachers across groups of gender and age. Journal of Adolescence, 29(5), 671–690.https://doi.org/10.1016/j.adolescence.2005.08.015.
*Hill, K. A., & Roberts, D. D. (2019). Parent–adolescent communication and social impacts on Black American adolescents’ academic well-being. Journal of Child and Family Studies, 28(11), 3207–3219.https://doi.org/10.1007/s10826-019-01497-3.
*Houck, C. D., Rodrigue, J. R., & Lobato, D. (2007). Parent–adolescent communication and psychological symptoms among adolescents with chronically ill parents. Journal of Pediatric Psychology, 32(5), 596–604.https://doi.org/10.1093/jpepsy/jsl048.
*Howard, D. E., Cross, S. I., Li, X., & Huang, W. (1999). Parent–youth concordance regarding violence exposure: Relationship to youth psychosocial functioning. Journal of Adolescent Health, 25(6), 396–406.https://doi.org/10.1016/s1054-139x(99)00102-0.
*Howard Sharp, K. M., Meadows, E. A., Keim, M. C., Winning, A. M., Barrera, M., Gilmer, M. J. et al. (2020). The influence of parent distress and parenting on bereaved siblings’ externalizing problems. Journal of Child and Family Studies, 29(4), 1081–1093.https://doi.org/10.1007/s10826-019-01640-0.
*Huizinga, G. A., Visser, A., van der Graaf, W. T., Hoekstra, H. J., & Hoekstra-Weebers, J. E. (2005). The quality of communication between parents and adolescent children in the case of parental cancer. Annals of Oncology, 16(12), 1956–1961. https://doi.org/10.1093/annonc/mdi395.
Hunsley, J., & Mash, E. J. (2007). Evidence-based assessment. Annual Review of Clinical Psychology, 3, 29–51. https://doi.org/10.1146/annurev.clinpsy.3.022806.091419
Hunsley, J., & Mash, E. J. (Eds.). (2008). A guide to assessments that work. Oxford University Press.
Hunsley, J., & Mash, E. J. (Eds.). (2018). A guide to assessments that work (2nd ed.). Oxford University Press.
*Ioffe, M., Pittman, L. D., Kochanova, K., & Pabis, J. M. (2020). Parent-adolescent communication influences on anxious and depressive symptoms in early adolescence. Journal of Youth and Adolescence, 49(8), 1716–1730.https://doi.org/10.1007/s10964-020-01259-1.
*Jackson, S., Bijstra, J., Oostra, L., & Bosma, H. (1998). Adolescents’ perceptions of communication with parents relative to specific aspects of relationships with parents and personal development. Journal of Adolescence, 21(3), 305–322.https://doi.org/10.1006/jado.1998.0155.
*Jeong, Y.-J., & Chun, Y.-J. (2010). The pathways from parents’ marital quality to adolescents’ school adjustment in South Korea. Journal of Family Issues, 31(12), 1604–1621.
*Jiménez, T. I., Estévez, E., Velilla, C. M., Martin-Albo, J., & Martínez, M. L. (2019). Family communication and verbal child-to-parent violence among adolescents: the mediating role of perceived stress. International Journal of Environmental Research and Mental Health, 16(22), 4538.https://doi.org/10.3390/ijerph16224538.
Kapetanovic, S., & Boson, K. (2022). Discrepancies in parents’ and adolescents’ reports on parent-adolescent communication and associations to adolescents’ psychological health. Current Psychology, 41, 4259–4270. https://doi.org/10.1007/s12144-020-00911-0
*Keim, M. C., Lehmann, V., Shultz, E. L., Winning, A. M., Rausch, J. R., Barrera, M. et al. (2017). Parent-child communication and adjustment among children with advanced and non-advanced cancer in the first year following diagnosis or relapse. Journal of Pediatric Psychology, 42(8), 871–881.https://doi.org/10.1093/jpepsy/jsx058.
Kelly, L., Keaten, J., Finch, C., Duarte, I. B., Hoffman, P., & Michels, M. M. (2002). Family communication patterns and the development of reticence. Communication Education, 51, 202–209. https://doi.org/10.1080/03634520216506
*Kim, E., Yim, H. W., Jeong, H., Jo, S. J., Lee, H. K., Son, H.J. & Han, H.H. (2018). The association between aggression and risk of Internet gaming disorder in Korean adolescents: The mediation effect of father-adolescent communication style. Epidemiology and Health, 40, e2018039. https://doi.org/10.4178/epih.e2018039.
