
Abstract
Objective
To explore whether cumulative serum urate (cumSU) is correlated with diabetes type II mellitus incidence.
Methods
In this study, we recruited individuals participating in all Kailuan health examinations from 2006 to 2013 without stroke, cancer, gestation, myocardial infarction, and diabetes type II diagnosis in the first three examinations. CumSU was calculated by multiplying the average serum urate concentration and the time between the two examinations (umol/L × year). CumSU levels were categorized into five groups: Q1–Q5. The effect of cumSU on diabetes type II incidence was estimated by logistic regression.
Results
A total of 36,277 individuals (27,077 men and 9200 women) participated in the final analysis. The multivariate logistic regression model showed the odds ratios (95% confidence intervals) of diabetes type II from Q1 to Q5 were 1.00 (reference), 1.25 (1.00 to 1.56), 1.43 (1.15 to 1.79), 1.49 (1.18 to 1.87), and 1.80 (1.40 to 2.32), respectively. Multivariable odds ratios per 1-standard deviation increase in cumSU were 1.26 (1.17 to 1.37) in all populations, 1.20 (1.10 to 1.32) for men, and 1.52 (1.27 to 1.81) for women, respectively.
Conclusions
CumSU is a significant risk factor for diabetes type II. Individuals with higher cumSU, especially women, are at a higher risk of diabetes type II independent of other known risk factors.
Key Points • Cumulative exposure to serum urate is a significant risk factor for diabetes type II. • Individuals with higher cumSU, especially women, are at a higher risk of diabetes type II. |
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Serum urate (SU), an end product of purine metabolism [1], correlates with many recognized cardiovascular risk factors [2] including age, male sex, hypertension, hypertriglyceridemia, obesity, insulin resistance, and metabolic syndrome [3,4,5]. However, the association between cumulative serum urate (cumSU) levels and diabetes type II mellitus is unclear. While some studies report a positive association between high SU levels and diabetes type II [5,6,7,8,9], others report either no association [10] or an inverse relationship [11]. Moreover, most studies examining the association between baseline SU and diabetes type II incidence have not investigated how cumSU affects blood sugar levels or diabetes type II incidence. We hypothesized that higher levels of cumSU are associated with greater incidence of diabetes type II mellitus.
We conducted this study in a large sample of Chinese adults to investigate the relationship between cumSU and diabetes type II mellitus incidence after adjusting for major confounders.
Methods
Study design and population
The Kailuan Study [12] is a prospective cohort study conducted in the Kailuan community in Tangshan City, China. From June 2006 to October 2007, a total of 101,510 participants (81,110 men and 20,400 women) aged 18–98 years were recruited to participate in the Kailuan Study. They were subsequently followed-up in three subsequent visits in 2008–2009, 2010–2011, and 2012–2013. The current analysis is based on a subgroup of 36,277 individuals (27,077 men and 9200 women) with complete follow-up data available and without diabetes type II mellitus prior to their last visit (Fig. 1). Subjects diagnosed with myocardial infarction, stroke, cancer, or pregnancy during the visits were excluded.

Flow Chart Describing the Selection and Subsequent Loss of Participants: Selection of Kailuan Study Participants. The Kailuan Study: A prospective cohort study conducted in the Kailuan community in Tangshan City, China. The Time of the study: From June 2006 to October 2007. Study Population: 101,510 participants. They were subsequently followed-up in three subsequent visits in 2008–2009, 2010–2011, and 2012–2013. The current analysis is based on a subgroup of 36,277 individuals with complete follow-up data available and without diabetes mellitus prior to their last visit.
Assessment of health metrics
Information on age, sex, disease history, medication (including insulin, oral hypoglycemic agents, diuretics, and antihypertensive drug use), physical activity, smoking, alcohol intake, and education was collected via questionnaires at baseline and each of the three follow-up visits. Height, weight, and blood pressure were examined by trained physician staff. All measurements were performed using standardized protocols described previously [12]. Blood samples were collected from the antecubital vein after overnight fasting. Fasting blood glucose was measured using the hexokinase/glucose-6-phosphate-dehydrogenase method. Total cholesterol and triglycerides were assessed enzymatically. High-density lipoprotein cholesterol and low-density lipoprotein cholesterol levels were determined using a direct test method (inter-assay coefficient of variation < 10%; Mind Bioengineering Co. Ltd., Shanghai, China). SU concentrations were determined using oxidase method. All biochemical variables were assessed at the central laboratory of Kailuan General Hospital with using a Hitachi autoanalyzer (Hitachi 747; Hitachi, Tokyo, Japan).
