
Abstract
Objectives
Pre-clinical studies have shown that iron can be carcinogenic, but few population-based studies investigated the association between markers of the iron metabolism and risk of cancer while taking into account inflammation. We assessed the link between serum iron (SI), total-iron binding capacity (TIBC), and risk of cancer by levels of C-reactive protein (CRP) in a large population-based study (n = 220,642).
Methods
From the Swedish Apolipoprotein Mortality Risk (AMORIS) study, we selected all participants (>20 years old) with baseline measurements of serum SI, TIBC, and CRP. Multivariate Cox proportional hazards regression was carried out for standardized and quartile values of SI and TIBC. Similar analyses were performed for specific cancers (pancreatic, colon, liver, respiratory, kidney, prostate, stomach, and breast cancer). To avoid reverse causation, we excluded those with follow-up <3 years.
Results
We found a positive association between standardized TIBC and overall cancer [HR 1.03 (95 % CI 1.01–1.05)]. No statistically significant association was found between SI and cancer risk except for postmenopausal breast cancer [HR for standardized SI 1.09 (95 % CI 1.02–1.15)]. The association between TIBC and specific cancer was only statistically significant for colon cancer [i.e., HR for standardized TIBC: 1.17 (95 % CI 1.08–1.28)]. A borderline interaction between SI and levels of CRP was observed only in stomach cancer.
Conclusions
As opposed to pre-clinical findings for serum iron and cancer, this population-based epidemiological study showed an inverse relation between iron metabolism and cancer risk. Minimal role of inflammatory markers observed warrants further study focusing on developments of specific cancers.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Pre-clinical studies have illustrated several carcinogenic properties of the iron metabolism. Excess iron yields hydroxyl radicals, which may cause conformational changes in the nuclear and cytoplasm membranes and results in activation of oncogenes [1, 2]. Moreover, iron can sustain the growth of neoplastic cells by suppressing host defences or inflammation [2]. In addition, iron functions as a vital nutrient for unlimited cell multiplication and is required for the unlimited and unrestricted proliferation of cells [2].
Several studies have reported that there is no correlation between dietary iron intake and risk of different types of cancer including pancreatic, breast, endometrial, and colorectal [3, 4]. Additionally, fewer studies assessed serum levels of markers of the iron metabolism. One study, a nested case–control study in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial, prospectively evaluated dietary intake and serum measures of iron, ferritin, transferrin, and total iron-binding capacity (TIBC) in relation to colorectal cancer (n = 356). They found a positive association with red meat intake, an inverse association with serum TIBC, but no association with the other serum markers [5]. In contrast, a study of over 6,000 US adults by Wu et al. [6] determined that people with higher levels of serum iron had an increased risk of dying from cancer. Other studies have found no correlation between serum iron and cancer [7], but none of these studies took the inflammatory state of the patient into consideration.
Inflammation is thought to be one of the underlying mechanisms linking iron metabolism and carcinogenesis as iron is involved in both processes. For instance, Kooistra et al. [8] showed that the absorption of iron from the gut was impaired in patients with elevated levels of C-reactive protein (CRP), which in turn has been positively linked with risk of cancer [9]. Moreover, it is important to note that the relationship between serum iron and TIBC can vary depending on the status of the individual. For example, in iron deficient anaemia, TIBC is high and serum iron is low. However, under conditions of inflammation—leading to anaemia of chronic disease (ACD)—the influence of hepcidin results in low serum iron due to iron being bound intracellularly with ferritin, and this is concomitant with low TIBC due to decreased synthesis of transferrin [10]. This results in a positive correlation between SI and TIBC.
To improve our understanding of iron metabolism in the context of carcinogenesis and inflammation, we examined possible associations between serum iron (SI), TIBC, CRP, and cancer risk in a prospective cohort study of 220,642 persons of whom 9,269 were diagnosed with cancer.
