
Abstract
Objective
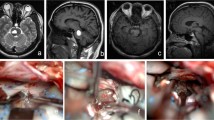
Pontine cavernomas are benign vascular lesions whose surgical treatment is challenging due to their localization. We report our experience in the surgical management of these lesions exclusively using a lateral, subtemporal transtentorial approach in high pontine lesions and an anterior petrosal approach in low pontine lesions.
Methods
We performed a retrospective study on a series of patients who were operated on for a pontine cavernoma in our neurosurgery department between 1987 and 2007. In the study, we detail the patients' clinical and preoperative radiological data and compare the two surgical techniques we used. Finally, we analyze the postoperative follow-up, the morbidity encountered according to the surgical approach used, and the long-term outcomes.
Results
We enrolled nine patients into the study. Six patients were operated on using an anterior petrosal approach. None of the patients died. Five patients were able to resume their former professional activity after surgery and were clearly improved following surgery. One patient was worse after surgery (hemiplegia and deafness). We used a subtemporal transtentorial approach in three of the patients. None of the patients died. Two of the patients were able to resume their prior professional activities without any sequels, and the third patient's condition worsened following surgery (temporal hematoma).
Conclusion
The lateral surgical approach for pontine cavernomas constitutes a reasonable surgical alternative to the transventricular, suboccipital, retromastoid, or transclival approaches. Patient morbidity in both approaches is acceptable, and the long-term outcome is satisfactory with respect to sequels and the resumption of prior professional activity.




Similar content being viewed by others


References
Amin-Hanjani S, Ogilvy CS, Candia GJ, Lyons S, Chapman PH (1998) Stereotactic radiosurgery for cavernous malformations: Kjellberg's experience with proton beam therapy in 98 cases at the Harvard Cyclotron. Neurosurgery 42:1229–1236
Ardeshiri A, Ardeshiri A, Wenger E, Holtmannspötter M, Winkler PA (2006) Subtemporal approach to the tentorial incisura: normative morphometric data based on magnetic resonance imaging scans. Neurosurgery 58:ONS22-8
Bogucki J, Czernicki Z, Gielecki J (2000) Cytoarchitectonic basis for safe entry into the brainstem. Acta Neurochir (Wien) 142:383–387
Cantore G, Missori P, Santoro A (1999) Cavernous angiomas of the brain stem. Intra-axial anatomical pitfalls and surgical strategies. Surg Neurol 52:84–93
Cenzato M, Stefini R, Ambrosi C, Giovanelli M (2008) Post-operative remnants of brainstem cavernomas: incidence, risk factors and management. Acta Neurochir (Wien) 150:879–886
Ciurea AV, Nastase C, Tascu A, Brehar FM (2007) Lethal recurrent hemorrhages of a brainstem cavernoma. Neurosurg Rev 30:259–262
Ferroli P, Sinisi M, Franzini A, Giombini S, Solero CL, Broggi G (2005) Brainstem cavernomas: long-term results of microsurgical resection in 52 patients. Neurosurgery 56:1203–1212
Figueiredo EG, Zabramski JM, Deshmukh P, Crawford NR, Spetzler RF, Preul MC (2006) Comparative analysis of anterior petrosectomy and transcavernous approaches to retrosellar and upper clival basilar artery aneurysms. Neurosurgery 58:ONS13-21
Fox JL (1967) Obliteration of midline vertebral artery aneurysm via basilar craniectomy. J Neurosurg 26:406–412
Fritschi JA, Reulen HJ, Spetzler RF, Zabramski JM (1994) Cavernous malformations of the brain stem. A review of 139 cases. Acta Neurochir (Wien) 130:35–46
Hasegawa T, McInerney J, Kondziolka D, Lee JY, Flickinger JC, Lunsford LD (2002) Long-term results after stereotactic radiosurgery for patients with cavernous malformations. Neurosurgery 50:1190–1197
Hauck EF, Barnett SL, White JA, Samson D (2009) Symptomatic brainstem cavernomas. Neurosurgery 64:61–70
House WF, Hitselberger WE, Horn KL (1986) The middle fossa transpetrous approach to the anterior-superior cerebellopontine angle. Am J Otol 7:1–4
Kashimura H, Inoue T, Ogasawara K, Ogawa A (2006) Pontine cavernous angioma resected using the subtemporal, anterior transpetrosal approach determined using three-dimensional anisotropy contrast imaging: technical case report. Neurosurgery 58:ONS-E175
Kawase T, Toya S, Shiobara R, Mine T (1985) Transpetrosal approach for aneurysms of the lower basilar artery. J Neurosurg 63:857–861
Kim MS, Pyo SY, Jeong YG, Lee SI, Jung YT, Sim JH (2005) Gamma knife surgery for intracranial cavernous hemangioma. J Neurosurg 102:102–106
Kondziolka D, Lunsford LD, Kestle JR (1995) The natural history of cerebral cavernous malformations. J Neurosurg 83:820–824
Kupersmith MJ, Kalish H, Epstein F, Yu G, Berenstein A, Woo H, Jafar J, Mandel G, De Lara F (2001) Natural history of brainstem cavernous malformations. Neurosurgery 48:47–53