Diabetes type II is diagnosed as fasting glucose ≥ 7 mmol/L, or fasting glucose ≤ 7 mmol/L with the use of insulin or oral hypoglycemic agents. Systolic and diastolic blood pressures were averaged across 2 measurements. Hypertension was defined as a mean systolic blood pressure ≥ 140 mmHg and/or a mean diastolic blood pressure ≥ 90 mmHg, or a mean systolic blood pressure < 140 mmHg and/or a mean diastolic blood pressure < 90 mmHg after treatment. Estimated glomerular filtration rate (mL/min/1.73 m2) was calculated by CKD-EPI. Body mass index was calculated as body weight (kg) divided by the square of body height (m2). Smoking was defined as consumption of 1 cigarette every day for at least 1 year. Drinking was defined as consuming on average 100-mL wine (or alcohol content over 50%) per day for more than 1 year. Physical activity was defined as performing at least 30-min exercise more than 3 times a week. Education was defined as high school education level or above. Positive family history of diabetes type II means first-degree relative has been diagnosed with diabetes type II.
Cumulative serum urate
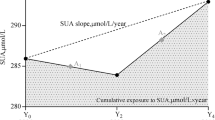
CumSU was defined as the summation of average SU for each pair of consecutive examinations multiplied by the time between these two consecutive visits in years:
[((SU1 + SU2)/2) × time1–2] + [((SU2 + SU3)/2) × time2–3] + [((SU3 + SU4)/2) × time3–4], where SU1, SU2, SU3, and SU4 indicate SU at examinations 1 (baseline), 2, 3, and 4, respectively [13,14,15,16]. Time1–2, time2–3, and time3–4 indicate the participant-specific time interval between consecutive examinations 1–4 in years. For men, CumSU was categorized in μmol/L × year as < 1499 (Q1 group), 1499–1739 (Q2 group), 1739–1971 (Q3 group), 1971–2261 (Q4 group), and ≥ 2261 (Q5 group). For women, cumSU was categorized as < 1259 (Q1 group), 1259–1435 (Q2 group), 1435–1602 (Q3 group), 1602–1841 (Q4 group), and ≥ 1841 (Q5 group).
Statistical analyses
Statistical analyses were performed with SPSS 13.0. Continuous variables were described as mean (standard deviation, SD). Comparison among different groups was analyzed by one-way analysis of variance. Categorical variables were described as percentages and were compared using chi-square tests (χ2 tests). Logistic regression model was used to estimate the risk of diabetes type II with cumSU metrics. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. We fitted three multivariate models. Model 1 is a univariate logistic regression analysis without adjustment. Model 2 is adjusted by baseline age and sex from model 1. Model 3 is adjusted by education level, physical activity, smoking, alcohol consumption, family history of diabetes type II, baseline hypertension, diuretics usage, body mass index, fasting blood glucose, SU, total cholesterol, triglycerides, and estimated glomerular filtration rate. Logistic regression analysis was used to evaluate the effect of one SD increase of cumSU on the new onset of diabetes type II. The significance level was set at P < 0.05.
Results
Data of population
Out of the 101,510 individuals participating in the baseline examination, 47,828 subjects underwent all 4 visits. The number of cases excluded due to diabetes type II diagnosis prior to the last visit was 6762. Moreover, 903, 1412, and 247 cases were excluded due to diagnosis of myocardial infarction, stroke, and cancer, respectively, during any visit. Two hundred eighty-six individuals were excluded due to pregnancy. We also excluded 1941 participants due to missing data of blood glucose and SU. The remaining 36,277 participants were included in the present study (Fig. 1). Among them, 9200 participants were women, and 27,077 cases were men. The mean age of the participants was 47.33 (11.48) years. For women, the average age was 46.88 (10.57) years. For men, the average age was 47.49 (11.77) years.
Baseline data among different groups
Q1 group occupies 19.99% of all the subjects, whereas Q2–Q5 occupies 19.97%, 20.05%, 19.97%, and 20.02%, respectively. As compared with the baseline data obtained in 2006, there were significant differences in sex, age, hypertension, diuretics use, body mass index, fasting blood glucose, SU, total cholesterol, triglycerides, estimated glomerular filtration rate, family history of diabetes type II, smoking, alcohol intake, physical activity, and education among the 5 groups (Table 1, P < 0.05).
