
Abstract
Purpose
The risk of rectal cancer after colectomy and ileorectal anastomosis may be reduced in the last decades, as patients with severe polyposis now have an ileoanal pouch. We have reevaluated the risk of rectal cancer and proctectomy for all causes according to the year of operation.
Methods
On the basis of the year of operation in 776 patients with ileorectal anastomosis and 471 pouch patients in Denmark, Finland, Holland, and Sweden, the “pouch period” was defined to start in 1990. Ileorectal anastomosis follow-up data was captured by May 31, 2006. The cumulative risk of rectal cancer and proctectomy was compared before and after 1990 by Kaplan-Meier analysis.
Results
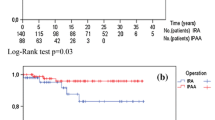
In the prepouch period 56/576 patients (10 percent) developed rectal cancer, vs. 4/200 (2 percent) in the pouch period. Neither the cumulative risk of rectal cancer (p = 0.07) nor the cumulative risk of proctectomy (p = 0.17) changed. However, in females the cumulative risk of rectal cancer (p = 0.04) and of proctectomy (p = 0.03) were lower in the pouch period.
Conclusions
Since the introduction of the ileoanal pouch rectal cancer has decreased after ileorectal anastomosis, but only statistically significant in females. This indicates that ileorectal anastomosis may still be justified in selected patients with mild adenomatosis, especially in young females.




Similar content being viewed by others


References
Kartheuser A, Stangherlin P, Brandt D, Remue C, Sempoux C. Restorative proctocolectomy and ileal pouch-anal anastomosis for familial adenomatous polyposis revisited. Fam Cancer 2006;241–60.
Hassan I, Chua HK, Wolff BG, et al. Quality of life after ileal pouch-anal anastomosis and ileorectal anastomosis in patients with familial adenomatous polyposis. Dis Colon Rectum 2005;48:2032–7.
Parc Y, Piquard A, Dozois RR, Parc R, Tiret E. Long-term outcome of familial adenomatous polyposis patients after restorative coloproctectomy. Ann Surg 2004;239:378–82.
Nieuwenhuis MH, Mathus-Vliegen LM, Slors FJ, et al. Genotype-phenotype correlations as a guide in the management of familial adenomatous polyposis. Clin Gastroenterol Hepatol 2007;5:374–8.
Valanzano R, Ficari F, Curia MC, et al. Balance between endoscopic and genetic information in the choice of ileorectal anastomosis for familial adenomatous polyposis. J Surg Oncol 2007;95:28–33.
Bülow C, Vasen H, Järvinen H, Björk J, Bisgaard ML, Bülow S. Ileorectal anastomosis is appropriate for a subset of patients with familial adenomatous polyposis. Gastroenterology 2000;119:1454–60.
Björk J, Akerbrant H, Iselius L, et al. Outcome of primary and secondary ileal pouch-anal anastomosis and ileorectal anastomosis in patients with familial adenomatous polyposis. Dis Colon Rectum 2001;44:984–92.
Soravia C, Klein L, Berk T, O’Connor BI, Cohen Z, McLeod RS. Comparison of ileal pouch-anal anastomosis and ileorectal anastomosis in patients with familial adenomatous polyposis. Dis Colon Rectum 1999;42:1028–33.
Church J. In which patients do I perform IRA, and why? Familial Cancer 2006;5:237–40.
Günther K, Braunrieder G, Bittorf BR, Hohenberger W, Matzel KE. Patients with familial adenomatous polyposis experience better bowel function and quality of life after ileorectal anastomosis than after ileoanal pouch. Colorectal Dis 2003;5:38–44.
Church J, Burke C, McGannon E, Pastean O, Clark B. Risk of rectal cancer in patients after colectomy and ileorectal anastomosis for familial adenomatous polyposis: a function of available surgical options. Dis Colon Rectum 2003;46:1175–81.
Bussey HJ, Eyers AA, Ritchie SM, Thomson JP. The rectum in adenomatous polyposis: the St. Mark’s policy. Br J Surg 1985;72 Suppl s29–31.
Bertario L, Russo A, Radice P, et al. Genotype and phenotype factors as determinants for rectal stump cancer in patients with familial adenomatous polyposis. Hereditary colorectal tumors registry. Ann Surg 2000;231:538–43.
