
Abstract
Purpose
We investigated the communication bandwidth (CB) limitation for remote robotics surgery (RRS) using hinotori™ (Medicaroid, Kobe, Japan).
Methods
The operating rooms of the Hokkaido University Hospital and Kyushu University Hospital were connected using the Science Information NETwork (SINET). The minimum required CB for the RRS was verified by decreasing the CB from 500 to 100 Mbps. Ten surgeons were tested on a task (intracorporeal suturing) at different levels of video compression (VC) (VC1: 120 Mbps, VC2: 40 Mbps, VC3: 20 Mbps) with the minimum required CB, and assessed based on the task completion time, Global Evaluative Assessment of Robotic Skills (GEARS), and System and Piper Fatigue Scale-12 (PFS-12).
Results
Packet loss was observed at 3–7% and image degradation was observed at 145 Mbps CB. The task performance with VC1 was significantly worse than that with VC2 and VC3 according to the task completion time (VC1 vs VC2, P = 0.032; VC1 vs. VC3, P = 0.032), GEARS (VC1 vs VC2; P = 0.029, VC1 vs VC3; P = 0.031), and PFS-12 (VC1 vs. VC2; P = 0.032, VC1 vs. VC3; P = 0.032) with 145 Mbps.
Conclusion
Our findings provide evidence that RRS using hinotori™ requires a CB ≥ 150 Mbps. We also found that when there is insufficient CB, RRS can be continued by compressing the image.
Similar content being viewed by others

Introduction
In recent years, the development of high-speed, high-capacity communication technology using optical fiber and 5th generation mobile communication systems (5G), together with new surgical robots, has made remote surgery a reality [1]. One of the advantages of remote robotics surgery (RRS) is that it can reduce the physical, mental, and financial burden on patients and surgeons by reducing the need for travel. However, there are still many problems to overcome to implement RRS in society, one of which is the establishment of a stable communication environment. Communication delays or significant packet loss during surgery leads to the distribution of images and inadequate robot functioning, which are major obstacles to safe surgery [2,3,4,5]. To avoid this, it is essential to identify the communication bandwidth (CB) required for safe and stable telecommunication according to the amount of video data and operation data for each surgical robot. The purpose of this study was to identify the required CB for RRS using hinotori™, a novel surgical robot made in Japan. Setting the required CB is essential to ensure future implementation.
Materials and methods
The minimum required CB for RRS using hinotori™ was verified by gradually decreasing the CB from 500 to 100Mbps. We measured the communication round-trip time (RTT; the time in milliseconds from the time the switch on the surgeon cockpit side sends a request to the time the response is received from the switch on the operation unit side), jitter (variation in latency of packet flow), and packet loss (the fraction of the total transmitted packets that did not arrive at the receiver) for each CB. Ten skilled surgeons, including five gastroenterological surgeons, two urologists, two gynecologists, and one thoracic surgeon, participated in this experiment. All had sufficient experience in laparoscopic surgery and robotic surgery.
After we found the minimum required bandwidth, the participants were tested on a standard task (intracorporeal suturing) based on the Fundamentals of Laparoscopic Surgery (FLS) curriculum [6] using different levels of video compression (VC); that is, the process of reducing the total number of bits needed to represent a given image or video sequence (VC1: 120 Mbps, VC2: 40 Mbps, VC3: 20 Mbps) with the minimum required bandwidth. We measured the RTT, jitter, packet loss for the VC, task completion time, and robotic surgical skill using the Global Evaluative Assessment of Robotic Skills (GEARS). Subjective evaluation of the surgeon was validated using the System and Piper Fatigue Scale-12 (PFS-12).
Network connections
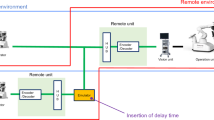
The operating rooms of Hokkaido University Hospital and Kyushu University Hospital were connected by SINET5 (Science Information NETwork) [7] (Fig. 1). SINET5 is a non-commercial science information network designed and operated by the National Institute of Informatics, and provides a nation-wide 100-Gbps backbone for about 1000 universities and research institutes throughout Japan. For this investigation, a virtual private communication circuit was established between the two hospitals alongside the Japan Sea, with a circuit distance of about 2000 km on a map basis and about 2600 km on an optical-fiber-length basis. The CBs of the circuit were set up in the range of 500–100 Mbps by specifying the rate limits so as to drop information packets if the usage rate of the circuit exceeded the specified rate limit. Communication information was compressed and decompressed using an encoder and decoder evaluated by Medicaroid (Medicaroid Corporation, Kobe, Japan). The encoders and decoders in this study use H.265 [8], which is a high compression technology that enables ultra-short delay video transmission and has been applied to ultra-short delay live broadcasting. A raw video is a sequence of images, and its size makes it impractical to store or transfer. VC takes advantage of the fact that the frames in a video sequence are highly correlated in time and reduces spatial and temporal redundancy, so that as few bits as possible are used to represent the video sequence. Modern standard video compression algorithms such as H.265 are psycho-visually optimized and compress the video data in such a way that quality and detail reduction are realistically invisible to human perception. To evaluate the communication delay during RRS, we measured the RTT of the network line and the packet loss of image signals. RTT is composed of communication line delay (SINET) (Fig. 2).