*Kim, M., & Park, I. J. K. (2011). Testing the moderating effect of parent–adolescent communication on the acculturation gap–distress relation in Korean American families. Journal of youth and adolescence, 40(12), 1661–1673.https://doi.org/10.1007/s10964-011-9648-4.
*Kimiecik, J. C., & Horn, T. S. (2012). Examining the relationship between family context and children’s physical activity beliefs: The role of parenting style. Psychology of Sport and Exercise, 13(1), 10–18.https://doi.org/10.1016/j.psychsport.2011.08.004.
*Knight, G. P., Tein, J. Y., Shell, R., & Roosa, M. (1992). The cross‐ethnic equivalence of parenting and family interaction measures among Hispanic and Anglo‐American families. Child Development, 63(6), 1392–1403.https://doi.org/10.2307/1131564.
Koerner, A. F., & Fitzpatrick, M. A. (1997). Family type and conflict: The impact of conversation orientation and conformity orientation on conflict in the family. Communication Studies, 48, 59–75. https://doi.org/10.1080/10510979709368491
Koerner, A. F., & Fitzpatrick, M. A. (2002). Toward a theory of family communication. Communication Theory, 12, 70–91. https://doi.org/10.1111/j.1468-2885.2002.tb00260.x
Krauss, R. M., & Fussell, S. R. (1996). Social psychological models of interpersonal communication. In E. T. Higgins & A. Kruglanski (Eds.), Social psychology: Handbook of basic principles (pp. 655–701). Guilford Press.
Krohn, M. D., Stern, S. B., Thornberry, T. P., & Jang, S. J. (1992). The measurement of family process variables: The effect of adolescent and parent perceptions of family life on delinquent behavior. Journal of Quantitative Criminology, 8(3), 287–315. https://doi.org/10.1007/BF01064550
*Kwok, S. Y. C. L., & Shek, D. T. L. (2010a). Hopelessness, parent-adolescent communication, and suicidal ideation among Chinese adolescents in Hong Kong. Suicide and Life-Threatening Behavior, 40(3), 224–233. https://doi.org/10.1521/suli.2010.40.3.224
*Kwok, S. Y. C. L., & Shek, D. T. L. (2010b). Personal and family correlates of suicidal ideation among Chinese adolescents in Hong Kong. Social Indicators Research, 95, 407–419.https://doi.org/10.1007/s11205-009-9528-4.
*Kwok, S. Y. C. L., & Shek, D. T. L. (2011). Family processes and suicidal ideation among Chinese adolescents in Hong Kong. The Scientific World Journal, 11, 27–41.https://doi.org/10.1100/tsw.2011.2.
Lambert, S. F., & Cashwell, C. S. (2004). Preteens talking to parents: Perceived communication and school-based aggression. The Family Journal, 12(2), 122–128. https://doi.org/10.1177/1066480703261953
Larsson, I., Staland-Nyman, C., Svedberg, P., Nygren, J. M., & Carlsson, I.-M. (2018). Children and young people’s participation in developing interventions in health and well-being: A scoping review. BMC Health Services Research, 18(1), 507. https://doi.org/10.1186/s12913-018-3219-2
*Lin, L., Wang, S., & Li, J. (2021). Association between the search for meaning in life and well-being in Chinese adolescents. Applied Research in Quality of Life.https://doi.org/10.1007/s11482-021.
Lindelöw, M. (1999). Parent–child interaction and adult depression: A prospective study. Acta Psychiatrica Scandinavica, 100, 270–278. https://doi.org/10.1111/j.1600-0447.1999.tb10861.x
Liu, Y. L. (2003). Parent-child interaction and children’s depression: The relationships between parent-child interaction and children’s depressive symptoms in Taiwan. Journal of Adolescence, 26, 447–457. https://doi.org/10.1016/s0140-1971(03)00029-0
*Liu, Q., Lin, Y., Zhou, Z., & Zhang, W. (2019). Perceived parent–adolescent communication and pathological Internet use among Chinese adolescents: A moderated mediation model. Journal of Child and Family Studies, 28(6), 1571–1580.https://doi.org/10.1371/journal.pone.0075642.
Loeber, R., Farrington, D. P., Stouthamer-Loeber, M., & Van Kammen, W. B. (1998). Antisocial behavior and mental health problems: Explanatory factors in childhood and adolescence. Psychology Press.