Incidence of new-onset diabetes type II among different groups
The incidence of new-onset diabetes type II in the last visit was 3.34%, with 1212 cases diagnosed during the last visit. In Q1, Q2, Q3, Q4, and Q5, 166, 206, 239, 258, and 343 cases were diagnosed, respectively. The incidence of new-onset diabetes type II was 2.29%, 2.84%, 3.29%, 3.56%, and 4.72%, in Q1–Q5 groups, respectively. In the incidence of new-onset diabetes type II, men scored higher than women in the Q1, Q2, and Q3 groups, while no differences between men and women in Q4 and Q5 groups were observed (Fig. 2).

Incidence of new-onset diabetes among different groups. SU, serum urate; DM, diabetes mellitus. **P < 0.05
Risk factor analysis to diabetes type II
As compared with Q1 group, the odds ratio of new-onset diabetes type II incidence was 1.25, 1.45, 1.58, and 2.12 in Q2, Q3, Q4, and Q5 groups, respectively. After complete adjustment (model 3), OR in Q2–Q4 was slightly increased while OR in Q5 group decreased from 2.12 to 1.80. The trend was more obvious for women than men. Multivariate adjusted ORs for the incidence of diabetes type II corresponding to a 1-S.D. increase in cumSU were 1.20 in men and 1.52 in women. We found a similar trend across age groups (Table 2).
Sensitivity analysis
To exclude the influence of hypertension and antihypertensive therapy on the association between cumSU and incidence of diabetes type II, a sensitivity analysis was performed after excluding 15,945 patients with hypertension. We found the association between cumSU and incidence of diabetes type II was unaffected (Table 3).
Discussion
Recently, hyperuricemia has been proposed as a novel risk factor for diabetes type II, but the results from epidemiologic studies have been mixed [5,6,7,8,9,10,11, 17,18,19] (Suppl. 1). From 2 generations of the Framingham Heart Study, Bhole et al. found that individuals with higher SU are at a higher future risk of diabetes type II independent of other known risk factors [6]. The results were consistent with subgroup analysis by sex and hypertension status. In contrast, it was found that higher SU levels were inversely associated with diabetes type II in a representative sample of adults [11].
Among all these studies, only a single-time SU was measured. This may not adequately reflect its longitudinal variation and cumulative burden. Therefore, to our knowledge, there is little information regarding how cumSU affects diabetes type II incidence. Summary measures of SU that capture both the duration and intensity could more accurately estimate the effects of these risk factors over several decades. As a result, we used cumSU to evaluate the association between SU and diabetes type II.
In our study, a higher cumSU grading significantly increased the risk of diabetes type II incidence. The result was consistent with subgroup analysis by sex and age. After total adjustment, the risk of diabetes type II increased with cumSU. The same trend was also found in a non-hypertension population, suggesting cumSU is an independent risk factor to diabetes type II. However, there was no correlation between baseline SU and new-onset diabetes type II. This means cumSU has higher prognostic ability than baseline UA.
We also found that elevation of one SD of cumSU was associated with increased risk of diabetes type II. Similarly, Juraschek et al. found that with each 1 mg/dL increase in SU, the hazard ratio of diabetes type II also increased [8]. Moreover, the association between SU and diabetes type II was stronger in women [20], which is consistent with our study. However, another study found multivariate adjusted HRs for the incidence of diabetes type II corresponding to a one SD increase in SU was more significantly increased in men than in women [21]. The reason needs to be further investigated.
The underlying role of SU in the deterioration of glucose metabolism is not clear. A possible explanation is that high SU levels regulate oxidative stress, inflammation, and enzymes associated with glucose and lipid metabolism primarily in the liver, adipose tissue, and skeletal muscle [22]. Through positive feedback, adipose tissue could produce and secrete additional SU through xanthine oxidoreductase [23]. Through altering glucose metabolism, hyperuricemia would decrease insulin sensitivity and lead to insulin resistance [5, 24]. In support of this, studies have shown that SU may be a true mediator of renal disease and progression, which correspondingly causes diabetes type II [25].
Our study has several major strengths. We first report the association of cumSU with diabetes type II. CumSU, in addition to single baseline SU, increases reliability due to sampling of additional time points. This parameter had never been correlated with disease outcome until now. Additionally, large sample size and a constant number of participants were other distinct advantages in this study.
