
Abstract
Background
A model that quantifies the risk of peritoneal recurrence would be a useful tool for improving decision-making in patients undergoing curative-aim gastrectomy for gastric cancer (GC).
Methods
Five Italian centers participated in this study. Two risk scores were created according to the two most widely used pathologic classifications of GC (the Lauren classification and the presence of signet-ring-cell features). The risk scores (the PERI-Gastric 1 and 2) were based on the results of multivariable logistic regressions and presented as nomograms (the PERI-Gram 1 and 2). Discrimination was assessed with the area under the curve (AUC) of receiver operating curves. Calibration graphs were constructed by plotting the actual versus the predicted rate of peritoneal recurrence. Internal validation was performed with a bootstrap resampling method (1000 iterations).
Results
The models were developed based on a population of 645 patients (selected from 1580 patients treated from 1998 to 2018). In the PERI-Gastric 1, significant variables were linitis plastica, stump GC, pT3–4, pN2–3 and the Lauren diffuse histotype, while in the PERI-Gastric 2, significant variables were linitis plastica, stump GC, pT3–4, pN2–3 and the presence of signet-ring cells. The AUC was 0,828 (0.778–0.877) for the PERI-Gastric 1 and 0,805 (0.755–0.855) for the PERI-Gastric 2. After bootstrap resampling, the PERI-Gastric 1 had a mean AUC of 0.775 (0.721–0.830) and a 95%CI estimate for the calibration slope of 0.852–1.505 and the PERI-Gastric 2 a mean AUC of 0.749 (0.693–0.805) and a 95%CI estimate for the slope of 0.777–1.351. The models are available at www.perigastric.org.
Conclusions
We developed the PERI-Gastric and the PERI-Gram as instruments to determine the risk of peritoneal recurrence after curative-aim gastrectomy. These models could direct the administration of prophylactic intraperitoneal treatments.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Gastric cancer (GC) is a disease characterized by a high rate of recurrence, which is reported in 40–61% of patients even after gastrectomy with curative intent [1, 2]. Metachronous peritoneal recurrence occurs in 10–46% of patients, representing 36–45% of all recurrence [3], with a reported median recurrence-free survival of 8.5–14 months [4, 5]. Prognosis after the development of carcinomatosis is dismal, with a median survival of 4–7 months and poor response to palliative chemotherapy [6, 7]. The occurrence of peritoneal relapse is often perceived as unsurprising and somewhat unavoidable, as neither neoadjuvant nor adjuvant systemic chemotherapy is effective in limiting its onset, especially in locally advanced gastric cancer [4, 8,9,10]. For this reason, adjuvant intraperitoneal prophylactic therapies have been investigated, with promising results [11, 12]. However, the high morbidity of these treatments has limited their implementation in clinical practice due to the unclear balance between benefits and overtreatment.
Quantifying the risk of peritoneal recurrence would be useful for improving decision-making in patients undergoing gastrectomy with curative intent and identifying high-risk patients who would probably benefit from prophylactic HIPEC or other intraperitoneal prophylactic treatments. The risk for carcinomatosis is influenced by specific GC subtypes that express different peritoneal tropism, as in diffuse and signet ring cell GC [9, 10, 13], but to date, few studies have developed prognostic models quantifying the actual risk for peritoneal recurrence in patients undergoing gastrectomy with curative intent [14], and even fewer have included indicators of the GC phenotype in these models[8, 15, 16].
The aim of our study was to develop a reliable peritoneal recurrence index to quantify the risk of peritoneal carcinomatosis in patients treated with gastrectomy with curative intent.
Methods
Study design
This was a multicentric retrospective cohort study to develop a prediction model for prognostic purposes. This study is reported in accordance with the Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD) reporting guideline statement checklist for prediction model development and internal validation [17]. The study was approved by the IRB of the Gemelli Hospital (IRB Protocol N. 3694).
Patient selection
The population of this study included all patients with histologically proven gastroesophageal or gastric carcinoma undergoing gastrectomy with scurative intent between January 1998 and December 2018 at the following centers: General Surgery—Fondazione Policlinico Universitario “A. Gemelli” IRCSS (Roma, Italia), Azienda Ospedaliero—Universitaria di Orbassano (Orbassano, Torino, Italia), Surgical Oncology—IRCCS Humanitas Research Hospital (Milano, Italia), Istituto Europeo di Oncologia IRCCS (Milano, Italia) and ASST Settelaghi—Presidio Ospedaliero Gallarate (Varese, Italia). Study patients with pathological stage IB-III undergoing upfront gastrectomy and patients with gastric carcinomas in clinical Stage I–III or cT4bNxM0 undergoing neoadjuvant therapy and subsequent gastrectomy with curative intent were included in this study. Patients undergoing R1–2 resection, patients undergoing less than D1+ lymphadenectomy, patients with metastatic disease (including patients with positive peritoneal cytology), patients who died within 30 postoperative days, patients with incomplete data on pathological staging and patients with follow-up < 18 months were excluded from the study.
