
Abstract
Our objective was to assess the influence of different levels of exposure to dynamic training on right ventricular (RV) structure, function and mechanics in elite male athletes. We recruited 492 male elite athletes aged between 18 and 30 years old. Athletes were grouped according to their sporting discipline using the Mitchell Classification as Low Dynamic (LD), Moderate Dynamic (MD) or High Dynamic (HD). All participants underwent 2D, Doppler, tissue Doppler and strain (ε) echocardiography with a focused and comprehensive assessment of the right heart. Athletes involved in MD sports had the largest absolute RV chamber size and when scaled to body size RVOT PLAX, RVOT2, RVD1 and RVD3 were larger in HD compared to MD and LD athletes. There were no between group differences in conventional RV functional indices as well as global RV ε (LD: − 23.4 ± 3.1 vs. MD: − 22.7 ± 2.7 vs. HD: − 23.5 ± 2.6, %) and strain rate (P > 0.01). The base to apex ε gradient in the RV septum was lower in the MD athletes compared to HD and LD due to a lower apical septal ε which significantly correlated with absolute RV chamber size. After scaling for body size there was evidence of larger RV cavities in both MD and HD athletes compared to LD athletes. Global RV function, ε and strain rate were not different between groups. MD athletes had lower apical septal ε that contributed to a smaller base-to-apex ε gradient that is partially associated with larger absolute RV chamber dimensions.
Similar content being viewed by others
Explore related subjects
Find the latest articles, discoveries, and news in related topics.Avoid common mistakes on your manuscript.
Introduction
The term athlete’s heart (AH) is used to describe the physiological cardiac adaptation in response to exercise training [1,2,3,4]. Many studies of AH have focused on the left ventricle but the right ventricle (RV) also undergoes physiological remodelling due to the hemodynamic overload associated with training [2, 5,6,7]. The nature of RV remodelling and functional change associated with prolonged training exposure often leads to a phenotypical presentation beyond normal limits that can create a diagnostic challenge when attempting to differentiate the AH from pathological cardiac adaptation associated with diseases that predispose an athlete to an increased risk of sudden cardiac death (SCD) [8,9,10].
In any individual, cardiac adaptation is influenced by a range of training exposure and individual factors [4]. A key mediating variable is the nature of the training exposure (mode, intensity, duration and volume) [4]. To date many studies have attempted to differentiate the cardiac response to endurance versus resistance training [2, 11] with most data supportive of a significantly greater cardiac adaptation to dynamic or endurance based exercise training [2, 7, 11,12,13] with limited or no significant cardiac adaptation to resistance training [11, 12]. In addition, recent work has demonstrated that dynamic exercise training is the primary driver for cardiac adaptation [11, 13]. The American College of Cardiology Task Force/Mitchell classification [14, 15] categorized sporting disciplines into nine main groups based on their physiological demands with a matrix of 3 levels of dynamic training (low, medium and high) as well as 3 levels of static training (low, medium and high). Given the likely impact of dynamic or endurance training, a clear assessment of RV phenotype in athletes grouped in low, medium and high dynamic training exposure would be valuable to inform the nature of RV remodelling in athletes. Another factor that impacts on the interpretation of AH data is the body size and composition of the athletes. To date most AH studies have presented absolute RV structural data or indices scaled linearly to body surface area (BSA) [10]. It is well established that allometric scaling is recommended to provide accurate size-independent measures of cardiac size that will aid accurate interpretation [16, 17].
Technical developments have also had a significant impact on measurement of the AH phenotype. Echocardiography plays an important role in the assessment of RV structure and function. Normal resting RV function has been reported in most athlete studies [10, 11, 13]. Technical advancements such as tissue-Doppler and strain (ε) imaging have led to new global and regional indices of RV function and mechanics that may provide extra diagnostic tools in the differentiation of AH from pathological cardiac adaptation [11]. ε imaging has highlighted subtle regional differences in RV mechanics, particularly in those athletes with a more marked RV phenotype [5, 18]. In addition, much of RV ε data has been reported from the RV lateral wall with limited attention given to septal contribution to RV function.