Methods
Study population and data collection
The Central Automation Laboratory (CALAB) database (1985–1996) includes laboratory measurements obtained from 351,487 men and 338,101 women, mainly from the greater Stockholm area (Sweden). All individuals were either healthy individuals referred for clinical laboratory testing as part of a general health check-up or outpatients referred for laboratory testing. No individuals were inpatients at the time their blood samples were taken, and none were excluded due to disease symptoms or because of treatment. Apart from the information on blood testing, no personal data were included in the CALAB database [11]. This database was linked to several Swedish national registries such as the National Cancer Register, the Hospital Discharge Register, the Cause of Death Register, the consecutive Swedish Censuses during 1970–1990, and the National Register of Emigration by using the Swedish 10-digit personal identity number to provide information on socio-economic status (SES), vital status, cancer diagnosis, and emigration. This linkage of national registers to the CALAB database is called AMORIS and has been described in detail elsewhere [11–17]. This study complied with the Declaration of Helsinki, and the ethics review board of the Karolinska Institute approved the study.
We selected all participants aged 20 or older with baseline measurements of SI, TIBC, and CRP (n = 220,642) who were free from cancer at baseline and were not diagnosed with cancer or died within 3 years after baseline. Follow-up time was defined as time from iron measurement until date of cancer diagnosis, emigration, death, or study closing date (31st of December 2002), whichever occurred first. The CALAB database also contained information on age and fasting status at time of blood sampling. All other information was retrieved from the above-listed national registries. SES is based on occupational status and categorizes gainfully employed subjects into manual and non-manual employees, as well as blue and white-collar workers [18]. History of hospitalization for lung disease was obtained from the National Patient Register and was used as a proxy for smoking.
Serum iron was measured via acidification with citric acid in order to dissociate the Fe3+ transferring complex (coefficient of variation <5 %), whereas TIBC (which indicates the maximum amount of iron required to saturate SI transport protein) was assessed by adding Fe3+ to the serum. Both markers were assessed with a DAX 96, Technicon Instruments Corporation, Tarrytown, NY, USA, 1993–1996. The quantitative determination of CRP was done with an established turbidimetric assay (reagents from Orion Diagnostics, Finland) using fully automated multichannel analyzers (an AutoChemist-PRISMA, New Clinicon, Stockholm, Sweden, 1985–1992) and DAX 96, Technicon Instruments Corporation, Tarrytown, NY, USA, 1993–1996 (coefficient of variation: 12 % at CRP level 40 mg/L). It was not possible to study high-sensitive (hs) CRP because at time of blood sampling and analysis (1985–1996), assay methods for plasma proteins had limited sensitivity, so that CRP concentrations <10 mg/L could not be measured precisely (i.e., non-hsCRP). However, the cut-off of 10 mg/L is widely accepted as the upper limit of the health-associated reference range [19–21]. All methods were fully automated with automatic calibration and accredited laboratory facilities [12].
To assess the effect of small changes in SI and TIBC levels, we calculated standardized values of calcium (i.e., dividing by the standard deviation) using its standard deviation (SD) as a unit when performing statistical models. Moreover, levels of SI and TIBC calcium were categorized into quartiles, based on the entire study population.
Statistical analysis
Pearson’s correlation coefficients were calculated to quantify the association between SI, TIBC, and CRP. To evaluate the association between SI, TIBC, and risk of incident cancer, multivariate hazard ratios were calculated for this risk of cancer by both standardized values and quartiles. A test for trend was conducted by using assignment to quartiles as an ordinal scale. All Cox proportional hazards models took into account potential confounding factors including age as a continuous variable, gender, SES, history of lung disease, and continuous CRP. Models for SI were also adjusted for TIBC and vice versa. Additionally, we performed stratified analyses by levels of CRP (<10 and ≥10 mg/L) to identify how inflammation affects the association between iron and cancer risk. A test for interaction was performed by adding the product of standardized serum iron and levels of CRP (<10 and ≥10 mg/L), and the product of standardized serum iron and serum TIBC.
The above-mentioned analyses were then repeated for specific types of cancer: pancreatic, colon, liver, respiratory, kidney, prostate, stomach, and breast. These cancers were chosen based on the current pre-clinical findings for an association between the iron metabolism and carcinogenesis [12]. Risk of breast cancer was analysed for pre- and post-menopausal women separately by using age as a proxy for menopausal status. This stratification was performed as pre-menopausal women are known to have lower iron levels [22]. In the analysis of pre-menopausal women, individuals were followed to age 50 after which they were censored [23]. In the assessment of post-menopausal risk, individuals with a baseline measurement taken before age 50 entered the study at age 50 by means of delayed entry. All analyses were performed with Statistical Analysis Systems (SAS) release 9.3 (SAS Institute, Cary, NC, USA).