Data collection
Data were retrospectively reviewed from prospectively collected datasets. Data collected from medical records included age, sex, location (with particular interest for the involvement of the EGJ) and grade of the tumor, peritoneal cytology results, type of upfront therapy (preoperative chemotherapy or surgery), type of gastrectomy, additional organ resection, type of lymphadenectomy, pathological staging, WHO classification, Lauren classification, presence of signet ring cells, presence of mucin, postoperative morbidity and survival outcomes [disease-free survival (DFS), progression-free survival (PFS) and overall survival (OS)]. Patients were classified according to the 8th edition of the American Joint Committee on Cancer manual [18]. The follow-up was conducted by the surgical teams at each center. Peritoneal recurrence was defined as any radiologic, laparoscopic, laparotomic, or histologic evidence of metachronous peritoneal carcinomatosis as the first recurrence site during follow-up.
Statistical analysis
Clinicopathological characteristics are summarized using frequencies and percentages for categorical variables and means (± standard deviations) or medians (ranges) for continuous variables. The characteristics of patients with or without peritoneal recurrence were compared using Pearson’s chi-squared test or Fisher’s exact test for categorical variables and Student’s t tests for continuous variables. The median follow-up was calculated as the median follow-up of survivors. DFS and OS were calculated from the date of gastrectomy. PFS was calculated from the date of recurrence. To select variables for the prognostic score, a backward multivariable logistic regression was conducted on the whole study population, including all variables that could potentially be associated with peritoneal recurrence. Two models (1 and 2) were developed in parallel, using two widely used pathologic classifications of GC, namely, the Lauren classification and the presence of SRC features, to increase the possibility for a wider application in clinical practice. Indeed, the Lauren classification is not universally applied in all Western centers, whereas a report of the presence of SRCs features in the clinical specimen could be available instead. In this study, the use of SRC features instead of the classical WHO definition of SRC tumors (SRCs > 50%) has been favored, according to the results from several groups demonstrating that the presence of SRC features even < 50% is a significant prognostic value. [9, 19, 20].
The two models can be used separately. According to a rate of the event incidence detected in the series (metachronous peritoneal carcinomatosis) of 9.9% and to a final number of 5 variables selected by multivariable logistic analysis, we performed a power analysis with the formula developed by Riley et al., setting a magnitude of required shrinkage of predictor effects of 0.06 [21] and obtaining a required sample size of 220 patients and 4.4 events per variable.
The risk scores for the expected outcomes (PERI-Gastric 1 and 2) were calculated according to the constant and regression coefficients of the variables in the final multivariable model, and a conversion from odds ratios (ORs) to risk probability coefficients was performed according to the following formula p = exp (OR)/(1 + exp(OR)) × 100 to obtain a probability score of developing peritoneal carcinomatosis that is expressed from 0 to 100%. In parallel to the PERI-Gastric point scores, a nomogram (the PERI-gram 1 and 2) was created using the Stata nomolog function [22].
Discrimination was assessed with the area under the curve (AUC) of receiver operating curves (ROCs) with the corresponding 95% confidence interval (95% CI). Calibration graphs were constructed by plotting the actual rate of peritoneal recurrence versus the predicted rate of peritoneal recurrence with the Stata pmcalplot function and calculating the slope equations with the Curve Estimation function in SPSS [23]. Internal validation was performed according to a bootstrap resampling method (1000 iterations) [24]: discrimination was assessed using the Stata command rocreg, and calibration was tested with the calibrationbelt function and bootstrap resampling with pmcalplot [23, 25]. All analyses were performed using IBM SPSS for Macintosh, v. 25 (IBM Co., Armonk, NY, USA), Stata for Windows v. 15.0 (StataCorp, College Station, TX, USA) and Microsoft Excel for Macintosh v 16.3.1 (Microsoft Corporation (2018); retrieved from https://office.microsoft.com/excel). All tests were 2-sided with a significance level of 0.05.
Results
Study population
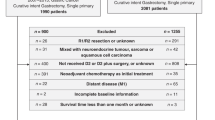
According to the inclusion and exclusion criteria, from an initial population of 1580 patients undergoing gastrectomy for GC, we selected 645 patients for inclusion in this study (Fig. 1). Their clinicopathologic characteristics are presented in Table 1. The median OS of survivors was 78 months (range 16–267). In patients with peritoneal recurrence, the median disease-free survival was 18 months (range 1–161), the median overall survival (OS) was 25 months after gastrectomy (range 5–184 months), and the median progression-free survival after recurrence was 5 months (range 0–55).