On the basis of these questions and the application of tissue Doppler and ε imaging, the aim of this study was to establish the nature and extent of RV structural, functional and mechanical presentation in elite male athletes involved in sports categorised with different levels of dynamic workload in accordance with Mitchell classification [14, 15].
Methods
Study design
A prospective cross-sectional study design was performed. Male elite athletes between the age of 18–30 years were included if they were competitive at National level and had no history, signs or symptoms of cardiovascular, metabolic, renal or respiratory disease. No athlete was taking prescribed medication and there was no evidence of a family history of (SCD) or unexplained death under the age of 40 years. The athletes were grouped according to sporting discipline as per Mitchell classification: Low dynamic (LD)—exercise training exposure at < 50% VO2max (including cricket, equestrian, motorcycling, martial arts, and weightlifting); Moderate dynamic (MD)—exercise exposure at 50–75% VO2max (including rugby); High dynamic (HD)—exercise training exposure at > 75% VO2max (including soccer, basketball, ice hockey, boxing, cycling, rowing and triathlon). Ethics approval was obtained by the Ethics Committee of the Liverpool John Moores University and all athletes provided written informed consent.
Athletes attended the echocardiography laboratory for a single visit, ensuring that they had not undertaken any exercise training 6 h prior to assessment and had not consumed alcohol and caffeine for the previous 24 h. The athletes initially completed a personal and family medical history questionnaire and had anthropometric assessment of height and weight, measurement of brachial artery blood pressure, a 12-lead Electrocardiogram (ECG) and a transthoracic echocardiogram performed. Athletes were excluded if after the completion of a health questionnaire, consultant examination, 12-lead ECG, full echocardiographic examination and/or any other clinically relevant follow-up test they had a definitive or suggestive diagnosis of cardiovascular disease [19].
Procedures
Anthropometric assessment
All athletes were assessed for height and body mass using a standard scale and stadiometer (SECA 764, Birmingham, UK). Body surface area (BSA) was calculated by using a standardised formula [20]. Systolic and diastolic blood pressure were recorded using an automated sphygmomanometer (DINAMAP 300, GE Medical System, Milwaukee, Wisconsin, USA) after 5 min of quiet seated rest.
12-Lead ECG
A standard resting 12-lead ECG (CardioExpress SL6, Spacelabs Healthcare, Washington US) was carried out in accordance with American Heart Association guidelines [19].
Echocardiographic assessment
Echocardiographic examination was performed using a Vivid Q ultrasound machine (GE Healthcare, Horten, Norway) with a 2.5–5 MHz transducer with the subject in the left lateral decubitas position. All acquisitions were made by two experienced sonographers using an echocardiography protocol in accordance with the American Society of Echocardiography [21, 22]. Offline analysis was performed, after storing the images in a raw Digital Imagine and Communications in Medicine format and exported, using commercial available software (EchoPAC V.110.0.2; GE Helathcare, Horten, Norway). All measurements were made in accordance with American Society of Echocardiography guidelines [22] by the same sonographers.
Conventional 2D, Doppler and tissue Doppler measures
The size of the RV outflow tract was assessed at the proximal (RVOT-PLAX; RVOT1) and distal (RVOT2) levels from the parasternal long and short axis orientations view. RV inflow dimensions were recorded at the base (RVD1), mid-cavity (RVD2) as well as the length from base to apex (RVD3) from a modified apical four chamber orientation. In the same view, RV area in diastole (RVDA) and systole (RVSA) were obtained by tracing the RV endocardium both in systole and diastole, allowing the calculation of fractional area change (RVFAC). RV wall thickness (RVWT) was measured from a subcostal view at mid wall level. For clinical utility, all structural variables were scaled to individual differences in BSA using a standard linear model. That aside, it is well established that biological systems follow a non-linear relationship and hence all indices were also scaled allometrically according to the laws of geometrically similarity. This data provides size independent values that allow direct comparison across athletes of different body composition and involves scaling linear dimensions to BSA0.5 and area measurements directly to BSA [16].
