
Abstract
Introduction
Level 1 data suggest that mesh reinforcement of the crural closure for hiatal hernia repair decreases the recurrence of hernia. The fear of erosion of the prosthetic into the esophagus has kept the use of mesh for hiatal hernia repair from becoming routine. A recent study found several cases of esophageal stenosis/erosion from the use of a biologic mesh. For these reasons, we evaluated a new resorptive prosthetic and new method of fixation of the prosthetic for crural reinforcement during hiatal hernia repair.
Methods
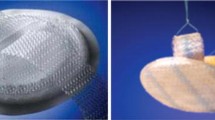
From February 2009 until December 2010, 70 patients underwent hiatal hernia repair using a synthetic bioabsorbable prosthetic made of polglycolide and teimethylene carbonate (Gore BioA Tissue Reinforcement™, Flagstaff, AZ). There were 48 patients with paraesophageal hiatal hernias and 22 with large sliding hiatal hernias. In this study, a square piece of mesh just the size to cover the crural closure only was utilized. Fibrin glue (Tisseel™) was applied over the suture closure of the crura, the mesh was then placed over the glue and held in place for several seconds, and then more fibrin glue was applied on top of the mesh.
Results
The new bioabsorbable polymer mesh was readily placed through a 10-mm trocar, had good handling characteristics laparoscopically, and no pre-operative preparation was required of the prosthetic. The material and the fibrin glue created a very substantial reinforcement of the crural closure, and the average time to place and fix the mesh was approximately 5 min. There were no short-term complications from the mesh, and no patient has had any significant post-operative sequelae.
Conclusion
Crural closure reinforcement during hiatal hernia repair can be done readily with this new bioabsorbable polymer–based mesh. Fibrin glue fixation of this new prosthetic can be done quickly and it creates a strong, fixed barrier that may decrease the chance of erosion. Further studies will need to be done to evaluate long-term efficacy and complications associated with its use.


Similar content being viewed by others


References
Hashemi M, Peters JH, DeMeester TR, Huprich JE, Quek M, Hagen JA, Crookes PF, Theisen J, DeMeester SR, Sillin LF, Bremner CG (2000) Laparoscopic repair of large type III hiatal hernia: objective followup reveals high recurrence rate. J Am Coll Surg 190(5):553–560
Soricelli E, Basso N, Genco A, Cipriano M (2009) Long-term results of hiatal hernia mesh repair and antireflux laparoscopic surgery. Surg Endosc, Apr 3
Lee E, Frisella MM, Matthews BD, Brunt LM (2007) Evaluation of acellular human dermis reinforcement of the crural closure in patients with difficult hiatal hernias. Surg Endosc 21(4):641–645
Frantzides CT, Madan AK, Carlson MA, Stavropoulos GP (2002) A prospective, randomized trial of laparoscopic polytetrafluoroethylene (PTFE) patch repair vs simple cruroplasty for large hiatal hernia. Arch Surg 137(6):649–652
Morino M, Giaccone C, Pellegrino L, Rebecchi F (2006) Laparoscopic management of giant hiatal hernia: factors influencing long-term outcome. Surg Endosc 20(7):1011–1016
Oelschlager BK, Pellegrini CA, Hunter J, Soper N, Brunt M, Sheppard B, Jobe B, Polissar N, Mitsumori L, Nelson J, Swanstrom L (2006) Biologic prosthesis reduces recurrence after laparoscopic paraesophageal hernia repair: a multicenter, prospective, randomized trial. Ann Surg 244(4):481–490
Stadlhuber RJ, Sherif AE, Mittal SK, Fitzgibbons RJ Jr, Michael Brunt L, Hunter JG, Demeester TR, Swanstrom LL, Daniel Smith C, Filipi CJ (2009) Mesh complications after prosthetic reinforcement of hiatal closure: a 28-case series. Surg Endosc 23(6):1219–1226
Horgan S, Pohl D, Bogetti D, Eubanks T, Pellegrini C (1999) Failed antireflux surgery: what have we learned from reoperations? Arch Surg 134(8):809–815; Discussion 815–817
Hainaux B, Sattari A, Coppens E, Sadeghi N, Cadière GB (2002) Intrathoracic migration of the wrap after laparoscopic Nissen fundoplication: radiologic evaluation. AJR Am J Roentgenol 178(4):859–862
Granderath FA, Schweiger UM, Kamolz T, Asche KU, Pointner R (2005) Laparoscopic Nissen fundoplication with prosthetic hiatal closure reduces postoperative intrathoracic wrap herniation: preliminary results of a prospective randomized functional and clinical study. Arch Surg 140(1):40–48
Johnson JM, Carbonell AM, Carmody BJ, Jamal MK, Maher JW, Kellum JM, DeMaria EJ (2006) Laparoscopic mesh hiatoplasty for paraesophageal hernias and fundoplications: a critical analysis of the available literature. Surg Endosc 20(3):362–366 (review). Epub 2006 Jan 25
Tatum RP, Shalhub S, Oelschlager BK, Pellegrini CA (2008) Complications of PTFE mesh at the diaphragmatic hiatus. J Gastrointest Surg 12(5):953–957. Epub 2007 Sep 18
Griffith PS, Valenti V, Qurashi K, Martinez-Isla A (2008) Rejection of goretex mesh used in prosthetic cruroplasty: a case series. Int J Surg 6(2):106–109
Frantzides CT, Carlson MA, Loizides S, Papafili A, Luu M, Roberts J, Zeni T, Frantzides A (2010) Hiatal hernia repair with mesh: a survey of SAGES members. Surg Endosc 24(5):1017–1024. Epub 2009 Dec 8
Fortelny RH, Petter-Puchner AH, Glaser KS (2009) Fibrin sealant (Tissucol™) for the fixation of hiatal mesh in the repair of giant paraesophageal hernia: a case report. Surg Laparosc Endosc Percutan Tech 19(3):e91–e94
Zehetner J, Lipham JC, Ayazi S, Oezcelik A, Abate E, Chen W, Demeester SR, Sohn HJ, Banki F, Hagen JA, Dickey M, Demeester TR (2010) A simplified technique for intrathoracic stomach repair: laparoscopic fundoplication with Vicryl mesh and BioGlue crural reinforcement. Surg Endosc 24(3):675–679. Epub 2009 Aug 19
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Powell, B.S., Wandrey, D. & Voeller, G.R. A technique for placement of a bioabsorbable prosthesis with fibrin glue fixation for reinforcement of the crural closure during hiatal hernia repair. Hernia 17, 81–84 (2013). https://doi.org/10.1007/s10029-012-0915-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10029-012-0915-4