Flowchart of the selection process of the study population according to the inclusion and exclusion criteria
Creation of the prognostic models, point scores and nomograms
To define the variables independently associated with peritoneal recurrence, two regressions were conducted using the Lauren classification and the presence of SRCs as major indicators of tumor histology, respectively (Tables 2, 3). According to the results, two point scores were created. The PERI-Gastric model including the Lauren classification (the PERI-Gastric 1) presented a – 2 log likelihood of 302 and a Nagelkerke R2 of 0.287. The PERI-Gastric model including the presence of SRCs (the PERI-Gastric 2) presented a– 2 log likelihood of 305 and a Nagelkerke R2 of 0.270.
The PERI-Gram 1 (Lauren) and 2 (SRC) nomograms visually displaying these models are presented in Fig. 2a, b.

a The PERI-Gram 1—prognostic nomogram predicting the risk of metachronous peritoneal carcinomatosis after curative gastrectomy, which was derived from multivariable logistic regression including 5 variables: the Lauren histotype, pathological N2 or N3 disease (involvement of more than 3 lymph nodes), pathologic T3 or T4 disease, stump GC or a GC presenting as linitis plastica (GC involving more than 2/3 of the stomach). b The PERI-Gram 2—prognostic nomogram predicting the risk of metachronous peritoneal carcinomatosis after curative gastrectomy, which was derived from multivariable logistic regression including 5 variables: the presence of SRC features, pathological N2 or N3 disease (involvement of more than 3 lymph nodes), pathologic T3 or T4 disease, stump GC or a GC presenting as linitis plastica (GC involving more than 2/3 of the stomach)
Discrimination, calibration and internal validation of the models
When discrimination and calibration were tested in the whole population of the study, the AUC under the ROC curve (Fig. 2) was 0.828 (0.778–0.877) for the model including the Lauren classification and 0.805 (0.755–0.855) for the model including SRCs. The assessment of the calibration plot showed that both models had good calibration, with coordinates for the linear equations of y = 0.61 + 1.020 × x for the PERI-Gastric 1 and y = 0.31 + 0.990 × x for the PERI-Gastric 2 (Fig. 2).
After bootstrap resampling, the mean AUCs under the ROC curve ± SD were 0.775 (0.721–0.830) and 0.749 (0.693–0.805). The calibration plot showed good accuracy for both models, with a 95% CI estimate for the slope of 0.852–1.505 for the PERI-Gastric 1 and 0.777–1.351 for the PERI-Gastric 2 (Fig. 3).

ROC curves representing the discrimination of the PERI-Gastric 1 (a) and 2 (b), respectively; Calibration curves for the PERI-Gastric 1 (c) and 2 (d), respectively
Discussion
In this study, we present two prognostic models that can quantify the risk for metachronous peritoneal carcinomatosis after gastrectomy with curative intent. Variables significantly associated with peritoneal recurrence were linitis plastica, stump GC, pT3–4, pN2–3, and the Lauren classification/SRC histology.
Both models were shown to have good discrimination and accuracy, especially in the range of probability of peritoneal recurrence from 0 to 30–40% (Fig. 2c, d).
This study is in accordance with others that estimated the risk of peritoneal recurrence after gastrectomy with curative intent, which reported similar risk factors (pT4, positive nodal status, signet ring cells and undifferentiated gradings) [10]. In 2014, one Asian study developed a prognostic point score for peritoneal recurrence in 481 patients undergoing gastrectomy and adjuvant therapy (Fig. 4). This study identified pT ≥ 3, pN3, Borrmann type 4, Ming infiltrative type and venous invasion as prognostic factors [8]. A 2020 Western study of 274 patients developed a prognostic score to identify patients at an increased risk of peritoneal recurrence after curative gastrectomy, identifying sex, pT stage, grading and signet ring cell histology as significant variables and detecting an 8.8-fold increased risk of peritoneal recurrence in patients with 3 or 4 of these factors [16]. This study included only patients with previously documented GC recurrence, and therefore, its clinical applicability was limited. The present study aimed to create an instrument capable of intraoperative risk stratification for all GC patients, allowing accurate planning of the surgical procedure and possible adjunctive intraperitoneal procedures.

Calibration curves and confidence intervals obtained with the calbrationbelt Stata function for the PERI-Gastric 1 (a) and 2 (b), respectively
According to previous reports, linitis plastica is associated with an increased risk of peritoneal recurrence [26, 27]. There are few reports on the biological behavior of stump GC in the Western literature, accounting for only a small number of cases [28], while in Eastern countries with screening programs, the outcomes of early-detected stump GC are reported to be similar to those of primary early GC [29]. Accordingly, the risk of metachronous peritoneal carcinomatosis in patients with stump early GC in the nomogram is below 5%. Nevertheless, studies conducted in Japan before the beginning of the national screening program and in other Eastern countries without a screening program reported that stump GC is usually associated with a worse prognosis [30], diagnosed at a highly advanced stage, with distant lymph node and peritoneal involvement [31].