RV longitudinal function was determined using M-mode derived tricuspid annular plane systolic excursion (TAPSE) and pulsed wave TDI, at the RV lateral wall tricuspid annulus to obtain peak myocardial velocities in systole (S’), early diastole (E’) and late diastole (A’). Pulsed wave Doppler of the RV outflow tract allowed the assessment of RV velocity time interval (RVOT VTI).
Speckle tracking echocardiography measures
The modified apical four-chamber view was used for the assessment of longitudinal RV lateral wall and septal ε and strain rate (SR). To provide optimal endocardial delineation, images were optimised using depth, gain, compression and sector width. Frame rates were set between 80 and 90 frames per second and the focal point was positioned mid cavity to reduce the impact of beam divergence. For offline analysis, pulmonary valve closure (PVC) was obtained from the pulsed wave Doppler signal at the RV outflow tract. A region of interest was placed around the RV basal lateral wall through to basal septum encompassing the mid and apical wall segments. The software automatically tracked the base, mid and apical segments and presented an assessment of tracking quality with segments being excluded if deemed unacceptable. Regional peak and time to peak RV ε, peak systolic SR (SRS’), peak early diastolic SR (SRE’) and peak late diastolic SR (SRA’) were obtained for each of the 6 myocardial segments and a global value was determined as an average of the base, mid and apical wall segments. A base to apex ε gradient was calculated for both the septum and the lateral wall as the difference between the peak values at both sites.
Temporal ε and SR was obtained by exporting the raw data to an excel spreadsheet (Excel, Microsoft Corp, Washington, US) and the global temporal values underwent cubic spline interpolation in both systole and diastole phase. The ε values were split into 5% increments of the cardiac cycle ensuring the raw peak ε and SR value was included.
Statistical analysis
Statistical analysis was performed using Statistical Package for the Social Sciences (SPSS) (version 23.0, Chicago IL, USA). All parameters are presented as mean ± SD. Normal distribution was confirmed using a Kolmogorov–Smirnov test. Analysis between groups was established using one-way ANOVA and Bonferroni post hoc test for multiple comparison to estimate pairwise differences between groups. Where data was not normally distributed ANOVA on ranks (Krusakal–Wallis) followed by the Mann–Whitney test for pairwise comparisons were employed. To minimize type 1 error rate inflation due to multiple testing, statistical significance was defined as two-sided p < 0.01. Where derived ε and SR values were significantly different between groups a standard bivariate correlation was used to establish any relationship to absolute RV chamber size.
Results
492 male athletes were recruited (LD: n = 48; MD: n = 157; HD: n = 287) through a range of pre-participation screening events and none were excluded after appropriate follow-up testing. Participant ethnicity was 84% White, 9% Black, 1% Asian, and 6% Mixed. All athletes were matched for training duration and weekly training hours (Table 1). MD athletes had significantly greater weight and BSA compared to both LD and HD groups.
Absolute and scaled RV structural parameters are presented in Table 2. MD athletes had significantly larger absolute values for RVOT1, RVOT2, RVDA and RVWT than both HD and LD whilst also having larger values of RVOT-PLAX, RVD1 and RVSA when compared to LD alone. HD had significantly larger absolute RVOT2, RVD1, and RVDA compared to LD. Following allometric scaling RVOT-PLAX, RVOT2, RVD1, and RVD3 were larger in HD compared to MD and LD athletes, RVDA was larger in MD and HD compared to LD and RVSA was larger for HD compared with LD athletes.
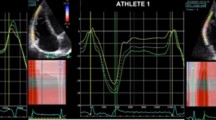
Standard RV functional data as well as global ε and SR data are presented Table 3. There were no significant differences between groups for functional and mechanical indices derived from standard conventional 2D, tissue Doppler and ε imaging. Segmental mechanical analysis determined that MD athletes had significantly lower ε in the apical septal wall segment compared to both the HD and LD groups. This contributed to a significantly lower base-apex ε gradient in the septal wall of MD athletes (Table 4). Assessment of the temporal distribution of global ε and SR across the cardiac cycle shows no significant differences between the three groups and is presented in Fig. 1.