Loeber, R., Stouthamer-Loeber, M., Van Kammen, W., & Farrington, D. P. (1991). Initiation, escalation and desistance in juvenile offending and their correlates. Journal of Criminal Law & Criminology, 82, 36–82.
*López, E. E., Olaizola, J. H., Ferrer, B. M. & Ochoa, G.M. (2006). Aggressive and nonaggressive rejected students: An analysis of their differences. Psychology in the Schools, 43(3), 387–400.https://doi.org/10.1002/pits.20152.
*Lu, J., Lin, L., Roy, B., Riley, C., Wang, E., Wang, K. et al. (2020). The impacts of parent-child communication on left-behind children’s mental health and suicidal ideation: A cross sectional study in Anhui. Children and Youth Services Review, 110, 104785. https://doi.org/10.1016/j.childyouth.2020.104785.
*Malcolm, S., Huang, S., Cordova, D., Freitas, D., Arzon, M., Jimenez, G. L., Pantin, H. & Prado, G. (2013). Predicting condom use attitudes, norms, and control beliefs in Hispanic problem behavior youth: The effects of family functioning and parent–adolescent communication about sex on condom use. Health Education & Behvior, 40(4), 384–391.https://doi.org/10.1177/1090198112440010.
*Manczak, E. M., Donenberg, G. R., & Emerson, E. (2018). Can mother–daughter communication buffer adolescent risk for mental health problems associated with maternal depressive symptoms. Journal of Clinical Child & Adolescent Psychology, 47(1), S509–S519.https://doi.org/10.1080/15374416.2018.1443458.
*Marta, E. (1997). Parent-adolescent interactions and psychosocial risk in adolescents: An analysis of communication, support and gender. Journal of Adolescence, 20(5), 473–487. https://doi.org/10.1006/jado.1997.0103.
McCarty, C. A., McMahon, R. J., Conduct Problems Prevention Research Group. (2003). Mediators of the relation between maternal depressive symptoms and child internalizing and disruptive behavior disorders. Journal of Family Psychology: Journal of the Division of Family Psychology of the American Psychological Association Division, 17(4), 545–556. https://doi.org/10.1037/0893-3200.17.4.545
McLean, K. C., Pasupathi, M., & Pals, J. L. (2007). Selves creating stories creating selves: A process model of self-development. Personality and Social Psychology Review, 11, 262–278. https://doi.org/10.1177/1088868307301034
McLeod, J. M., Atkin, C. K., & Chaffee, S. H. (1972). Adolescents, parents and television use: self report and other-report measures from the Wiscon sample. In G. A. Comstock & E. A. Rubinstein (Eds.), Television and social behavior: Television and adolescent aggressiveness (pp. 239–313). Government Printing Office.
*McNaughton, D. B., Cowell, J. M., & Fogg, L. (2015). Efficacy of a Latino mother–child communication intervention in elementary schools. The Journal of School Nursing, 31(2), 126–134. https://doi.org/10.1177/1059840514526997.
Miller-Day, M., & Kam, J. A. (2010). More than just openness: Developing and validating a measure of targeted parent–child communication about alcohol. Health Communication, 25(4), 293–302. https://doi.org/10.1080/10410231003698952
Moilanen, K. L., Padilla-Walker, L. M., & Blaacker, D. R. (2018). Dimensions of short-term and long-term self-regulation in adolescence: Associations with maternal and paternal parenting and parent-child relationship quality. Journal of Youth and Adolescence, 47(7), 1409–1426. https://doi.org/10.1007/s10964-018-0825-6
*Morrison, G. M., & Zetlin, A. (1992). Family profiles of adaptability, cohesion, and communication for learning handicapped and nonhandicapped adolescents. Journal of Youth and Adolescence, 21(2), 225–240.https://doi.org/10.1007/BF01537338.
Murphy, L. K., Murray, C. B., & Compas, B. E. (2017). Topical review: Integrating findings on direct observation of family communication in studies comparing pediatric chronic illness and typically developing samples. Journal of Pediatric Psychology, 42(1), 85–94. https://doi.org/10.1093/jpepsy/jsw051
Noller, P., & Feeney, J. A. (2004). Studying family communication: multiple methods and multiple sources. In A. L. Vangelisti (Ed.), Handbook of family communication. Lawrence Erlbaum Associates.