Our investigation has several limitations. First, all participants came from the city of Tangshan and were employees or retirees of the Kailuan Group Company. This study population was not representative of the total Chinese population. Therefore, Chinese individuals with a different lifestyle or different mean education level were not adequately represented. Second, our study shows cumSU is more correlated with diabetes type II in women than in men, the association between cumSU and diabetes type II in the whole population may be underestimated due to the disproportionate ratio of women to men. Lastly, specific confounding variables like diet and antihyperuricemia medication were not analyzed.
In conclusion, higher cumSU increases the risk of diabetes type II. This association was stronger than that of single SU and the risk of diabetes type II. Therefore, when assessing the risk of diabetes type II, the role of cumSU should be taken into consideration, especially in women.
References
Richette P, Bardin T (2010) Gout. Lancet 375:318–328. https://doi.org/10.1016/s0140-6736(09)60883-7
Qin L, Yang Z, Gu H, Lu S, Shi Q, Xing Y, Li X, Li R, Ning G, Su Q (2014) Association between serum uric acid levels and cardiovascular disease in middle-aged and elderly Chinese individuals. BMC Cardiovasc Disord 14(1):26–28. https://doi.org/10.1186/1471-2261-14-26
Cicero AF, Salvi P, D’Addato S, Rosticci M, Borghi C, Brisighella Heart Study group (2014) Association between serum uric acid, hypertension, vascular stiffness and subclinical atherosclerosis: data from the brisighella heart study. J Hypertens 32(1):57–64. https://doi.org/10.1097/HJH.0b013e328365b916
Oda E, Kawai R, Sukumaran V, Watanabe K (2009) Uric acid is positively associated with metabolic syndrome but negatively associated with diabetes in Japanese men. Intern Med 48(20):1785–1791. https://doi.org/10.2169/internalmedicine.48.2426
Krishnan E, Pandya BJ, Chung L, Hariri A, Dabbous O (2012) Hyperuricemia in young adults and risk of insulin resistance, prediabetes, and diabetes: a 15-year follow-up study. Am J Epidemiol 176(2):108–116. https://doi.org/10.1093/aje/kws002
Bhole V, Choi JW, Kim SW, de Vera M, Choi H (2010) Serum uric acid levels and the risk of type 2 diabetes: a prospective study. Am J Med 123(10):957–961. https://doi.org/10.1016/j.amjmed.2010.03.027
Dehghan A, van Hoek M, Sijbrands EJ, Hofman A, Witteman JC (2008) High serum uric acid as a novel risk factor for type 2 diabetes. Diabetes Care 31(2):361–362. https://doi.org/10.2337/dc071276
Juraschek SP, McAdams-Demarco M, Miller ER, Gelber AC, Maynard JW, Pankow JS, Young H, Coresh J, Selvin E (2014) Temporal relationship between uric acid concentration and risk of diabetes in a community-based study population. Am J Epidemiol 179(6):684–691. https://doi.org/10.1093/aje/kwt320
Wang T, Bi Y, Xu M, Huang Y, Xu Y, Li X, Wang W, Ning G (2011) Serum uric acid associates with the incidence of type 2 diabetes in a prospective cohort of middle-aged and elderly Chinese. Endocrine 40(1):109–116. https://doi.org/10.1007/s12020-011-9449-2
Taniguchi Y, Hayashi T, Tsumura K, Endo G, Fujii S, Okada K (2001) Serum uric acid the risk for hypertension and type 2 diabetes in Japanese men: the Osaka Health Survey. J Hypertens 19(7):1209–1215. https://doi.org/10.1097/00004872-200107000-00005
Bandaru P, Shankar A (2011) Association between serum uric acid levels and diabetes mellitus. Int J Endocrinol 2011(18):604715. https://doi.org/10.1155/2011/604715
Wu S, Li Y, Jin C, Yang P, Li D, Li H, Shen C (2012) Intra-individual variability of high-sensitivity c-reactive protein in Chinese general population. Int J Cardiol 157(1):75–79. https://doi.org/10.1016/j.ijcard.2010.12.019
Zemaitis P, Liu K, Jacobs DR Jr, Cushman M, Durazo-Arvizu R, Shoham D, Palmas W, Cooper R, Kramer H (2014) Cumulative systolic bp and changes in urine albumin-to-creatinine ratios in nondiabetic participants of the multi-ethnic study of atherosclerosis. Clin J Am Soc Nephrol 9(11):1922–1929. https://doi.org/10.2215/CJN.02450314