Right ventricular temporal curves of a1 mean longitudinal ε and a2 strain rate compared between Low, Moderate and High dynamic classifications
There were significant positive, but small correlations between the apical septal ε and RVOT-PLAX (r = 0.14, P = 0.014), RVOT1 (r = 0.11, P = 0.041), RVOT2 (r = 0.13, P = 0.015) and RVDA (r = 0.13, P = 0.016). Apical lateral ε was correlated with RVOT2 (r = 0.12, P = 0.03).
Discussion
The key findings from this study were (1) athletes involved in sports with MD and HD training exposure had generally larger absolute and scaled RV structural indices than athletes with LD training exposure, (2) there were no between differences in conventional RV functional indices as well as global RV ε and SR, (3) athletes with MD training exposure had a smaller base to apex ε gradient in both septal and lateral walls largely due to reduced apical ε and this appears to be partly related to absolute RV chamber size.
Right ventricular structure
It has been established that exercise training in elite male athletes causes RV structural adaptation [2, 6, 9, 23,24,25,26], which is likely driven by changes in cardiac load [27]. During acute dynamic exercise the body employs large muscle groups that require substantial O2 demand. This demand is met by increased cardiac work elevating both LV and RV cardiac output. The long-term adaptation to this acute loading is a significant dilation of the ventricular cavities and this is clearly observed in the RV of the HD and MD athletes in this study. This RV data supports a range of previous research in largely endurance-based athletes [2, 13, 26, 28] as well as data from a training study Spence et al. [28] that identified that participants engaged in a HD exercise training programme had greater RV adaptation than those with LD exercise training. A recent meta-analysis partially supports our work with strength trained athletes (LD) having smaller RV inflow chamber size [26]. Interestingly, unlike our data, this meta-analysis demonstrates no training specific differences in the RV outflow. The absolute RV structural data in this study were generally greater in the MD athletes, which may be somewhat counterintuitive based on training loads. It is important to note, however, that the MD athletes were physically bigger and that after scaling both HD and MD athletes had larger RV structural indices than the LD athletes. Utomi et al. [11] undertook a meta-analysis detailing greater RV enlargement in endurance athletes compared to control participants, however, there was a positive and significant association in the regression model between RV parameters and BSA. Our data confirm the importance and utility of appropriate scaling of cardiac data [17]. It is interesting to note that many of the MD athletes were elite rugby football league players. As well as being bigger athletes, it may be pertinent to question whether the American College of Cardiology/Mitchell Classification have placed this athletic group in the wrong category. It is pertinent to recommend that all RV structural indices in the athlete should be indexed appropriately to provide size independence.
Right ventricular function
Our conventional echocardiographic data demonstrated no difference in global RV function, during systole or diastole, between groups undertaking different amounts of dynamic training. Although there is evidence to suggest athletes have different RV function than non-athlete controls [2, 5, 29,30,31,32], there are limited data between different athlete groups. Those studies that have compared athletes largely report no difference in TAPSE [2, 13, 26, 33], RVFAC [2, 25, 34] and myocardial tissue velocities [2, 7, 34]. Similar to these conventional indices of global RV function there was no difference in peak global ε and SR between athlete groups which supports some previous studies [2, 13, 26].