Schema of network connection for remote robotic surgery. The operating rooms at Hokkaido University Hospital and Kyushu University Hospital (network communication distance of nearly 2,000 km) were connected by SINET. SINET Science Information NETwork, HUH Hokkaido University Hospital, KUH Kyushu University Hospital

Network system. The round-trip time (RTT) is composed of communication line delay (SINET). SINET Science Information NETwork
Robot system
We used the hinotori™ surgical robot system (Medicaroid Corporation, Kobe, Japan), the first made-in-Japan robotic system, which received regulatory approval from the Japanese Ministry of Health, Labor, and Welfare in August, 2020. A Karl Storz™ 3D endoscope system (Karl Storz, Tuttlingen, Germany) was installed in the system.
Task: intracorporeal suturing
At least three throws of the suture were made, including one double throw and two single throws. The time was measured from when the instrument appeared on the monitor until when the suture material and needle were cut. The task completion time and results of the technical evaluation using GEARS were recorded [9]. The technical evaluation was conducted by two physicians certified in the endoscopic surgical skill qualification system of the Japan Society for Endoscopic Surgery (JSES) [10]. The subjective evaluation of the surgeon was validated using PFS-12 [11].
Statistical analysis
Each test score was compared between groups using the Mann–Whitney U test for continuous variables. Statistical significance was set at P < 0.05. Statistical analysis was performed using the JMP® 15 software (SAS Institute Inc., Cary, NC, USA).
Results
Minimum required CB for RRS using the hinotori™
Figure 3 shows an example of the network communication delay, packet loss, and jitter for each CB (500–300–200–150–145 Mbps). Ten surgeons attempted a simple task such as ring movement in each CB. At 145 Mbps CB, the packet loss was noticeable (3.0–7.0%) and image degradation was observed (Fig. 4). However, the RTT and jitter did not change (RTT, 30–30.4 ms; jitter, 0–0.35 ms).

The packet loss and jitter for communication bandwidths of 500 Mbps, 300 Mbps, 200 Mbps, 150 Mbps, and 145 Mbps. At 145 Mbps, the packet loss was noticeable (3–7%), but the round-trip time (RTT) and jitter did not change (RTT, 30–30.4 ms; jitter, 0–0.35 ms)

Operation image from 145 Mbps communication bandwidth. At 145 Mbps, image degradation was observed
Completing the task: intracorporeal suturing
Five surgeons attempted simulation of intracorporeal suturing with a CB of 145 Mbps, which was revealed to be the minimum required CB for the robot system in the former experiment. Concerning changes in network communication delay in VC2 and VC3, the RTT and jitter did not change (RTT, 30–31.5 ms; jitter, 0–0.6 ms), and no packet loss was observed (Fig. 5). The total amount of communication data, including the robot control signal, under a CB of 145 Mbps was 130–155 Mbps for VC1, 50–65 Mbps for VC2, and 35–40 Mbps for VC3 (Fig. 6). The intracorporeal suturing completion time was significantly longer in VC1 than in VC2 or VC3, at 667.4 ± 56.4 s, 275.8 ± 73.9 s, and 236.4 ± 42.5 s, respectively (VC1 vs. VC2, P = 0.009; VC1 vs. VC3, P = 0.009; VC2 vs. VC3, P = 0.209; Fig. 7a). The GEARS score was significantly lower in VC1 than in VC2 or VC3, at 17.4 ± 1.7, 26.6 ± 3.4, and 27.2 ± 1.5, respectively; (VC1 vs. VC2, P = 0.008; VC1 vs. VC3, P = 0.009; VC2 vs. VC3, P = 0.829; Fig. 7b). The PFS-12 score was significantly higher in VC1 than in VC2 or VC3, at 98.8 ± 18.1, 34.4 ± 20.5, and 33.2 ± 28.1, respectively (VC1 vs. VC2, P = 0.009; VC1 vs. VC3, P = 0.009; VC2 vs. VC3, P = 0.917; Fig. 7c).