*Noor, N. M., & Alwi, A. (2013). Stressors and well‐being in low socio‐economic status Malaysian adolescents: The role of resilience resources. Asian Journal of Social Psychology, 16(4), 292–306. https://doi.org/10.1111/ajsp.12035.
*Ochoa, G. M., Lopez, E. E., & Emler, N. P. (2007). Adjustment problems in the family and school contexts, attitude towards authority, and violent behavior at school in adolescence. Adolescence, 42(168), 779–794.
*Ochoa, L. G., Fernandez, A., Lee, T. K., Estrada, Y., & Prado, G. (2021). The intergenerational impact of adverse childhood experiences on Hispanic families: The mediational roles of parental depression and parent-adolescent communication. Family Process, 61(1), 422–435. https://doi.org/10.1111/famp.12652.
*Offrey, L. D., & Rinaldi, C. M. (2017). Parent–child communication and adolescents’ problem-solving strategies in hypothetical bullying situations. International Journal of Adolescence and Youth, 22(3), 251–267.https://doi.org/10.1080/02673843.2014.884006.
*Ohannessian, C. M., & Vannucci, A. (2020). Adolescent psychological functioning and membership in latent adolescent–parent communication dual trajectory classes. Journal of Research on Adolescence, 30(S1), 66–86.https://doi.org/10.1111/jora.12442.
*Ohannessian, C. M. (2012). Parental problem drinking and adolescent psychosocial adjustment: The mediating role of adolescent–parent communication. Journal of Research on Adolescence, 22(3), 498–511. https://doi.org/10.1111/j.1532-7795.2012.00791.x.
Olson, D. H., Sprenkle, D. H., & Russell, C. S. (1979). Circumplex model of marital and family systems I: Cohesion and adaptability dimensions, family types and clinical applications. Family Process, 18(1), 3–28. https://doi.org/10.1111/j.1545-5300.1979.00003.x
*Orm, S., Haukeland, Y., Vatne, T., Silverman, W. K., & Fjermestad, K. (2021). Prosocial behavior is a relative strength in siblings of children with physical disabilities or autism spectrum disorder. Journal of Developmental and Physical Disabilities.https://doi.org/10.1007/s10882-021-09816-7.
*Orm, S., Haukeland, Y. B., Vatne, T., & Fjermestad, K. (2022). Measuring family communication in pediatric nursing: Psychometric properties of the Parent-Child Communication Scale - Child Report (PCCS-CR). Journal of Pediatric Nursing, 62, 78–83.https://doi.org/10.1016/j.pedn.2021.10.022.
*Otero, S., Moreno-Iniguez, M., Payá, B., Castro-Fornieles, J., Gonzalez-Pinto, A., Baeza, I. et al. (2011). Twelve-month follow-up of family communication and psychopathology in children and adolescents with a first psychotic episode (CAFEPS study). Psychiatry Research, 185(1–2), 72–77.https://doi.org/10.1016/j.psychres.2009.12.007.
*O’Toole, S., Gallagher, P., Benson, A., Shahwan, A., Austin, J. K., & Lambert, V. (2021). Exploring the relationship between parent-child communication about epilepsy and psychosocial well-being. Journal of Health Psychology, 26(8), 1207–1221.https://doi.org/10.1177/1359105319871642.
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., & Moher, D. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. International Journal of Surgery, 88, 105906. https://doi.org/10.1016/j.ijsu.2021.105906
Papini, D. R., Roggman, L., & Anderson, J. (1990). Early adolescent age and gender differences in patterns of emotional self-disclosure to parents and friends. Adolescence, 25, 959–976.
*Pantaleao, A., & Ohannessian, C. M. (2019). Does coping mediate the relationship between adolescent-parent communication and adolescent internalizing symptoms? Journal of Child and Family Studies, 28(2), 479–489. https://doi.org/10.1007/s10826-018-1289-8.
Park, H. S., & Koo, H. Y. (2009). The buffering effect of parent–child communication in the relationship between stress and suicidal ideation for Korean adolescents. Journal of Korean Academy of Psychiatric and Mental Health Nursing, 18(1), 87–94.
*Park, I. J. K., & Kim, P. Y. (2012). The role of self‐construals in the link between anger regulation and externalizing problems in Korean American adolescents: Testing a moderated mediation model. Journal of Clinical Psychology, 68(12), 1339–1359.https://doi.org/10.1002/jclp.21878.