There is less data in the literature reporting regional RV ε and SR in dynamically trained athletes. The observation of reduced apical ε in the RV septal wall segment in MD athletes is a novel finding and appears to be related, in part, to RV size and potentially body size. Teske et al. [5] and La Gerche et al. [18] both demonstrated reduced RV basal SR in athletes with larger RV area and attributed this to RV geometry, heart rate and resting reserve [5, 18]. Teske et al. [35] reported a reduction in ε and SR in basal and mid segments in endurance athletes with marked RV dilatation as normal physiological adaptation [35]. In addition, during the competitive season, D’Ascenzi et al. [36] documented no significant differences (P > 0.14) in global ε among 29 top-level athletes. They did however demonstrate an increase in RV apical wall ε at both mid-season and end-season which was associated to RV mid-cavity, RVEDA, RVESA and SV [36]. The impact of hand grip exercise on RV apical ε has also been demonstrated in an acute setting and may provide some evidence for this type of stimulus leading to chronic functional adaptation [37]. During maximal exercise the RV has the ability to increase its contractility to compensate for the increase in work [38] and it is likely that the changes in the RV apical segment ε is due to the changes in training intensity and chamber size. The data from the current study demonstrates an association between apical septal ε and RV outflow tract, rather than the inflow/sinus region of the RV. This might provide some explanation for the reduction in apical deformation, rather than that of basal segments between different dynamic sport discipline. Evidence shows crisscross fibres within the apical interventicular septum which contribute to the RVOT structure [39]. Therefore, any structural changes in the RVOT might contribute to the apical ε in this wall segment. It is clear that RV size accounts for only a small portion of the variance in the apical septal ε and thus further work is required to provide further mechanistic insight.
Clinical/imaging implications
It is documented that 3–10% of all sudden cardiac deaths in young athletes is due to arrhythmogenic right ventricular cardiomyopathy (ARVC) [40]. In this regard, differentiation of RV physiological adaptation from pathological changes caused by ARVC is of utmost importance in pre-participation cardiac screening programs. This study provides valuable information on RV structural and functional adaptation in athletes undertaking different amounts of dynamic load exercise training, which may aid in specific screening programs. This study presents absolute and scaled RV structure that shows the importance of indexing to provide size-independent RV structural data.
These data demonstrate that despite marked RV dimensional remodelling, exercise-induced RV adaptation in a young male elite athlete population is not associated with any degradation in function and thus does not support the theory of an exercise-induced ARVC. It is important to note that any potential mal-adaptation occurs in sporadic cases and may be dependent on long term repeated exposure and insufficient recovery time [41].
The addition of novel non-invasive imaging techniques may provide unique insights into the RV AH phenotype particularly the potential use of speckle-tracking echocardiography [42, 43]. Our data also demonstrates the use of both septal and free wall ε for assessment of global RV function. This is challenging due to the inability to clearly define which portion of the septum contributes to the RV. It is therefore apparent that further work in athletic and non-athletic populations should aim to establish the extend and contribution of septal and free wall deformation to global RV mechanics.
Limitations
This study explored the effect of three different levels of dynamic exercise load upon the RV without taking into account the static components for each level (nine box Mitchell classification), which would help determine the effect of varying static and dynamic components of each sport on cardiac adaptation. There is some discrepancy in sample size in the 3 groups but larger samples in all groups would have improved the power and generalisability of the data. The addition of a sedentary control group would also provide some benefit. Furthermore, this study only investigated RV remodelling among male athletes It is apparent that further study related to gender specific adaptation would be valuable.
Conclusion
This study compared the effects of 3 different levels of dynamic exercise training (using the Mitchell classification) on RV structure, function and mechanics. RV morphology was generally larger in HD athletes, compared to MD and LD groups when data were allometrically scaled to BSA. Despite no significant differences in RV function between the three groups, there was reduction in regional ε in the apical septal wall segment which may partially be explained by greater absolute RV dimensions and body size in MD athletes.