Results
A total of 9,269 persons developed cancer during mean follow-up of 10.57 years. Table 1 shows the baseline characteristics of the study population by cancer status. The Pearson’s correlation between SI and TIBC was −0.04 (p < 0.001). The Pearson’s correlation between SI and CRP was −0.06 (p < 0.001) and −0.03 between TIBC and CRP (p < 0.001). Both SI and TIBC were normally distributed in the study population.
Multivariate Cox proportional hazard ratios for incident cancer and SI and TIBC are shown in Table 2. A positive association was found between standardized values of TIBC and cancer risk [HR per SD of TIBC 1.05 (95 % CI 1.03–1.07)], which was also seen when using quartiles (i.e., HR for 2nd, 3rd and 4th quartile versus 1st quartile: 1.01 (95 % CI 0.96–1.08); 1.05 (0.99–1.11); and 1.15 (1.08–1.22), respectively, p value for trend <0.0001). No statistically significant association was found between SI and cancer risk. Similar findings were found after stratification by CRP levels, although the link between TIBC and cancer risk became weaker among those with CRP ≥10 mg/L. We observed no statistically significant interaction between SI and TIBC and between SI and CRP levels (p interaction 0.08 and 0.42, respectively) (Table 2).
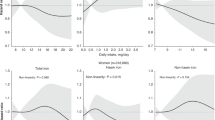
Finally, we performed the above analyses for specific types of cancer (Table 3). The above pattern was also observed for colon cancer (i.e., HR per SD of TIBC 1.17 (95 % CI 1.08–1.28)) as well as pancreatic, respiratory, liver, kidney, prostate, stomach, and premenopausal breast cancer—although most findings were not statistically significant. Interestingly, a positive relation between SI and cancer risk was observed postmenopausal breast cancer (HR per SD of TIBC 1.09 (95 % CI 1.02–1.15)), and similar trend for SI quartiles was also observed. An interaction effect between SI and TIBC was observed for respiratory cancer (p interaction 0.003) (Table 3). Meanwhile, no statistically significant interaction between SI and levels of CRP was observed, but a borderline interaction in stomach cancer (p interaction: 0.05).
Discussion
Overall, we found an inverse association between TIBC and cancer risk particularly in colon cancer. No statistically significant association between SI and cancer risk was observed except for postmenopausal breast cancer, where a positive association was observed. Stratification based on CRP levels showed no markedly different results.
For many years, it has been suggested that iron overload plays a role in carcinogenesis [2]. This was originally described in experimental systems where the injection of iron dextran led to the development of soft tissue sarcoma [2]. More recently, it has been demonstrated that excess iron can promote protein and genomic alterations mirrored in human cancers [2] and this may occur via iron-induced persistent oxidative stress [2]. Also in epidemiological studies, the role of iron in risk of cancer has emerged; Ellervik and colleagues showed a statistically significant positive association between transferrin saturation, a marker of iron overload, and risk of all cancers [2]. Moreover, when studying the iron metabolism in relation to cancer, it is important to take markers of inflammation into account. During inflammation, normal iron homeostatic mechanisms are disturbed leading to the redistribution of iron, resulting in the accumulation of iron in liver, spleen, and at sites of inflammation while concomitantly reducing the iron present in the bone marrow, leading to anaemia of chronic disease (ACD). This process is initiated by hepcidin, an antimicrobial peptide that mediates the internalization and destruction of the iron exporter Ferroportin-1 and which is under the control of pro-inflammatory cytokines [2]. Therefore, under conditions of inflammation, iron availability for proliferating cells is increased and may contribute to the pathogenesis of cancer.
Our study however suggests that apart from postmenopausal breast cancer, there is no association with total SI and cancer and in fact suggests the opposite as there is a positive association with TIBC and cancer. However, this association was influenced by the inflammatory state of the patient, as increased CRP levels weakened the association. This may reflect ACD where hepcidin production in response to inflammatory cytokines will result in low TIBC. Nevertheless, it is of note that the small number of cases in some types of cancer resulted in limited power of our analyses.