The combinations of advanced pT (pT3–4), advanced pN stage (pN2–3) and specific histopathology (Lauren diffuse or SRC GC) accounted for only approximately 30% of the risk of peritoneal carcinomatosis. The remaining risk, rather than being random, could be represented by unmeasured positive cytology (reported as positive in up to 13.2% of patients without macroscopic peritoneal disease [27]) and peritoneal contamination occurring during surgery [32] (currently unmeasured).
The main implication of this study is the potential for change in the clinical practice. The application of prophylactic intraperitoneal treatments is still controversial due to an unclear balance between their efficacy and the risk of overtreatment, as an increased rate of postoperative complications could occur even in expert hands [11, 12]. Moreover, the healthcare costs of intraperitoneal treatment are a major issue not only in countries with an insurance-based health system but also in countries with a DRG (Diagnosed related groups) reimbursement system [33]. Indeed, in the current (Western) guidelines, intraperitoneal adjuvant prophylactic therapies are not recommended outside of the context of clinical research [34, 35]. This article aims to be a starting point for setting the criteria to administer prophylactic intraperitoneal treatments, only if their efficacy will be validated.
Among the prophylactic intraperitoneal treatments, HIPEC is probably the most studied, followed by early postoperative intraperitoneal chemotherapy (EPIC) and normothermic intraperitoneal chemotherapy (NIC). Prophylactic intraperitoneal chemotherapy after gastrectomy carries a nonnegligible increase in postoperative morbidity (reported odds ratios range from 1.74 to 1.82) [11, 12], and its efficacy is still debated. Indeed, previous Western RCTs have not proven that there is a survival benefit for prophylactic HIPEC [36, 37], even though the negative results of these studies could be concluded to be due to a low study power caused by a small sample size and possible inappropriate selection of included patients. Some promising results for prophylactic HIPEC were detected in Japanese RCTs [38, 39]. A 2014 meta-analysis of RCTs including all prophylactic strategies (HIPEC, EPIC and NIC) reported a significant reduction in peritoneal recurrence in patients treated with intraperitoneal chemotherapy versus surgery alone (OR 0.47, 95% CI 0.35–0.63) [11]. However, another recent meta-analysis of randomized and nonrandomized clinical studies on prophylactic HIPEC have not proven that this strategy has a significant effect on survival and peritoneal recurrence in the RCT arm (even if a tendency toward significance was documented and borderline significance was identified for 5-year survival—OR 0.82 95% CI 0.67–1.00) [12]. Recently, a Chinese randomized case–control study reported a significantly higher 3-year DFS rate (93 vs 65%) and lower peritoneal recurrence rate (23 vs 3%) for prophylactic HIPEC versus standard gastrectomy [40]. The European GASTRICHIP phase III RCT, which is currently ongoing, is evaluating the survival benefit of prophylactic HIPEC as an adjunct to perioperative therapy and gastrectomy in patients with T4 or N+ disease and/or positive cytology [41], and another RCT with the same purpose, the GOETH, was recently registered [42].
Notwithstanding the results of these RCTs, it should be clear that for patients at high risk for peritoneal carcinomatosis (due to undetected positive cytology, contamination occurring during surgery, or disease biology), effective strategies to prevent peritoneal carcinomatosis are strongly needed. Indeed, peritoneal recurrence is frequent, poorly preventable with the current clinical strategies and has devastating implications, as patients developing metachronous peritoneal carcinomatosis have a dismal prognosis and poor survival (usually < 8 months) [6, 7]. A high risk of peritoneal recurrence (i.e. ≥ 25 to 30%), independent of the administration of systemic therapy, could be a strong rationale for the use of prophylactic intraperitoneal treatments, after an accurate risk/benefit analysis of the long-term risks associated with peritoneal recurrence and the short-term risks associated with the specific intraperitoneal procedure. In the future, if prophylactic intraperitoneal procedures would be validated as effective measures, it could even be hypothesized that GC patients at high risk of peritoneal recurrence may be better treated in centers with such an expertise, or that the skill set of a gastric cancer surgeon should include a specific training in intraperitoneal procedures.
