
Abstract
Purpose
The colon coordinates fecal elimination while reabsorbing excess fluid. Extended colonic resection removes synchronous and prevents metachronous disease but may adversely alter bowel function and health-related quality of life to a greater degree than segmental resection. This study examined the short-term morbidity and long-term function and quality of life after colon resections of different extents.
Methods
Patients undergoing extended resections (n = 201, subtotal colectomy with ileosigmoid or total abdominal colectomy with ileorectal anastomosis) and segmental colonic resections (n = 321) during 1991 to 2003 were reviewed for perioperative outcomes and surveyed for bowel function and quality of life using an institutional questionnaire and a validated quality of life instrument (response rate: 70 percent).
Results
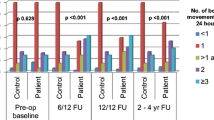
The most common indication for extended resections was multiple polyps, and for segmental resections, single malignancy. The complication-free rate was 75.4 percent after segmental resections, 42.8 percent after ileosigmoid anastomosis, and 60 percent after ileorectal anastomosis. Median daily stool frequency was two after segmental resections, four after ileosigmoid anastomosis, and five after ileorectal anastomosis, despite considerable dietary restrictions (55.6 percent) and medication use (19.6 percent daily) after ileorectal anastomosis. Significant proportions of patients felt restricted from preoperative social activity (31.5 percent), housework (20.4 percent), recreation (31.5 percent), and travel (42.6 percent) after ileorectal anastomosis. The overall quality of life after segmental resection, ileosigmoid anastomosis, and ileorectal anastomosis was 98.5, 94.9, and 91.2, respectively.
Conclusions
Measurable compromises in long-term bowel function and quality of life were observed after extended vs. segmental resections. The relative differences in patient-related outcomes should be deliberated against the clinical benefits of extended resection for the individual patient.
Similar content being viewed by others


References
Wright HK. The functional consequences of colectomy. Am J Surg 1975;130:532–4.
Ottinger LW. Frequency of bowel movements after colectomy with ileorectal anastomosis. Arch Surg 1978;113:1048–9.
Aylett SO. Three hundred cases of diffuse ulcerative colitis treated by total colectomy and ileorectal anastomosis. BMJ 1966;1909:1001–5.
Dozois EJ, Dozois RR. Familial adenomatous polyposis. In: Kelly KA, Sarr MG, Hindler RA. Mayo Clinic gastrointestinal surgery. Philadelphia: Saunders, 2004:559–67.
Setti-Carraro P, Nicholls RJ. Choice of prophylactic surgery for the large bowel component of familial adenomatous polyposis. Br J Surg 1996;83:885–92.
Church JM. Prophylactic colectomy in patients with hereditary nonpolyposis colorectal cancer. Ann Med 1996;28:479–82.
Brief DK, Brener BJ, Goldenkranz R, Alpert J, Yalof I, Parsonnet V. An argument for increased use of subtotal colectomy in the management of carcinoma of the colon. Am Surg 1983;49:66–72.
Demeter JG, Freeark RJ. The role of prophylactic subtotal colectomy in metachronous carcinoma of the colon and rectum. Surg Gynecol Obstet 1992;175:1–7.
Boardman LA. Heritable colorectal cancer syndromes: recognition and preventive management. Gastroenterol Clin North Am 2002;31:1107–31.
The SCOTIA group. Single-stage treatment for malignant left-sided colonic obstruction: a prospective randomized clinical trial comparing subtotal colectomy with segmental resection following intraoperative irrigation. Br J Surg 1995;82:1622–7.
Reemst PH, Kuijpers HC, Wobbes T. Management of left-sided colonic obstruction by subtotal colectomy and ileocolic anastomosis. Eur J Surg 1998;164:537–42.
Easson AM, Cotterchio M, Crosby JA, et al. A population-based study of the extent of surgical resection of potentially curable colon cancer. Ann Surg Oncol 2002;9:380–7.
Oakley JR, Jagelman DG, Fazio VW, et al. Complications and quality of life after ileorectal anastomosis for ulcerative colitis. Am J Surg 1985;149:23–30.
Pastore RL, Wolff BG, Hodge D. Total abdominal colectomy and ileorectal anastomosis for inflammatory bowel disease. Dis Colon Rectum 1997;40:1455–64.
Knowles CH, Scott M, Lunniss PJ. Outcome of colectomy for slow transit constipation. Ann Surg 1999;230:627–38.
Church JM, Fazio VW, Lavery IC, Oakley JR, Milsom J, McGannon E. Quality of life after prophylactic colectomy and ileorectal anastomosis in patients with familial adenomatous polyposis. Dis Colon Rectum 1996;39:1404–8.
Hassan I, Chua HK, Wolff BG, et al. Quality of life after ileo-pouch anal anastomosis and ileorectal anastomosis in patients with familial adenomatous polyposis. Dis Colon Rectum 2005;48:2032–7.
Walsh RM, Aranha GV, Freeark RJ. Mortality and quality of life after total abdominal colectomy. Arch Surg 1990;125:1564–6.
Elton C, Makin G, Hitos K, Cohen CR. Mortality, morbidity and functional outcome after ileorectal anastomosis. Br J Surg 2003;90:59–65.
Clavien PA, Sanabria JR, Strasberg SM. Proposed classification of complications of surgery with examples of utility in cholecystectomy. Surgery 1992;111:518–26.
Pemberton JH, Phillips SF, Ready RR, Zinsmeister AR, Beahrs OH. Quality of life after Brooke ileostomy and ileal pouch-anal anastomosis. Comparison of performance status. Ann Surg 1989;209:620–8.
Drossman DA, Patrick DL, Whitehead WE, et al. Further validation of the IBS-QOL: a disease-specific quality-of-life questionnaire. Am J Gastroenterol 2000;95:999–1007.
Patrick DL, Drossman DA, Frederick IO, DiCesare J, Puder KL. Quality of life in persons with irritable bowel syndrome: development and validation of a new measure. Dig Dis Sci 1998;43:400–11.
Suzman MS, Talmor M, Jennis R, Binkert B, Barie PS. Accurate localization and surgical management of active lower gastrointestinal hemorrhage with technetium-labeled erythrocyte scintigraphy. Ann Surg 1996;224:29–36.
Van Dalen R, Church J, McGannon E, Fay S, Burke C, Clark B. Patterns of surgery in patients belonging to amsterdam-positive families. Dis Colon Rectum 2003;46:617–20.
bin Mohd Zam NA, Tan KY, Ng C, et al. Mortality, morbidity and functional outcome after total or subtotal abdominal colectomy in the Asian population. ANZ J Surg 2005;75:840–3.
Eu KW, Lim SL, Seow-Choen F, Leong AF, Ho YH. Clinical outcome and bowel function following total abdominal colectomy and ileorectal anastomosis in the Oriental population. Dis Colon Rectum 1998;41:215–8.
Aranha GV, Walsh RM, Jacobs HK, et al. Factors influencing bowel function following total abdominal colectomy. Dis Colon Rectum 1996;39:1418–22.
Nakamura T, Pikarsky AJ, Potenti FM, et al. Are complications of subtotal colectomy with ileorectal anastomosis related to the original disease. Am Surg 2001;67:417–20.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
You, Y.N., Chua, H.K., Nelson, H. et al. Segmental vs. Extended Colectomy: Measurable Differences in Morbidity, Function, and Quality of Life. Dis Colon Rectum 51, 1036–1043 (2008). https://doi.org/10.1007/s10350-008-9325-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10350-008-9325-1