Pek, J. C. X. (2006). Parent-Child Communication, Child Report. Fast Track Project Technical Report. Retrieved from https://fasttrackproject.org/techrept/p/pcc/pcc5tech.pdf.
Peterson, C. (1990). Disagreement, negotiation and conflict resolution in families with adolescents. In P. Heaven & V. J. Callan (Eds.), Adolescence: An Australian perspective. Harcourt, Brace, Jovanovich.
*Phillips-Salimi, C. R., Robb, S. L., Monahan, P. O., Dossey, A., & Haase, J. E. (2014). Perceptions of communication, family adaptability and cohesion: A comparison of adolescents newly diagnosed with cancer and their parents. International Journal of Adolescent Medicine and Health, 26(1), 19–26.https://doi.org/10.1515/ijamh-2012-0105.
Portugal, A. P. M., & Alberto, I. M. M. (2014). Escala de Avaliação da Comunicação na Parentalidade (COMPA): Desenvolvimento e validação de uma medida da comunicação parento-filial. Avances En Psicologia Latinoamericana, 32(1), 85–103. https://doi.org/10.12804/apl32.1.2014.06
*Portugal, A. P. M., & Alberto, I. M. M. (2019). Parent–Child Communicational Characteristics: A Comparison Study between Subjects from Post-Divorce and Intact Nuclear Families. Journal of Divorce & Remarriage, 60(7), 566–582. https://doi.org/10.1080/10502556.2019.1627163.
*Prado, G., Huang, S., Cordova, D., Malcolm, S., Estrada, Y., Cano, N. et al. (2013). Ecodevelopmental and intrapersonal moderators of a family based preventive intervention for Hispanic youth: A latent profile analysis. Prevention Science, 14(3), 290–299.https://doi.org/10.1007/s11121-012-0326-x.
*Qu, W., Li, K., & Wang, Y. (2021). Early adolescents’ parent–child communication and friendship quality: A cross-lagged analysis. Social Behavior and Personality: an International Journal, 49(9), e10697. https://doi.org/10.2224/sbp.10697.
*Raimundi, M. J., Molina, M. F., Schmidt, V., & Hernández-Mendo, A. (2019). Family functioning profiles and character strengths in young elite athletes from Argentina. International Journal of Sport and Exercise Psychology, 17(1), 32–51.https://doi.org/10.1080/1612197X.2016.1189949.
*Reis, S. D., & Heppner, P. P. (1993). Examination of coping resources and family adaptation in mothers and daughters of incestuous versus nonclinical families. Journal of Counseling Psychology, 40(1), 100–108. https://doi.org/10.1037/0022-0167.40.1.100.
*Rhee, S., Chang, J., & Rhee, J. (2003). Acculturation, communication patterns, and self-esteem among Asian and Caucasian American adolescents. Adolescence, 38(152), 749–768.
*Rishel, C. W., Cottrell, L., Stanton, B., Cottrell, S., & Branstetter, S. (2010). The buffering effect of nonparental adults on the relationship between parent-adolescent communication and adolescent risk behavior. Families in Society, 91(4), 371–377.https://doi.org/10.1606/1044-3894.4031.
Ritchie, L. D., & Fitzpatrick, M. A. (1990). Family communication patterns: Measuring intrapersonal perceptions of interpersonal relationships. Communication Research, 17(4), 523–544. https://doi.org/10.1177/009365090017004007
*Ritchwood, T. D., Penn, D., Peasant, C., Albritton, T., & Corbie-Smith, G. (2017). Condom use self-efficacy among younger rural adolescents: The influence of parent-teen communication, and knowledge of and attitudes toward condoms. The Journal of Early Adolescence, 37(2), 267–283. https://doi.org/10.1177/0272431615599065.
*Rodrigues, M. A., Sanford, S. R., Rogers, M. P., Lee, K. M., Wilson, M. A., Amos, J. et al. (2020). From maternal tending to adolescent befriending: The adolescent transition of social support. American Journal of Primatology, 82(11), e23050. https://doi.org/10.1002/ajp.23050.
*Rosenthal, D., Senserrick, T., & Feldman, S. (2001). A typology approach to describing parents as communicators about sexuality. Archives of Sexual Behavior, 30(5), 463–482. https://doi.org/10.1023/A:1010235116609.