This study included both patients undergoing perioperative treatment or upfront surgery and those undergoing or not undergoing adjuvant treatment. This could be considered a confounding bias, even though treatment bias was adjusted for in the logistic multivariable analysis, and no significant associations were detected between both neoadjuvant and adjuvant therapy and peritoneal recurrence. This is in line with our previous results [9] and with other studies reporting that peritoneal recurrence is rarely controlled with preoperative systemic chemotherapy [4, 10]. Moreover, peritoneal recurrence is the most common recurrence type even in patients treated with adjuvant chemotherapy [8]. This has been attributed to the limited obtainable drug concentration in the peritoneal cavity by most systemic chemotherapeutics [43]. For the aim of this study, we considered all patients undergoing curative intent D1+ and D2 gastrectomy with peritoneal carcinomatosis as the first site of recurrence, hence the recurrence rate (9.9%) is apparently lower compared with the rate reported in literature usually based only on Stage II–III or on patients with recurrence. Overall, these data do not seem to differ significantly from those of the available Western literature [44, 45].
The main weakness of this study was that the pathological variables included in the score were obtained postoperatively, limiting the value of a score intended for use as a preoperative/intraoperative risk assessment. This is the same limitation of most RCTs on prophylactic HIPEC, that include patients based on the preoperative/intraoperative staging [40, 42]. However, the pathologic type (Lauren and SRC) and the disease staging may be determined preoperatively (from endoscopic biopsies and preoperative staging exams) [46, 47], allowing for appropriate intraoperative decisions regarding the need for prophylactic intraperitoneal treatments. The accuracy of the clinical staging of GC is often reported to be suboptimal [48] but could nonetheless be optimized by the combination of diagnostic endoscopy as well as staging CT scan and diagnostic laparoscopy [49], and there are active research topics in the fields of image processing and interpretation by artificial intelligence methods that could further increase the accuracy of clinical staging in the next years [50]. Another limitation of this study is the unavailability of peritoneal cytology for most of the included patients. Positive cytology indicates stage IV disease and is a prognostic factor associated with worse outcomes and higher peritoneal recurrence rates. However, the cytologic examination has been found to have low sensitivity and poor reproducibility in most centers and is often not obtainable intraoperatively with the current available methods [51, 52]. Moreover, the cytology status of some patients could change before and after preoperative chemotherapy [53]. Due to these current limitations, patients with positive cytology are usually included in trials on prophylactic HIPEC [41, 42]. Due to the relevance of this topic, a widespread use of diagnostic laparoscopy and the effort to introduce fast and reliable techniques for cytology in every gastric cancer center should be valued to improve the intraoperative estimation of the risk of peritoneal diffusion (due to pre-existing peritoneal free cancer cells or contamination occurring during surgery) [54, 55].
This is the largest multicentric Western study that developed a prognostic model to assess the risk of peritoneal recurrence after gastrectomy with curative intent. It was also the first to develop a point score and prognostic nomogram. Nomograms are visual representations of point scores. Both nomograms and point scores can assess the probability of a clinical event, and therefore, they have been regarded as an immediate, yet more advanced, method compared with traditional staging systems (i.e., the TNM). They have the advantage of estimating individualized risks and the potential to improve decisions on targeted treatments [56]. Previous studies showed a similar recurrence pattern for patients treated with a curative aim at Western centers [5, 9], suggesting that this score could be widely applicable for at least stratifying the risk of Western GC patients.
Overall, according to current knowledge and clinical practice, we believe that the PERI-Gastric and the PERI-Gram represent practical and effective instruments for predicting the prognosis of radically resected GC patients in terms of the risk of peritoneal recurrence. They are valuable for identifying a subset of patients who could benefit from the application of effective intraperitoneal prophylactic treatments. Moreover, they could help with the accurate risk stratification of patients included in previous low-power RCTs and appropriate enrollment of future RCTs on prophylactic intraperitoneal treatments. Last, they could be used to identify categories at high-risk risk of peritoneal carcinomatosis to improve the follow-up plans (i.e., posing an early suspect of recurrence).
Conclusions
The PERI-Gastric and PERI-Gram make it possible to quantify the risk of metachronous peritoneal carcinomatosis and represent useful tools for improving decision making for patients undergoing gastrectomy with curative intent and selecting high-risk patients for prophylactic intraperitoneal treatments. They could also be useful for weighing the results of past and future RCTs assessing the benefits of prophylactic HIPEC based on the actual risk of peritoneal carcinomatosis in every patient. A free online calculation tool based on the PERI-Gastric models is available at the following link: www.perigastric.org.
References
D’Angelica M, Gonen M, Brennan MF, et al. Patterns of initial recurrence in completely resected gastric adenocarcinoma. Ann Surg. 2004;240(5):808–16. https://doi.org/10.1097/01.sla.0000143245.28656.15.
Liu D, Lu M, Li J, et al. The patterns and timing of recurrence after curative resection for gastric cancer in China. World J Surg Oncol. 2016. https://doi.org/10.1186/s12957-016-1042-y.
