
Abstract
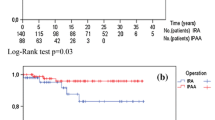
PURPOSE: The aim of this study was to evaluate the surgical complications and long-term outcome and assess the functional results and quality of life after ileorectal anastomosis and ileal pouch-anal anastomosis in patients with familial adenomatous polyposis. METHODS: From 1980 to 1997, 131 patients with familial adenomatous polyposis were operated on or were followed up or both at the Familial Gastrointestinal Cancer Registry at Mount Sinai Hospital. Demographic and operative data were prospectively collected in the ileal pouch-anal anastomosis group, and retrospectively in the ileorectal anastomosis group. A questionnaire or telephone interview or both were undertaken to evaluate functional outcome and quality of life. RESULTS: The ileorectal anastomosis group consisted of 60 patients (mean age, 31 years; mean follow-up, 7.7 years). In the ileal pouch-anal anastomosis group there were 50 patients (mean age, 35 years; mean follow-up, 6 years). There were no statistically significant differences with respect to anastomotic leak rate in ileal pouch-anal anastomosisvs. ileorectal anastomosis (12vs. 3 percent;P=0.21), risk of small-bowel obstruction (24vs. 15 percent;P=0.58), and risk of intra-abdominal sepsis (3vs. 2 percent;P=0.86). Reoperation rate was similar in the two groups (14vs. 16 percent;P=0.94). Twenty-one patients (37 percent) with ileorectal anastomosis were converted to ileal pouch-anal anastomosis (12 patients) or proctocolectomy (9 patients), because of rectal cancer (5 patients), dysplasia (1 patient), or uncontrollable rectal polyps (15 patients). Two pelvic pouches were excised, and another one was defunctioned. Information regarding functional results and quality of life was obtained in 40 patients (66.6 percent) in the ileorectal anastomosis group and in 43 patients (86 percent) in the ileal pouch-anal anastomosis group. Patients with ileorectal anastomosis had a significantly better functional outcome with regard to nighttime continence and perineal skin irritation. But otherwise, functional results and quality of life were similar. CONCLUSIONS: Although ileorectal anastomosis has a better functional outcome, ileal pouch-anal anastomosis may be preferable because of the lower long-term failure rate. Ileorectal anastomosis is still an option in patients with familial adenomatous polyposis with rectal polyp sparing and good compliance for follow-up.
Similar content being viewed by others

References
Groden J, Thliveris A, Samowitz W,et al. Identification and characterization of the familial adenomatous polyposis coli gene. Cell 1991;66:589–600.
Kinzler K, Nilbert M, Su L,et al. Identification of FAP locus genes from chromosome 5q21. Science 1991;253:661–5.
Bussey H. Familial polyposis coli. Families studies, histopathology, differential diagnosis, and results of treatment. Baltimore: The Johns Hopkins University Press, 1975.
Lockhart-Mummery JP. Case of complete resection of the large bowel for multiple adenomata. Proc R Soc Med 1919;12:3–45.
Jagelman DG. Choice of operation in familial adenomatous polyposis. World J Surg 1991;15:47–9.
Dozois RR, Berk T, Bülow S,et al. Surgical aspects of familial adenomatous polyposis. Int J Colorectal Dis 1988;3:1–16.
Madden MV, Neale KF, Nicholls RJ,et al. Comparison of morbidity and function after colectomy with ileorectal anastomosis or restorative proctocolectomy for familial adenomatous polyposis. Br J Surg 1991;78:789–92.
Nugent KP, Phillips RK. Rectal cancer risk in older patients with familial adenomatous polyposis and an ileorectal anastomosis: a cause for concern. Br J Surg 1992;79:1204–6.
Heiskanen I, Järvinen HJ. Fate of the rectal stump after colectomy and ileorectal anastomosis for familial adenomatous polyposis. Int J Colorectal Dis 1997;12:9–13.
De Cosse J, Bülow S, Neale K,et al. Rectal cancer risk in patients treated for familial adenomatous polyposis. The Leeds Castle Polyposis Group. Br J Surg 1992;79:1372–5.
Parks AG, Nicholls RJ, Belliveau P. Proctocolectomy with ileal reservoir and anal anastomosis. Br J Surg 1980;67:533–8.
Soravia C, Kartheuser A, Ayala T,et al. L'anastomose iléo-anale dans la rectocolite ulcéro-hémorragique et la polypose adénomateuse familiale: faut-il faire une mucosectomie endo-anale de principe? Gastroenterol Clin Biol 1994; 18:469–74.