*Rosnati, R., Iafrate, R., & Scabini, E. (2007). Parent-adolescent communication in foster, inter-country adoptive, and biological Italian families: Gender and generational differences. International Journal of Psychology, 42(1), 36-45. https://doi.org/10.1080/00207590500412128.
Sales, J. M., Milhausen, R. R., Wingood, G. M., Diclemente, R. J., Salazar, L. F., & Crosby, R. A. (2008). Validation of a Parent-Adolescent Communication Scale for use in STD/HIV prevention interventions. Health Education & Behavior, 35(3), 332–345. https://doi.org/10.1177/1090198106293524
Satir, V. (1988). The new peoplemaking. Science & Behavior Books.
*Scabini, E., Lanz, M., & Marta, E. (1999). Psychosocial adjustment and family relationships: A typology of Italian families with a late adolescent. Journal of Youth and Adolescence, 28(6), 633–644.https://doi.org/10.1023/A:1021614915850.
Schmidt, V., Maglio, A., Messoulam, N., Molina, M. F., & Gonzalez, A. (2010). La comunicación del adolescente con sus padres: Construcción y validación de una escala desde un enfoque mixto. Revista Interamericana De Psicología/interamerican Journal of Psychology, 44(2), 299–311.
Schrodt, P. (2005). Family communication schemata and the circumplex model of family functioning. Western Journal of Communication, 69(4), 359–376. https://doi.org/10.1080/10570310500305539
*Schulte, M. T., Armistead, L., Marelich, W. D., Payne, D. L., Goodrum, N. M., & Murphy, D. A. (2017). Maternal parenting stress and child perception of family functioning among families affected by HIV. Journal of the Association of Nurses in AIDS Care, 28(5), 784–794.https://doi.org/10.1016/j.jana.2017.05.004.
*Schuster, R. M., Mermelstein, R., & Wakschlag, L. (2013). Gender-specific relationships between depressive symptoms, marijuana use, parental communication and risky sexual behavior in adolescence. Journal of Youth and Adolescence, 42(8), 1194–1209.
*Schwinn, T. M., Schinke, S., Fang, L., & Kandasamy, S. (2014). A web-based, health promotion program for adolescent girls and their mothers who reside in public housing. Addictive Behaviors, 39(4), 757–760.
*Sears, H. A., Robinson, B. S., & Byers, E. S. (2020). Young adolescents’ responsiveness to sexual communication with their mother: Distinguishing diverse intentions. Journal of Adolescence, 80, 136–144. https://doi.org/10.1016/j.adolescence.2020.02.006.
Shek, D. T. L., Lee, B. Μ, Lee, T. Y., & Lam, C. M. (2006). Frequency, satisfaction and quality dimensions of perceived parent-adolescent communication among Chinese adolescents in Hong Kong. International Journal of Adolescent Medicine and Health, 18(2), 259–270.
*Shin, S. H., Choi, H., Kim, M. J., & Kim, Y. H. (2010). Comparing adolescents’ adjustment and family resilience in divorced families depending on the types of primary caregiver. Journal of Clinical Nursing, 19(11–12), 1695–1706. https://doi.org/10.1111/j.1365-2702.2009.03081.x.
Sillars, A., Holman, A. J., Richards, A., Jacobs, K. A., Koerner, A., & Reynolds-Dyk, A. (2014). Conversation and conformity orientations as predictors of observed conflict tactics in parent-adolescent discussions. Journal of Family Communication, 14(1), 16–31. https://doi.org/10.1080/15267431.2013.857327
*Sillars, A., Koerner, A., & Fitzpatrick, M. A. (2005). Communication and inderstanding in parent-adolescent relationships. Human Communication Research, 31(1), 102–128. https://doi.org/10.1093/hcr/31.1.102.
*Simpson, E. G., Lincoln, C. R., & Ohannessian, C. M. (2020). Does adolescent anxiety moderate the relationship between adolescent–parent communication and adolescent coping. Journal of Child and Family Studies, 29(1), 237–249. https://doi.org/10.1007/s10826-019-01572-9.
Stamp, G. H. (2004). Theories of family relationships and a family relationships theoretical model. In A. L. Vangelisti (Ed.), Handbook of family communication. Lawrence Erlbaum Associates.
*Toombs, E., Unruh, A., & McGrath, P. (2018). Evaluating the parent-adolescent communication toolkit: Usability and preliminary content effectiveness of an online intervention. Nursing Open, 5(1), 29–36.https://doi.org/10.1002/nop2.107.