References
Pluim BM, Zwinderman AH, Van Der Laarse A, van der Wall EE (2000) The athlete’s heart: a meta-analysis of cardiac structure and function. Circulation 101:336–344
D’Andrea A, Riegler L, Golia E et al (2013) Range of right heart measurements in top-level athletes: the training impact. Int J Cardiol 164:48–57
De Luca A, Stefani L, Galanti G (2013) Right ventricle chamber of young trained athletes: morphology and function. Asian J Sports Med 4:281–288
Brown B, Somauroo J, Green DJ et al (2017) The complex phenotype of the athlete’s heart: implications for preparticipation screening. Exerc Sport Sci Rev 45:96–104
Teske AJ, Cox MG, De Boeck BW, Doevendans P, Hauer RN, Cramer MJ (2009) Echocardiographic tissue deformation imaging quantifies abnormal regional right ventricular function in arrhythmogenic right ventricular dysplasia/cardiomyopathy. J Am Soc Echocardiogr 22:920–927
Oxborough D, Sharma S, Shave R et al (2012) The right ventricle of the endurance athlete: the relationship between morphology and deformation. J Am Soc Echocardiogr 25:263–271
Pagourelias V, Kouidi E, Efthimiadis G, Deligiannis A, Geleris P, Vasilikos V (2013) Right atrial and ventricular adaptations to training in male Caucasian athletes: an echocardiographic study. J Am Soc Echocardiogr 26:1344–1352
Maron BJ, Pelliccia A (2006) Contemporary reviews in cardiovascular medicine the heart of trained athletes cardiac remodeling and the risks of sports, including sudden death. Circulation 114:1633–1644
D’Andrea A, Caso P, Bossone E, Scarafile R, Riegler L, Salvo G (2010) Right ventricular myocardial involvement in either physiological or pathological left ventricular hypertrophy: an ultrasound speckle tracking two-dimensional strain analysis. Eur J Echocardiogr 11:492–500
Utomi V, Oxborough D, Ashley E et al (2014) Predominance of normal left ventricular geometry in the male “athlete”s heart’. Heart 100:1264–1271
Utomi V, Oxborough D, Whyte GP et al (2013) Systematic review and meta-analysis of training mode, imaging modality and body size influences on the morphology and function of the male athlete’s heart. Heart 99:1727–1733
Spence AL, Naylor LH, Carter HH et al (2013) Does echocardiography accurately reflect CMR-determined changes in left ventricular parameters following exercise training ? A prospective longitudinal study. J Appl Physiol 114:1052–1057
Oxborough D, Heemels A, Somauroo J et al (2016) Left and right ventricular longitudinal strain-volume/area relationships in elite athletes. Int J Cardiovasc Imaging 32:1199–1211
Mitchell JH, Haskell W, Snell P, Van Camp SP (2005) Task force 8: classification of sports. J Am Coll Cardiol 45:1364–1367
Levine B, Kovacs RJ, Link MS, Maron MS (2015) Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities: task force 1: classification of sports: dynamic, static, and impact. J Am Coll Cardiol 66:2350–2355
Batterham AM, George KP, Whyte G, Sharma S, McKenna W (1999) Scaling cardiac structural data by body dimensions: a review of theory, practice, and problems. Int J Sports Med 20:495–502
Dewey FE, Rosenthal D, Murphy DJ, Froelicher VF, Ashley EA (2008) Contemporary reviews in cardiovascular medicine does size matter? Clinical applications of scaling cardiac size and function for body size. Circulation 117:2279–2287
La Gerche A, Burns AT, D’Hooge J, Macisaac AI, Heidbüchel H, Prior DL (2012) Exercise strain rate imaging demonstrates normal right ventricular contractile reserve and clarifies ambiguous resting measures in endurance athletes. J Am Soc Echocardiogr 25:253–262
Sharma S, Drezner JA, Baggish A et al (2017) International Recommendations for Electrocardiographic Interpretation in Athletes. J Am Coll Cardiol 69:1057–1075
Mosteller R (1987) Simplified calculation of body surface area. N Engl J Med 317:1098
Rudski LG, Lai WW, Afilalo J et al (2010) Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography. J Am Soc Echocardiogr 23:685–713
Lang RM, Badano LP, Mor-avi V et al (2015) Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the american society of echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr 28:1–39
Zaidi A, Panoulas VF, Sheikh N, Gati S (2013) Physiologic right ventricular adaptation in elite athletes of African and Afro-Caribbean Origin. Circulation 127:1783–1792