Kartheuser A, Parc R, Penna C,et al. Ileal pouch-anal anastomosis as the first choice operation in patients with familial adenomatous polyposis: a ten-year experience. Surgery 1996;119:615–23.
Nyam DC, Brillant PT, Dozois RR, Kelly KA, Pemberton JH, Wolff BG. Ileal pouch-anal canal anastomosis for familial adenomatous polyposis. Ann Surg 1997;226:514–21.
Cohen Z, McLeod RS, Stephen W, Stern HS, O'Connor BI, Reznick R. Continuing evolution of the pelvic pouch procedure. Ann Surg 1992;216:506–11.
Fazio VW, Ziv Y, Church JM,et al. Ileal pouch-anal anastomoses complications and function in 1005 patients. Ann Surg 1995;222:120–7.
Berk T, Cohen Z, Cullen JB. Familial polyposis and the role of the preventive registry. Can Med Assoc J 1981;124:1427–8.
Soravia C, O'Connor B, Berk T, McLeod RS, Cohen Z. Functional outcome of conversion of ileorectal anastomosis to ileal pouch-anal anastomosis in patients with familial adenomatous polyposis and ulcerative colitis. Dis Colon Rectum 1999;42:000–000.
McLeod R, Churchill D, Lock A, Vanderburgh S. Cohen Z. Quality of life of patients with ulcerative colitis preoperatively and postoperatively. Gastroenterology 1991;101:1307–13.
Soravia C, Bapat B, Cohen Z. Familial adenomatous polyposis (FAP) and Hereditary nonpolyposis colorectal cancer (HNPCC): a review of clinical, genetic and therapeutic aspects. Schweiz Med Wschr 1997;127:682–90.
Ambroze WL, Dozois RR, Pemberton JH, Beart RW Jr, Ilstrup DM. Familial adenomatous polyposis: results following ileal pouch-anal anastomosis and ileorectostomy. Dis Colon Rectum 1992;35:12–5.
MacRae HM, McLeod RS, Cohen Z, O'Connor BI, Ton EN. Risk factors for pelvic pouch failure. Dis Colon Rectum 1997;40:257–62.
von Herbay A, Stern J, Herfarth C. Pouch-anal cancer after restorative proctocolectomy for familial adenomatous polyposis. Am J Surg Pathol 1996;20:995–9.
Bassuini MM, Billings PJ. Carcinoma in an ileoanal pouch after restorative proctocolectomy for familial adenomatous polyposis. Br J Surg 1996;83:506.
Hoehner JC, Metcalf AM. Development of invasive adenocarcinoma following colectomy with ileoanal anastomosis for familial polyposis coli. Dis Colon Rectum 1994;37:824–8.
Tytgat GNJ. Surveillance of familial adenomatous polyposis patients after ileorectal anastomosis or ileoanal pouch anastomosis. Gastrointest Endosc Clin North Am 1997;7:111–27.
Nugent KP, Spigelman AD, Nicholls RJ, Talbot IC, Neale K, Phillips RK. Pouch adenomas in patients with familial adenomatous polyposis. Br J Surg 1993;80:1618–9.
Church JM, Oakley JR, Wu JS. Pouch polyposis after ileal pouch-anal anastomosis for familial adenomatous polyposis. Dis Colon Rectum 1996;39:584–6.
Penna C, Tiret E, Parc R,et al. Operation and abdominal desmoid tumors in familial adenomatous polyposis. Surg Gynecol Obstet 1993;177:263–8.
Soravia C, Berk T, Madlensky L,et al. Genotype-phenotype correlations in attenuated adenomatous polyposis coli. Am J Hum Genet 1998;62:1290–301.
Vasen HF, van der Luijt RB, Slors JF,et al. Molecular genetic tests as a guide to surgical management of familial adenomatous polyposis. Lancet 1996;348:433–5.
Wu JS, Paul P, McGannon EA, Church JM. APC genotype, polyp number, and surgical options in familial adenomatous polyposis. Ann Surg 1998;227:57–62.
Evans DG, Evans D, Hill J, Dudding T, Burn J, Maher ER. Molecular genetic tests in surgical management of familial adenomatous polyposis[letter]. Lancet 1997;350:1777.
Author information
Authors and Affiliations
Additional information
Read at the meeting of The American Society of Colon and Rectal Surgeons, San Antonio, Texas, May 2 to 7, 1998.
About this article
Cite this article
Soravia, C., Klein, L., Berk, T. et al. Comparison of ileal pouch-anal anastomosis and ileorectal anastomosis in patients with familial adenomatous polyposis. Dis Colon Rectum 42, 1028–1033 (1999). https://doi.org/10.1007/BF02236696
Issue Date:
DOI: https://doi.org/10.1007/BF02236696