*Updegraff, K. A., Madden‐Derdich, D. A., Estrada, A. U., Sales, L. J., & Leonard, S. A. (2002). Young adolescents’ experiences with parents and friends: Exploring the connections. Family Relations, 51(1), 72–80. https://doi.org/10.1111/j.1741-3729.2002.00072.x.
Valderas, J. M., Ferrer, M., Mendívil, J., Garin, O., Rajmil, L., Herdman, M., et al. (2008). Development of EMPRO: A tool for the standardized assessment of patient-reported outcome measures. Value in Health, 11(4), 700–708. https://doi.org/10.1111/j.1524-4733.2007.00309.x
*Van Dijk, M. P., Branje, S., Keijsers, L., Hawk, S. T., Hale, W. W., & Meeus, W. (2014). Self-concept clarity across adolescence: longitudinal associations with open communication with parents and internalizing symptoms. Journal of Youth and Adolescence, 43(11), 1861–1876.https://doi.org/10.1007/s10964-013-0055-x.
Vangelisti, A. L., & Caughlin, J. P. (1997). Revealing family secrets: The influence of topic, function, and relationships. Journal of Social and Personal Relationships, 14(5), 679–705. https://doi.org/10.1177/0265407597145006
*Vannucci, A., Finan, L., Ohannessian, C. M., Tennen, H., De Los Reyes, A., & Liu, S. (2019). Protective factors associated with daily affective reactivity and instability during adolescence. Journal of Youth and Adolescence, 48(4), 771–787.https://doi.org/10.1007/s10964-018-0943-1.
Varela, R. E., Sanchez-Sosa, J. J., Biggs, B. K., & Luis, T. M. (2009). Parenting strategies and socio-cultural influences in childhood anxiety: Mexican, Latin American descent, and European American families. Journal of Anxiety Disorders, 23(5), 609–616. https://doi.org/10.1016/j.janxdis.2009.01.012
*Velazquez, E., Garthe, R. C., Pope, M., Avila, M., Romo, S., Everhart, R. S. et al. (2021). The relationship between caregiver prompting behaviors, parenting practices, and adolescent tobacco use outcomes in black families. Journal of Child and Family Studies, 30(8), 2003–2015. https://doi.org/10.1007/s10826-021-01995-3
*Wang, B., Stanton, B., Li, X., Cottrell, L., Deveaux, L., & Kaljee, L. (2013). The influence of parental monitoring and parent–adolescent communication on Bahamian adolescent risk involvement: A three-year longitudinal examination. Social Science & Medicine, 97, 161–169. https://doi.org/10.1016/j.socscimed.2013.08.013.
*Wang, F., Lin, L., Lu, J., Cai, J., Xu, J., & Zhou, X. (2020). Mental health and substance use in urban left-behind children in China: A growing problem. Children and Youth Services Review, 116, 105135. https://doi.org/10.1016/j.childyouth.2020.105135.
*Wang, F., Lin, L., Xu, M., Li, L., Lu, J., & Zhou, X. (2019). Mental health among left-behind children in rural China in relation to parent-child communication. International Journal of Environmental Research and Public Health, 16(10), 1855. https://doi.org/10.3390/ijerph16101855.
*Weber, M., Alvariza, A., Kreicbergs, U., & Sveen, J. (2019). Family communication and psychological health in children and adolescents following a parent’s death from cancer. Omega-Journal of Death and Dying, 83(3), 630–648. https://doi.org/10.1177/0030222819859965.
*White, F. A. (2000). Relationship of family socialization processes to adolescent moral thought. The Journal of Social Psychology, 140(1), 75–91.
*White, F. A., & Matawie, K. M. (2004). Parental morality and family processes as predictors of adolescent morality. Journal of Child and Family Studies, 13(2), 219–233. https://doi.org/10.1023/B:JCFS.0000015709.81116.ce.
*Wu, C., & Chao, R. K. (2011). Intergenerational cultural dissonance in parent–adolescent relationships among Chinese and European Americans. Developmental Psychology, 47(2), 493–508. https://doi.org/10.1037/a0021063.
*Xia, Y. R., Xie, X., Zhou, Z., Defrain, J., Defrain, J., & Combs, R. (2004). Chinese adolescents’ decision-making, parent-adolescent communication and relationships. Marriage & Family Review, 36(1–2), 119–145. https://doi.org/10.1300/J002v36n01_06.