Guner A, Yildirim R. Surgical management of metastatic gastric cancer: moving beyond the guidelines. Transl Gastroenterol Hepatol. 2019. https://doi.org/10.21037/tgh.2019.08.03.
Ikoma N, Chen HC, Wang X, et al. Patterns of initial recurrence in gastric adenocarcinoma in the era of preoperative therapy. Ann Surg Oncol. 2017. https://doi.org/10.1245/s10434-017-5838-y.
Spolverato G, Ejaz A, Kim Y, et al. Rates and patterns of recurrence after curative intent resection for gastric cancer: a United States multi-institutional analysis. J Am Coll Surg. 2014. https://doi.org/10.1016/j.jamcollsurg.2014.03.062.
Wei J, Yang Y, Du J, et al. Peritoneal metastasis in relation to outcome and therapeutic strategy in gastric cancer. Transl Cancer Res. 2017. https://doi.org/10.21037/tcr.2017.01.13.
Thomassen I, Van Gestel YR, Van Ramshorst B, et al. Peritoneal carcinomatosis of gastric origin: a population-based study on incidence, survival and risk factors. Int J Cancer. 2014. https://doi.org/10.1002/ijc.28373.
Lee JH, Son SY, Lee CM, et al. Factors predicting peritoneal recurrence in advanced gastric cancer: implication for adjuvant intraperitoneal chemotherapy. Gastric Cancer. 2014. https://doi.org/10.1007/s10120-013-0306-2.
Agnes A, Biondi A, Laurino A, et al. A detailed analysis of the recurrence timing and pattern after curative surgery in patients undergoing neoadjuvant therapy or upfront surgery for gastric cancer. J Surg Oncol. 2020. https://doi.org/10.1002/jso.25959.
Seyfried F, von Rahden BH, Miras AD, et al. Incidence, time course and independent risk factors for metachronous peritoneal carcinomatosis of gastric origin—a longitudinal experience from a prospectively collected database of 1108 patients. BMC Cancer. 2015. https://doi.org/10.1186/s12885-015-1081-8.
Coccolini F, Cotte E, Glehen O, et al. Intraperitoneal chemotherapy in advanced gastric cancer. Meta-analysis of randomized trials. Eur J Surg Oncol. 2014;40(1):12–26. https://doi.org/10.1016/j.ejso.2013.10.019.
Desiderio J, Chao J, Melstrom L, et al. The 30-year experience—a meta-analysis of randomised and high-quality non-randomised studies of hyperthermic intraperitoneal chemotherapy in the treatment of gastric cancer. Eur J Cancer. 2017;79:1–14. https://doi.org/10.1016/j.ejca.2017.03.030.
Marrelli D, Roviello F, De Manzoni G, et al. Different patterns of recurrence in gastric cancer depending on Lauren’s histological type: Longitudinal study. World J Surg. 2002. https://doi.org/10.1007/s00268-002-6344-2.
Aoyama T, Yoshikawa T, Hayashi T, et al. Risk factors for peritoneal recurrence in stage II/III gastric cancer patients who received S-1 adjuvant chemotherapy after D2 gastrectomy. Ann Surg Oncol. 2012. https://doi.org/10.1245/s10434-011-2158-5.
Roviello F, Marrelli D, De Manzoni G, et al. Prospective study of peritoneal recurrence after curative surgery for gastric cancer. BJS. 2003. https://doi.org/10.1002/bjs.4164.
Kus T, Kose F, Aktas G, et al. Prediction of peritoneal recurrence in patients with gastric cancer: a multicenter study. J Gastrointest Cancer. 2020. https://doi.org/10.1007/s12029-020-00419-7.
Moons KGM, Altman DG, Reitsma JB, et al. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): explanation and elaboration. Ann Intern Med. 2015. https://doi.org/10.7326/M14-0698.
Amin MB, Edge S, Greene F, et al. AJCC cancer staging manual Eighth edition. Springer Int Publ. 2017. https://doi.org/10.1007/978-3-319-40618-3.
Mariette C, Carneiro F, Grabsch HI, et al. Consensus on the pathological definition and classification of poorly cohesive gastric carcinoma. Gastric Cancer. 2019. https://doi.org/10.1007/s10120-018-0868-0.
Charalampakis N, Nogueras González GM, Elimova E, et al. The proportion of signet ring cell component in patients with localized gastric adenocarcinoma correlates with the degree of response to pre-operative chemoradiation. Oncology. 2016. https://doi.org/10.1159/000443506.
Riley RD, Ensor J, Snell KIE, et al. Calculating the sample size required for developing a clinical prediction model. BMJ. 2020. https://doi.org/10.1136/bmj.m441.
Zlotnik A, Abraira V. A general-purpose nomogram generator for predictive logistic regression models. Stata J. 2015. https://doi.org/10.1177/1536867x1501500212.