The major strength of this analysis lies in the large number of subjects with prospective measurements of SI, TIBC, and CRP in AMORIS, all measured at the same clinical laboratory. To our knowledge, this is the only prospective study on cancer risk with information on SI, TIBC, as well as information on inflammation. This database provided complete follow-up for each person as well as linkage to other registers allowing for detailed information on cancer diagnosis, time of death, and emigration. The AMORIS population was selected by analysing blood samples from health check-ups in non-hospitalized individuals. The AMORIS cohort is similar to the general working population of Stockholm County in terms of SES and ethnicity. During the study period, all-cause mortality was about 14 % lower in the AMORIS population than in the general population of Stockholm County when taking age, gender, and calendar year into account [24]. This selection of a healthy cohort does however not affect the internal validity of our study. A restriction of this study is that there was no information available on tumour grade, stage, or histology, making it impossible to assess the association between iron metabolism and tumour severity, nor did we have information on other important serum iron markers such as ferritin which is widely accepted as a more definitive marker, especially of ACD [25] or potential confounders such as smoking status and body mass index. However, even though we used history of lung disease as a proxy for smoking, some confounding effects may remain. As already mentioned, we only had information on non-hsCRP. The effect of using hsCRP instead of non-hsCRP in the context of inflammation and cancer risk has not been investigated in detail yet, but it is likely that low-grade inflammation is not captured by using this cut-off resulting in an underestimation of the association between CRP and cancer. However, the cut-off value of 10 mg/L is thought to be satisfactory for the purpose of medical events such as ischemic necrosis [19–21]. Nevertheless, we did not have any additional information on acute infection.
Conclusions
This large population-based epidemiological study adds to the existing pre-clinical studies on serum iron and development of specific cancer types. As opposed to previous studies, we found an inverse relation between iron metabolism and risk of cancer, as clearly shown for colon cancer. The positive link found with post-menopausal breast cancer emphasizes the need to address the specific tumour types and clinical features when assessing iron metabolism in the context of cancer. Although no statistically significant interaction between inflammatory markers and iron metabolism was observed, the borderline interaction in relation to stomach cancer indicates a potential role of inflammation in specific cancer development.
References
Mascitelli L, Goldstein MR (2011) Metabolic syndrome and liver cancer: is excess iron the link? Hepatology 54(4):1487
Weinberg ED (1996) The role of iron in cancer. Eur J Cancer Prev 5(1):19–36
Kabat GC, Miller AB, Jain M, Rohan TE (2007) A cohort study of dietary iron and heme iron intake and risk of colorectal cancer in women. Br J Cancer [Research Support, Non-US Gov’t] 97(1):118–122
Kabat GC, Miller AB, Jain M, Rohan TE (2007) Dietary iron and heme iron intake and risk of breast cancer: a prospective cohort study. Cancer Epidemiol Biomarkers Prev [Clinical Trial Randomized Controlled Trial Research Support, Non-U.S. Gov’t] 16(6):1306–1308
Cross AJ, Sinha R, Wood RJ, Xue X, Huang WY, Yeager M et al (2011) Iron homeostasis and distal colorectal adenoma risk in the prostate, lung, colorectal, and ovarian cancer screening trial. Cancer Prev Res (Phila) 4(9):1465–1475
Wu T, Sempos CT, Freudenheim JL, Muti P, Smit E (2004) Serum iron, copper and zinc concentrations and risk of cancer mortality in US adults. Ann Epidemiol 14(3):195–201
Li F, Kishida T, Kobayashi M (1999) Serum iron and ferritin levels in patients with colorectal cancer in relation to the size, site, and disease stage of cancer. J Gastroenterol 34(2):195–199
Kooistra MP, Niemantsverdriet EC, van Es A, Mol-Beermann NM, Struyvenberg A, Marx JJ (1998) Iron absorption in erythropoietin-treated haemodialysis patients: effects of iron availability, inflammation and aluminium. Nephrol Dial Transpl 13(1):82–88