*Xiao, Z., Li, X., & Stanton, B. (2011). Perceptions of parent-adolescent communication within families: It is a matter of perspective. Psychology, Health & Medicine, 16(1), 53–65. https://doi.org/10.1080/13548506.2010.521563.
Xin, M., Chen, P., Liang, Q., Yu, C., Zhen, S., & Zhang, W. (2021). Cybervictimization and adolescent internet addiction: A moderated mediation model. International Journal of Environmental Research and Public Health, 18(5), 2427. https://doi.org/10.3390/ijerph18052427
*Yang, H., Stanton, B., Li, X., Cottrel, L., Galbraith, J., & Kaljee, L. (2007). Dynamic association between parental monitoring and communication and adolescent risk involvement among African-American adolescents. Journal of the National Medical Association, 99(5), 517–524.
*Yang, J., Campo, S., Ramirez, M., Krapfl, J. R., Cheng, G., & Peek-Asa, C. (2013). Family communication patterns and teen drivers’ attitudes toward driving safety. Journal of Pediatric Health Care, 27(5), 334–341. https://doi.org/10.1016/j.pedhc.2012.01.002
Yang, X., & Zou, H. (2008). Characteristics of parent-adolescent communication. Psychological Development and Education (chinese), 24, 49–54.
*Ying, L., Ma, F., Huang, H., Guo, X., Chen, C., & Xu, F. (2015). Parental monitoring, parent-adolescent communication, and adolescents’ trust in their parents in China. PLoS ONE, 10(8), e0134730. https://doi.org/10.1371/journal.pone.0134730.
*Ying, L., Yan, Q., Shen, X., Jia, X., & Lin, C. (2019). Economic pressure and loneliness in migrant children in China: The mediating roles of parent-child communication and parental warmth. Child Psychiatry & Human Development, 50(1), 142–149. https://doi.org/10.1007/s10578-018-0827-3.
*Ying, L., Zhou, H., Yu, S., Chen, C., Jia, X., Wang, Y. et al. (2018). Parent-child communication and self-esteem mediate the relationship between interparental conflict and children’s depressive symptoms. Child Care and Health Development, 44(6), 908–915. https://doi.org/10.1111/cch.12610.
*Yoon, D. P. (2000). Causal modeling predicting psychological adjustment of Korean-born adolescent adoptees. Journal of Human Behavior in the Social Environment, 3(3–4), 65–82. https://doi.org/10.1300/J137v03n03_06.
*Young, D. W., & Childs, N. A. (1994). Family images of hospitalized adolescents: The failure to generate shared understandings. Psychiatry, 57(3), 258–267. https://doi.org/10.1080/00332747.1994.11024689.
Youngstrom, E. A., VanMeter, A., Frazier, T. W., Hunsley, J., Prinstein, M. J., Ong, M. L., & Youngstrom, J. K. (2017). Evidence-based assessment as an integrative model for applying psychological science to guide the voyage of treatment. Clinical Psychology: Science and Practice, 24, 331–363. https://doi.org/10.1111/cpsp.12207
*Yu, S., Clemens, R., Yang, H., Li, X., Stanton, B., Deveaux, L. et al. (2006). Youth and parental perceptions of parental monitoring and parent-adolescent communication, youth depression, and youth risk behaviors. Social Behavior and Personality, 34(10), 1297–1310. https://doi.org/10.2224/sbp.2006.34.10.1297.
*Zhang, Y., Huang, J., & Wang, Y. (2019). Parent–adolescent communication and Chinese adolescents’ self-esteem: A cross-lagged model. Social Behavior and Personality. An International Journal, 47(10), e8416. https://doi.org/10.2224/sbp.8416.
*Zhou, X., Zhen, R., & Wu, X. (2021). Insecure attachment to parents and PTSD among adolescents: the roles of parent–child communication, perceived parental depression, and intrusive rumination. Development and Psychopathology, 33(4), 1290–1299.https://doi.org/10.1017/S0954579420000498.
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no financial or proprietary interests in any material discussed in this article.
Ethical approval
This work does not utilize human subject data and no ethical approval is required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zapf, H., Boettcher, J., Haukeland, Y. et al. A Systematic Review of Parent–Child Communication Measures: Instruments and Their Psychometric Properties. Clin Child Fam Psychol Rev 26, 121–142 (2023). https://doi.org/10.1007/s10567-022-00414-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10567-022-00414-3