DeCosse JJ, Bülow S, Neale K, et al. Rectal cancer risk in patients treated for familial adenomatous polyposis. Br J Surg 1993;79:1372–5.
Heiskanen I, Järvinen HJ. Fate of the rectal stump after colectomy and ileorectal anastomosis for familial adenomatous polyposis. Int J Colorectal Dis 1997;12:9–13.
Iwama T, Mishima Y. Factors influencing rectum-preserving surgery in patients with familial adenomatous polyposis. Dis Colon Rectum 1994;37:1024–6.
Björk J, Akerbrant HI, Iselius LE, Hultcrantz RW. Risk factors for rectal cancer morbidity and mortality in patients with familial adenomatous polyposis after colectomy and ileorectal anastomosis. Dis Colon Rectum 2000;43:1719–25.
Nugent KP, Phillips RS. Rectal cancer risk in older patients with familial adenomatous polyposis and an ileorectal anastomosis: a cause for concern. Br J Surg 1992;79:1204–6.
Utsunomiya J, Iwama T, Imajo M, et al. Total colectomy, mucosal proctectomy, and ileoanal anastomosis. Dis Colon Rectum 1980;23:459–66.
Parks AG, Nicholls RJ, Belliveau P. Proctocolectomy with ileal reservoir and anal anastomosis. Br J Surg 1980;67:533–8.
Aziz O, Athanasiou T, Fazio VW, et al. Meta-analysis of observational studies of ileorectal versus ileal pouch-anal anastomosis for familial adenomatous polyposis. Br J Surg 2006:407–17.
Debinski HS, Love S, Spigelman AD, Phillips RK. Colorectal polyp counts and cancer risk in familial adenomatous polyposis. Gastroenterology 1996;110:1028–30.
Vasen HF, van der Luijt RB, Slors JF, et al. Molecular tests as a guide to surgical management of familial adenomatous polyposis. Lancet 1996;348:433–5.
Tonelli F, Valanzano R, Monaci I, Mazzoni P, Anastasi A, Ficari F. Restorative proctocolectomy or rectum-preserving surgery in patients with familial adenomatous polyposis: results of a prospective study. World J Surg 1997;21:653–9.
van Duijvendijk P, Slors JF, Taat CW, Oosterveld P, Vasen HF. Functional outcome after colectomy and ileorectal anastomosis compared with proctocolectomy and ileal pouch-anal anastomosis in familial adenomatous polyposis. Ann Surg 1999;230:648–54.
Ambroze WL Jr, Dozois RR, Pemberton JH, Beart RW Jr, Ilstrup DM. Familial adenomatous polyposis: results following ileal pouch-anal anastomosis and ileorectostomy. Dis Colon Rectum 1992;35:12–5.
Van Duijvendijk P, Slors JF, Taat CW, et al. Quality of life after total colectomy with ileorectal anastomosis or proctocolectomy and ileal pouch-anal anastomosis for familial adenomatous polyposis. Br J Surg 2000;87:590–6.
Ko CY, Rusin LC, Schoetz DJ Jr, et al. Does better functional result equate with better quality of life? Implications for surgical treatment in familial adenomatous polyposis. Dis Colon Rectum 2000;43:829–37.
Vasen HF, van Duijvendijk P, Buskens E, et al. Decision analysis in the surgical treatment of patients with familial adenomatous polyposis: a Dutch-Scandinavian collaborative study including 659 patients. Gut 2001;49:231–5.
Olsen KO, Juul S, Bülow S, et al. Female fecundity before and after operation for familial adenomatous polyposis. Br J Surg 2003;90:227–31.
Tekkis PP, Heriot AG, Gallagher M, et al. Predicting the risk of proctectomy after total colectomy and ileorectal anastomosis for familial adenomatous polyposis (FAP): a multifactorial model [abstract]. Colorectal Dis 2005;7(Suppl 1)26.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Bülow, S., Bülow, C., Vasen, H. et al. Colectomy and Ileorectal Anastomosis is still an Option for Selected Patients with Familial Adenomatous Polyposis. Dis Colon Rectum 51, 1318–1323 (2008). https://doi.org/10.1007/s10350-008-9307-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10350-008-9307-3