Ensor J, Snell KI, Martin EC. PMCALPLOT: stata module to produce calibration plot of prediction model performance. Stat Softw Components. 2020.
Iasonos A, Schrag D, Raj GV, Panageas KS. How to build and interpret a nomogram for cancer prognosis. J Clin Oncol. 2008;26(8):1364–70. https://doi.org/10.1200/JCO.2007.12.9791.
Nattino G, Lemeshow S, Phillips G, et al. Assessing the calibration of dichotomous outcome models with the calibration belt. Stata J. 2017. https://doi.org/10.1177/1536867X1801700414.
Kodera Y, Nakanishi H, Ito S, et al. Detection of disseminated cancer cells in linitis plastica-type gastric carcinoma. Jpn J Clin Oncol. 2004. https://doi.org/10.1093/jjco/hyh097.
Ikoma N, Blum M, Chiang YJ, et al. Yield of staging laparoscopy and lavage cytology for radiologically occult peritoneal carcinomatosis of gastric cancer. Ann Surg Oncol. 2016. https://doi.org/10.1245/s10434-016-5409-7.
Tran TB, Hatzaras I, Worhunsky DJ, et al. Gastric remnant cancer: a distinct entity or simply another proximal gastric cancer? J Surg Oncol. 2015. https://doi.org/10.1002/jso.24080.
Shimada H, Fukagawa T, Haga Y, Oba K. Does remnant gastric cancer really differ from primary gastric cancer? A systematic review of the literature by the Task Force of Japanese Gastric Cancer Association. Gastric Cancer. 2016. https://doi.org/10.1007/s10120-015-0582-0.
Chen QY, Zhong Q, Zhou JF, et al. Conditional survival and recurrence of remnant gastric cancer after surgical resection: a multi-institutional study. Cancer Sci. 2020. https://doi.org/10.1111/cas.14231.
Yonemura Y, Sugiyama K, Fujimura T, et al. A new surgical technique (left upper abdominal evisceration) for advanced carcinoma of the gastric stump. Hepatogastroenterology. 1994.
Takebayashi K, Murata S, Yamamoto H, et al. Surgery-induced peritoneal cancer cells in patients who have undergone curative gastrectomy for gastric cancer. Ann Surg Oncol. 2014. https://doi.org/10.1245/s10434-014-3525-9.
Naffouje SA, O’Donoghue C, Salti GI. Evaluation of cytoreductive surgery and hyperthermic intraperitoneal chemotherapy in a community setting: a cost-utility analysis of a hospital’s initial experience and reflections on the health care system. J Surg Oncol. 2016;113(5):544–7. https://doi.org/10.1002/jso.24162.
Ajani J, D’Amico T, Bentrem D, et al. NCCN clinical practice guidelines in oncology gastric cancer—Version 4.2021. 2021. https://www.nccn.org/.
Smyth EC, Verheij M, Allum W, et al. Gastric cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2016. https://doi.org/10.1093/annonc/mdw350.
Sautner T, Hofbauer F, Depisch D, et al. Adjuvant intraperitoneal cisplatin chemotherapy does not improve long-term survival after surgery for advanced gastric cancer. J Clin Oncol. 1994. https://doi.org/10.1200/JCO.1994.12.5.970.
Rosen HR, Jatzko G, Repse S, et al. Adjuvant intraperitoneal chemotherapy with carbon-adsorbed mitomycin in patients with gastric cancer: results of a randomized multicenter trial of the Austrian Working Group for Surgical Oncology. J Clin Oncol. 1998. https://doi.org/10.1200/JCO.1998.16.8.2733.
Fujimoto S, Takahashi M, Mutou T, et al. Successful intraperitoneal hyperthermic chemoperfusion for the prevention of postoperative peritoneal recurrence in patients with advanced gastric carcinoma. Cancer. 1999. https://doi.org/10.1002/(SICI)1097-0142(19990201)85:3%3c529::AID-CNCR3%3e3.0.CO;2-9.
Yonemura Y, De Aretxabala X, Fujimura T, et al. Intraoperative chemohyperthermic peritoneal perfusion as an adjuvant to gastric cancer: final results of a randomized controlled study. Hepatogastroenterology. 2001.
Beeharry MK, Zhu Z-L, Liu W-T, et al. Prophylactic HIPEC with radical D2 gastrectomy improves survival and peritoneal recurrence rates for locally advanced gastric cancer: personal experience from a randomized case control study. BMC Cancer. 2019;19:932. https://doi.org/10.1186/s12885-019-6125-z.