D’Ascenzi F, Cameli M, Padeletti M et al (2013) Characterization of right atrial function and dimension in top-level athletes: a speckle tracking study. Int J Cardiovasc Imaging 29:87–94
D’Ascenzi F, Pisicchio C, Caselli S et al (2017) RV remodeling in olympic athletes. J Am Coll Cardiol Img 10:385–393
D’Ascenzi F, Pelliccia A, Solari M et al (2017) Normative reference values of right heart in competitive athletes: a systematic review and meta-analysis. J Am Soc Echocardiogr 30:845–858
Galderisi M, Cardim N, Andrea AD et al (2015) The multi-modality cardiac imaging approach to the Athlete’s heart: an expert consensus of the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging 16:353
Spence AL, Naylor LH, Carter HH et al (2011) A prospective randomised longitudinal MRI study of left ventricular adaptation to endurance and resistance exercise training in humans. J Physiol 22:5443–5452
Erol M, Karakelleoglu S (2002) Assessment of right heart function in the athlete’s heart. Hear Vessel 16:175–180
Caso P, Galderisi M, Andrea AD et al (2002) Analysis by pulsed Doppler tissue imaging of venticular interaction in long-distance competitive swimmers. J Am Coll Cardiol 9149(2):193–197
D’Andrea A, Caso P, Sarubbi B et al (2003) Right ventricular myocardial adaptation to different training protocols in top-level athletes. Echocardiography 20:329–336
D’Andrea A, Caso P, Scarafile R et al (2007) Biventricular myocardial adaptation to different training protocols in competitive master athletes. Int J Cardiol 115:342–349
Baggish AL, Wang F, Weiner RB et al (2008) Training-specific changes in cardiac structure and function: a prospective and longitudinal assessment of competitive athletes. J Appl Physiol 104:1121–1128
Moro A, Okoshi M, Padovani C, Okoshi K (2013) Doppler echocardiography in athletes from different sports. Med Sci Monit 19:187–193
Teske AJ, Prakken NH, De Boeck BW et al (2009) Echocardiographic tissue deformation imaging of right ventricular systolic function in endurance athletes. Eur Heart J 8:969–977
D’Ascenzi F, Pelliccia A, Corrado D et al (2015) Right ventricular remodelling induced by exercise training in competitive athletes. 17:301–307
Stefani L, Pedrizzetti G, De Luca A et al (2009) Real-time evaluation of longitudinal peak systolic strain (speckle tracking measurement) in left and right ventricles of athletes. Cardiovasc Ultrasound 7:17
La Gerche A, Heidbuchel H, Burns AT et al (2011) Disproportionate exercise load and remodeling of the athlete’s right Ventricle. Med Sci Sport Exerc 6:974–981
Cho EJ, Jiamsripong P, Calleja AM et al (2009) Right ventricular free wall circumferential strain reflects graded elevation in acute right ventricular afterload. Am J Physiol Heart Circ Physiol 296:H413-H420
Harmon KG, Drezner JA, Maleszewski JJ et al (2014) Pathogeneses of sudden cardiac death in national collegiate athletic association athletes. Circ Arrhythmia Electrophysiol 7:198–204
La Gerche A, Burns AT, Mooney DJ et al (2012) Exercise-induced right ventricular dysfunction and structural remodelling in endurance athletes. Eur Heart J 8:998–1006
D’Ascenzi F, Caselli S, Solari M et al (2016) Novel echocardiographic techniques for the evaluation of athletes’ heart: A focus on speckle-tracking echocardiography. Eur J Prev Cardiol 23:437–446
Pelliccia A, Caselli S, Sharma S et al (2017) European association of preventive cardiology (EAPC) and European Association of Cardiovascular Imaging (EACVI) joint position statement: recommendations for the indication and interpretation of cardiovascular imaging in the evaluation of the athlete. Eur Heart J. https://doi.org/10.1093/eurheartj/ehx532
Funding
The primary author received government sponsorship funding from ministry of health of Kuwait.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
There is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Qasem, M., George, K., Somauroo, J. et al. Influence of different dynamic sporting disciplines on right ventricular Structure and function in elite male athletes. Int J Cardiovasc Imaging 34, 1067–1074 (2018). https://doi.org/10.1007/s10554-018-1316-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10554-018-1316-2