Van Hemelrijck M, Holmberg L, Garmo H, Hammar N, Walldius G, Binda E et al (2011) Association between levels of C-reactive protein and leukocytes and cancer: three repeated measurements in the Swedish AMORIS study. Cancer Epidemiol Biomarkers Prev 20(3):428–437
Rajamaki A, Irjala K, Aitio A (1979) Immunochemical determination of serum transferrin. Reference values, correlation with serum total iron-binding capacity and value in the diagnosis of iron deficiency anaemia and anaemia of chronic disorders. Scandinavian J Haematol 23(3):227–231
Walldius G, Jungner I, Holme I, Aastveit AH, Kolar W, Steiner E (2001) High apolipoprotein B, low apolipoprotein A-I, and improvement in the prediction of fatal myocardial infarction (AMORIS study): a prospective study. Lancet 358(9298):2026–2033
Jungner I, Marcovina SM, Walldius G, Holme I, Kolar W, Steiner E (1998) Apolipoprotein B and A-I values in 147576 Swedish males and females, standardized according to the world health organization-international federation of clinical chemistry first international reference materials. Clin Chem 44(8 Pt 1):1641–1649
Holme I, Aastveit AH, Jungner I, Walldius G (2008) Relationships between lipoprotein components and risk of myocardial infarction: age, gender and short versus longer follow-up periods in the apolipoprotein mortality risk study (AMORIS). J Intern Med 264(1):30–38
Holme I, Aastveit AH, Hammar N, Jungner I, Walldius G (2009) Relationships between lipoprotein components and risk of ischaemic and haemorrhagic stroke in the apolipoprotein mortality risk study (AMORIS). J Intern Med 265(2):275–287
Walldius G, Jungner I, Kolar W, Holme I, Steiner E (1992) High cholesterol and triglyceride values in Swedish males and females: increased risk of fatal myocardial infarction. First report from the AMORIS (Apolipoprotein related mortality risk) study. Blood Press Suppl 4:35–42
Van Hemelrijck M, Garmo H, Binda E, Hayday A, Karagiannis SN, Hammar N et al (2010) Immunoglobulin E and cancer: a meta-analysis and a large Swedish cohort study. Cancer Causes Control 21:1657–1667
Van Hemelrijck M, Garmo H, Holmberg L, Walldius G, Jungner I, Hammar N, Lambe M (2011) Prostate cancer risk in the Swedish AMORIS study: the interplay among triglycerides, total cholesterol, and glucose. Cancer 117(10):2086–2095
Central Bureau for Statistics. Statistics Sweden. Stockholm SAfhwss
Wilkins J, Gallimore JR, Moore EG, Pepys MB (1998) Rapid automated high sensitivity enzyme immunoassay of C-reactive protein. Clin Chem 44(6 Pt 1):1358–1361
Forrest LM, McMillan DC, McArdle CS, Angerson WJ, Dagg K, Scott HR (2005) A prospective longitudinal study of performance status, an inflammation-based score (GPS) and survival in patients with inoperable non-small-cell lung cancer. Br J Cancer 92(10):1834–1836
Proctor MJ, Talwar D, Balmar SM, O’Reilly DS, Foulis AK, Horgan PG et al (2010) The relationship between the presence and site of cancer, an inflammation-based prognostic score and biochemical parameters. Initial results of the Glasgow inflammation outcome study. Br J Cancer 103(6):870–876
Bengtsson C, Lindquist O, Redvall L (1981) Menstrual status and menopausal age of middle-aged Swedish women. A population study of women in Goteborg 1968–1969 and 1974–1975. Acta Obstet Gynecol Scand 60(3):269–275
Lambe M, Wigertz A, Garmo H, Walldius G, Jungner I, Hammar N (2011) Impaired glucose metabolism and diabetes and the risk of breast, endometrial, and ovarian cancer. Cancer Causes Control 22(8):1163–1171
Holzmann M, Jungner I, Walldius G, Ivert I, Nordqvist T, Östergren J (2008) Apolipoproteins B and A-I, standard lipid measures and incidence of myocardial infarction in men and women, with or without chronic kidney disease. Study IV in thesis for doctorial degree (Ph.D.). In: Holzmann M (ed) Renal insufficiency, mortality and myocardial infarction, Stockholm, Karolinska Institutet
Vanarsa K, Ye Y, Han J, Xie C, Mohan C, Wu T (2012) Inflammation associated anemia and ferritin as disease markers in SLE. Arthritis Res Ther 14(4):R182
Conflict of interest
There are no financial disclosures.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
About this article
Cite this article
Gaur, A., Collins, H., Wulaningsih, W. et al. Iron metabolism and risk of cancer in the Swedish AMORIS study. Cancer Causes Control 24, 1393–1402 (2013). https://doi.org/10.1007/s10552-013-0219-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10552-013-0219-8