Kyoshima K, Kobayashi S, Gibo H, Kuroyanagi T (1993) A study of safe entry zones via the floor of the fourth ventricle for brain-stem lesions. Report of three cases. J Neurosurg 78:987–993
Liscák R, Vladyka V, Simonová G, Vymazal J, Novotny J Jr (2005) Gamma knife surgery of brain cavernous hemangiomas. J Neurosurg 102:207–213
Mathiesen T, Edner G, Kihlström L (2003) Deep and brainstem cavernomas: a consecutive 8-year series. J Neurosurg 99:31–37
Moriarity JL, Clatterbuck RE, Rigamonti D (1999) The natural history of cavernous malformations. Neurosurg Clin N Am 10:411–417
Moriarity JL, Wetzel M, Clatterbuck RE, Javedan S, Sheppard JM, Hoenig-Rigamonti K, Crone NE, Breiter SN, Lee RR, Rigamonti D (1999) The natural history of cavernous malformations: a prospective study of 68 patients. Neurosurgery 44:1166–1671
Oiwa Y, Nakai K, Masaki Y, Masuo O, Kuwata T, Moriwaki H, Itakura T (2002) Presigmoid approach for cavernous angioma in the pons—technical note. Neurol Med Chir (Tokyo) 42:91–96
Pollock BE, Garces YI, Stafford SL, Foote RL, Schomberg PJ, Link MJ (2000) Stereotactic radiosurgery for cavernous malformations. J Neurosurg 93:987–991
Porter RW, Detwiler PW, Spetzler RF, Lawton MT, Baskin JJ, Derksen PT, Zabramski JM (1999) Cavernous malformations of the brainstem: experience with 100 patients. J Neurosurg 90:50–58
Porter PJ, Willinsky RA, Harper W, Wallace MC (1997) Cerebral cavernous malformations: natural history and prognosis after clinical deterioration with or without hemorrhage. J Neurosurg 87:190–197
Reisch R, Bettag M, Perneczky A (2001) Transoral transclival removal of anteriorly placed cavernous malformations of the brainstem. Surg Neurol 56:106–115
Rohde V, Berns E, Rohde I, Gilsbach JM, Ryang YM (2007) Experiences in the management of brainstem hematomas. Neurosurg Rev 30:219–223
Saito N, Sasaki T, Chikui E, Yuyama R, Kirino T (2002) Anterior transpetrosal approach for pontine cavernous angioma—case report. Neurol Med Chir (Tokyo) 42:272–274
Samii M, Eghbal R, Carvalho GA, Matthies C (2001) Surgical management of brainstem cavernomas. J Neurosurg 95:825–832
Steiger HJ, Hänggi D, Stummer W, Winkler PA (2006) Custom-tailored transdural anterior transpetrosal approach to ventral pons and retroclival regions. J Neurosurg 104:38–46
Stevenson GC, Stoney RJ, Perkins RK, Adams JE (1966) A transcervical transclival approach to the ventral surface of the brain stem for removal of a clivus chordoma. J Neurosurg 24:544–551
Velut S, Jan M (1988) Petrectomy of the point during approach to the clivus: technic, values and limitations. A propos of a case of meningioma. Neurochirurgie 34:17–25
Wang CC, Liu A, Zhang JT, Sun B, Zhao YL (2003) Surgical management of brain-stem cavernous malformations: report of 137 cases. Surg Neurol 59:444–454
Yaşargil MG, Reichman MV, Kubik S (1987) Preservation of the frontotemporal branch of the facial nerve using the interfascial temporalis flap for pterional craniotomy. Technical article. J Neurosurg 67:463–466
Author information
Authors and Affiliations
Corresponding author
Additional information
Comments
The authors describe the use of the subtemporal transtentorial and anterior petrosectomy approaches to pontine cavernomas in nine patients treated at their institution over a 20-year period. Six patients were operated upon using the anterior transpetrosal approach; three underwent the subtemporal transtentorial approach. They achieved reasonable outcomes for patients in the series. The points that the authors make are valid regarding the discussion of the advantage of these approaches.
They provide a nice discussion of the alternative approaches (trans fourth ventricle: suboccipital and anterior transclival) to these pontine lesions. They describe their indications for both the subtemporal transtentorial and the anterior transpetrosal approach.
For many of the mid to lower lesions of the pons (such as in Fig. 2), many surgeons would alternatively choose a retrosigmoid or posterior petrosal approach. I have also personally used a far-lateral transcondylar approach to a lesion in the anterior and most inferior belly of the pons, which enables nice access from an inferior to superior trajectory in between the sixth nerves as the exit the pons.
The authors are to be commended for their nice description of the use of these approaches to this difficult anatomical area.
W.T. Couldwell
Utah, USA
Rights and permissions
About this article
Cite this article
François, P., Ben Ismail, M., Hamel, O. et al. Anterior transpetrosal and subtemporal transtentorial approaches for pontine cavernomas. Acta Neurochir 152, 1321–1329 (2010). https://doi.org/10.1007/s00701-010-0667-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-010-0667-9