
Abstract
Background
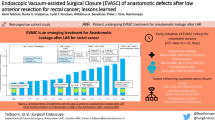
Anastomotic insufficiency in patients with colorectal anastomosis is a major complication with high morbidity and mortality. Local treatment with transrectal lavage and drainage can be considered in patient without peritonitis. In order to prevent prolonged wound closure and secondary complications during conservative treatment we investigated the vacuum assisted closure (VAC) in this setting.
Methods
Ten patients with anastomotic insufficiency after colorectal resections, who did not require transabdominal interventions, were treated with an Endo-vacuum assisted closure dressing (Group A; n = 5) or by transrectal lavage (Group B; n = 5). Time for wound healing, duration of hospitalization and pain assessment were compared in both groups.
Results
The Endo-vacuum assisted closure treatment was performed for a median time of 27 days without any vacuum assisted closure associated complications. Wound healing was significantly accelerated in Group A compared to Group B. Time in hospital was slightly shortened in patients with Endo-vacuum assisted closure. Pain assessment in both groups did not show any significant differences.
Conclusion
Endo-vacuum assisted closure therapy is a novel approach that can be considered in diverted patients with failed colorectal anastomoses. Larger randomized trials that include complete cost-benefit analyses are needed to establish its role in this setting.





Similar content being viewed by others


References
Nesbakken A, Nygaard K, Lunde OC, Blucher J, Gjertsen O, Dullerud R. Anastomotic leak following mesorectal excision for rectal cancer: true incidence and diagnostic challenges. Colorectal Dis 2005;7:576–81.
Averbach AM, Chang D, Koslowe P, Sugarbaker PH. Anastomotic leak after double-stapled low colorectal resection. Dis Colon Rectum 1996;39:780–7.
Rullier E, Laurent C, Garrelon JL, Michel P, Saric J, Parneix M. Risk factors for anastomotic leakage after resection of rectal cancer. Br J Surg 1998;85:355–8.
Tonus C, Keller O, Kropp R, Nier H. Colorectal cancer. Which factors influence postoperative complications? Langenbecks Arch Chir 1996;381:251–7.
Law WL, Chu KW, Ho J, Chan CW. Risk factors for anastomotic leakage after low anterior resection with total mesorectal excision. Am J Surg 2000;179:92–6.
Peeters KC, Tollenaar RA, Marijnen CA, et al. Risk factors for anastomotic failure after total mesorectal excision of rectal cancer. Br J Surg 2005;92:211–6.
Anderson ID, Fearon KC, Grant IS. Laparotomy for abdominal sepsis in the critically ill. Br J Surg 1996;83:535–9.
Keighley MR, Williams NS, eds. Surgery of the anus, rectum and colon. Philadelphia, Saunders; 1993:1024–6.
Armstrong DG, Lavery LA. Diabetic Foot Study Consortium. Negative pressure wound therapy after partial diabetic foot amputation: a multicentre, randomised controlled trial. Lancet 2005;12:1704–10.
Labler L, Trentz O. The use of vacuum assisted closure (VAC (®)) in soft tissue injuries after high energy pelvic trauma. Langenbecks Arch Surg 2007;392:601–9.
Fleck TM, Fleck M, Moidl R, et al. The vacuum assisted closure system for the treatment of deep sternal wound infections after cardiac surgery. Ann Thorac Surg 2002;74:1596–1600.
Schaffzin DM, Douglas JM, Stahl TJ, Smith LE. Vacuum-assisted closure of complex perineal wounds. Dis Colon Rectum 2004;47:1745–8.
Weidenhagen R, Grutzner KU, Kopp R, Spelsberg FW, Jauch KW. Role of vacuum therapy in the management of the septic abdomen. Zentralbl Chir 2006;131(Suppl 1):115–9.
Argenta LC, Morykwas MJ. Vacuum-assisted closure: a new method for wound control and treatment: clinical experience. Ann Plast Surg 1997;38:563–76.
Argenta LC, Morykwas MJ, Marks MW, DeFranzo AJ, Molnar JA, David LR. Vacuum-assisted closure: state of clinic art. Plast Reconstr Surg 2006;117:127–42.
Morykwas MJ, Argenta LC, Shelton-Brown EI, McGuirt W. Vacuum-assisted closure: a new method for wound control and treatment: animal studies and basic foundation. Ann Plast Surg 1997;38:553–62.
Weidenhagen R, Spelsberg F, Lang RA, Jauch KW, Gruetzner KU. New method for sepsis control caused by anastomotic leakage in rectal surgery- the endo-VAC. Int J Colorectal Dis 2003;5:1–4.
Nagell CF, Holte K. Treatment of anastomotic leakage after rectal resection with transrectal vacuum-assisted drainage (VAC) A method for rapid control of pelvic sepsis and healing. Int J Colorectal Dis 2006;31:1–4.
Karliczek A, Jesus EC, Matos D, Castro AA, Atallah AN, Wiggers T. Drainage or nondrainage in elective colorectal anastomosis: a systematic review and meta-analysis. Colorectal Dis 2006:8:259–65.
Urbach DR, Kennedy ED, Cohen MM. Colon and rectal anastomoses do not require routine drainage: a systematic review and meta-analysis. Ann Surg 1999;229:174–80.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Mees, S.T., Palmes, D., Mennigen, R. et al. Endo–vacuum Assisted Closure Treatment for Rectal Anastomotic Insufficiency. Dis Colon Rectum 51, 404–410 (2008). https://doi.org/10.1007/s10350-007-9141-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10350-007-9141-z