Glehen O, Passot G, Villeneuve L, et al. GASTRICHIP: D2 resection and hyperthermic intraperitoneal chemotherapy in locally advanced gastric carcinoma: a randomized and multicenter phase III study. BMC Cancer. 2014. https://doi.org/10.1186/1471-2407-14-183.
Prophylactic Surgery Plus HIPEC With CO2 in patients affected by gastric carcinoma. GOETH Study—Full Text View—ClinicalTrials.gov. 2019. https://clinicaltrials.gov/ct2/show/NCT03917173.
Lagast N, Carlier C, Ceelen WP. Pharmacokinetics and tissue transport of intraperitoneal chemotherapy. Surg Oncol Clin N Am. 2018. https://doi.org/10.1016/j.soc.2018.02.003.
Spolverato G, et al. Rates and patterns of recurrence after curative intent resection for gastric cancer: a united states multi-institutional analysis. J Am Coll Surg. 2014;219(4):664–75. https://doi.org/10.1016/j.jamcollsurg.2014.03.062.
Roviello F, Marrelli D, de Manzoni G, Morgagni P, Di Leo A, Saragoni L, De Stefano A. Prospective study of peritoneal recurrence after curative surgery for gastric cancer. Br J Surg. 2003;90(9):1113–9. https://doi.org/10.1002/bjs.4164.
Makino T, Fujiwara Y, Takiguchi S, et al. Preoperative T staging of gastric cancer by multi-detector row computed tomography. Surgery. 2011. https://doi.org/10.1016/j.surg.2010.12.003.
Chao Y, Zhu ZG, Yan M, et al. Value of multidetector-row computed tomography in the preoperative T and N staging of gastric carcinoma: a large-scale Chinese study. J Surg Oncol. 2009. https://doi.org/10.1002/jso.21316.
Vergadis C, Schizas D. Is accurate N-staging for gastric cancer possible? Front Surg. 2018;5:41. https://doi.org/10.3389/fsurg.2018.00041.
Fukagawa T. Role of staging laparoscopy for gastric cancer patients. Ann Gastroenterol Surg. 2019;3(5):496–505. https://doi.org/10.1002/ags3.12283.
Zhang XP, Wang ZL, Tang L, Sun YS, Cao K, Gao Y. Support vector machine model for diagnosis of lymph node metastasis in gastric cancer with multidetector computed tomography: a preliminary study. BMC Cancer. 2011. https://doi.org/10.1186/1471-2407-11-10.
Yepuri N, Bahary N, Jain A, Dhir M. Review and update on the role of peritoneal cytology in the treatment of gastric cancer. J Surg Res. 2019;235:607–14. https://doi.org/10.1016/j.jss.2018.10.049.
McMullen JRW, Selleck M, Wall NR, Senthil M. Peritoneal carcinomatosis: limits of diagnosis and the case for liquid biopsy. Oncotarget. 2017;8:43481–90. https://doi.org/10.18632/oncotarget.16480.
Jamel S, Markar SR, Malietzis G, Acharya A, Athanasiou T, Hanna GB. Prognostic significance of peritoneal lavage cytology in staging gastric cancer: systematic review and meta-analysis. Gastric Cancer. 2018;21(1):10–8. https://doi.org/10.1007/s10120-017-0749-y.
Gęca K, Rawicz-Pruszyński K, Mielko J, et al. Rapid detection of free cancer cells in intraoperative peritoneal lavage using one-step nucleic acid amplification (OSNA) in gastric cancer patients. Cells. 2020. https://doi.org/10.3390/cells9102168.
Jagric T, Potrc S, Mis K, et al. Flow cytometry as the new “gold standard” for detection of free tumour cells in abdominal lavage fluid in gastric cancer patients: a comparative study of molecular and conventional methods. Surg Pract. 2016. https://doi.org/10.1111/1744-1633.12173.
Balachandran VP, Gonen M, Smith JJ, DeMatteo RP. Nomograms in oncology: more than meets the eye. Lancet Oncol. 2015;16(4):e173–80. https://doi.org/10.1016/S1470-2045(14)71116-7.
Acknowledgements
We thank Nikola Dino Capocchiano—Fondazione Policlinico Universitario Agostino Gemelli IRCCS—for the website IT support and design.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
Procedures were followed as outlined in accordance with ethical standards formulated in the Helsinki Declaration 1975 and later versions. An approval was obtained from the local Ethics Committee (ID number: 3694).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Agnes, A., Biondi, A., Persiani, R. et al. Development of the PERI-Gastric (PEritoneal Recurrence Index) and PERI-Gram (Peritoneal Recurrence Index NomoGRAM) for predicting the risk of metachronous peritoneal carcinomatosis after gastrectomy with curative intent for gastric cancer. Gastric Cancer 25, 629–639 (2022). https://doi.org/10.1007/s10120-021-01268-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10120-021-01268-4