Yu J, Dai L, Zhao Q, Liu X, Chen S, Wang A, Su Z, Wu S (2017) Association of cumulative exposure to resting heart rate with risk of stroke in general population: the Kailuan cohort study. J Stroke Cerebrovasc Dis 26(11):2501–2509. https://doi.org/10.1016/j.jstrokecerebrovasdis.2017.05.037
Wang A, Liu J, Li C, Gao J, Li X, Chen S, Wu S, Ding H, Fan H, Hou S (2017) Cumulative exposure to high-sensitivity c-reactive protein predicts the risk of cardiovascular disease. J Am Heart Assoc 6(10):e005610. https://doi.org/10.1161/JAHA.117.005610
Liu X, Cui L, Wang A, Wang X, Song Q, Li S, Shi J, Zhao X, Chen S, Du X, Ji C, Huxley R, Guo Y, Wu S (2016) Cumulative exposure to ideal cardiovascular health and incident diabetes in a Chinese population: the Kailuan study. J Am Heart Assoc 5(9):e004132. https://doi.org/10.1161/JAHA.116.004132
Viazzi F, Leoncini G, Vercelli M, Deferrari G, Pontremoli R (2011) Serum uric acid levels predict new-onset type 2 diabetes in hospitalized patients with primary hypertension: the magic study. Diabetes Care 34(1):126–128. https://doi.org/10.2337/dc10-0918
Krishnan E, Akhras KS, Sharma H, Marynchenko M, Wu EQ, Tawk R, Liu J, Shi L (2013) Relative and attributable diabetes risk associated with hyperuricemia in us veterans with gout. QJM 106(8):721–729. https://doi.org/10.1093/qjmed/hct093
Kodama S, Saito K, Yachi Y, Asumi M, Sugawara A, Totsuka K, Saito A, Sone H (2009) Association between serum uric acid and development of type 2 diabetes. Diabetes Care 32(9):1737–1742. https://doi.org/10.2337/dc09-0288
Kivity S, Kopel E, Steinlauf S, Segev S, Sidi Y, Olchovsky D (2013) The association between serum uric acid and diabetes mellitus is stronger in women. J Women’s Health (Larchmt) 22(9):782–789. https://doi.org/10.1089/jwh.2012.4043
Nan H, Qiao Q, Söderberg S, Pitkäniemi J, Zimmet P, Shaw J, Alberti G, Uusitalo U, Pauvaday V, Chitson P, Tuomilehto J (2008) Serum uric acid and incident diabetes in Mauritian Indian and Creole populations. Diabetes Res Clin Pract 80(2):321–327. https://doi.org/10.1016/j.diabres.2008.01.002
Lima WG, Martins-Santos ME, Chaves VE (2015) Uric acid as a modulator of glucose and lipid metabolism. Biochimie 116:17–23. https://doi.org/10.1016/j.biochi.2015.06.025
Tsushima Y, Nishizawa H, Tochino Y, Nakatsuji H, Sekimoto R, Nagao H, Shirakura T, Kato K, Imaizumi K, Takahashi H, Tamura M, Maeda N, Funahashi T, Shimomura I (2013) Uric acid secretion from adipose tissue and its increase in obesity. J Biol Chem 288(38):27138–27149. https://doi.org/10.1074/jbc.M113.485094
Fabbrini E, Serafini M, Colic Baric I, Samuel (2014) Effect of plasma uric acid on antioxidant capacity, oxidative stress, and insulin sensitivity in obese subjects. Diabetes 63(3):976–981. https://doi.org/10.2337/db13-1396
Kang DH, Nakagawa T, Feng L, Watanabe S, Han L, Mazzali M, Truong L, Harris R, Johnson RJ (2002) A role for uric acid in the progression of renal disease. J Am Soc Nephrol 13(12):2888–2897. https://doi.org/10.1097/01
Acknowledgments
We are grateful to the participants that were recruited in this study for their essential contribution.
Contributors
YH, YL, XL, WY, YW, and PY participated in the study design, drafting of the manuscript, data collection, and statistical analysis. JW, YH, RS, HS, JW, WY, BL, NL, HS, WY, LL, and YH participated in data collection and statistical analysis. LC designed the study and gave final approval for the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The study was approved by the Ethics Committees of Kailuan General Hospital following the guidelines outlined by the Helsinki Declaration. All subjects agreed to participate in this study and provided written informed consent.
Disclosures
None.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 35 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Han, Y., Liu, Y., Liu, X. et al. Association between cumulative serum urate and development of diabetes type II: the Kailuan Study. Clin Rheumatol 39, 339–346 (2020). https://doi.org/10.1007/s10067-019-04790-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-019-04790-0