Comparison of round-trip time (RTT), packet loss, and jitter depending on the video compression (VC) amount. At VC 1 (120 Mbps), packet loss was between 3 and 7%. At VC 2 (40 Mbps) and VC 3 (20 Mbps), packet loss was not observed. RTT and jitter showed no changes (RTT, 30–31.5 ms, jitter, 0–1.0 ms) for all VC

Total amount of communication data under communication bandwidth of 145 Mbps. The total amount of communication data (including the robot control signal) was 130–155 Mbps at video compression (VC) 1 (120 Mbps), 50–65 Mbps at VC 2 (40 Mbps), and 35–40 Mbps at VC 3 (20 Mbps)

Intracorporeal suturing completion time and robotic skill evaluation using the Global Evaluative Assessment of Robotic Skills (GEARS). The subjective evaluation of the surgeon was validated using the System and Piper Fatigue Scale-12 (PFS-12). a Intracorporeal suturing completion time: VC1 significantly prolonged the task completion time versus that with VC2 and VC3 (P = 0.009 and P = 0.009, respectively). b GEARS scores with VC1 were significantly lower than those with VC2 and VC3 (P = 0.008 and P = 0.009, respectively). c PFS-12 scores with VC1 were significantly higher than those with VC2 and VC3 (P = 0.009 and P = 0.009, respectively). VC: video compression (VC1, 120 Mbps; VC2, 40 Mbps; VC3, 20 Mbps)
Discussion
For this study, we set up the Japanese-made surgical robot system, hinotori™, in an operating room 2000 km away from the operator, to investigate the feasibility of RRS and confirmed the robot’s behavior in an environment where surgery is possible. Through this SINET connection verification, we confirmed that there was no recognizable communication delay or image degradation at a CB of more than 150 Mbps. Our findings also suggested that image degradation could be avoided by considering the amount of VC, even when the available CB is insufficient.
Telemedicine has become an inevitable trend through the development of modern medical technology. Teleconsultation, telediagnosis, mobile wards, remote patient image sharing, remote emergency treatment, image sharing and emergency treatment for stroke, digital operating rooms, and distance education have made considerable progress [12,13,14,15,16,17]. The development of RRS has been especially remarkable. Using the ZEUS robotic system and the Transatlantic Optical Faber Network, Jack Marescaux [18, 19] performed the first remote cholecystectomy clinically. This procedure, also known as Lindbergh surgery, is considered a milestone in telesurgery, following which 22 telesurgeries were performed at a hospital in North Bay, approximately 400 km north of Hamilton, Canada [20]. Although both surgeries were successful, the transatlantic connection used an expensive dedicated line (10 Mbps CB), whereas the Canadian clinical case used an Internet Protocol-Virtual Private Network line, a special inter-hospital network developed by the government (15 Mbps CB). In USA, Florida Hospital has successfully performed robot-assisted remote surgery using the Internet. Surgeons in Texas, 1200 miles away from Florida, remotely controlled a da Vinci robot to operate on a simulated patient via the Internet [21]. In Japan, robotic telesurgical simulation for training was first reported by Hashizume et al. [22]. Consequently, the underdeveloped information and communication technology was a decisive factor that led to a long hiatus in telesurgery research [23]. The recent development of high-speed, high-capacity communication technology using optical fiber and 5G, with new surgical robots, is making remote surgery a reality [24]. The bandwidths of the optical fiber and 5G network were 1 Gbps, which is comparable to the bearing capacity of the Internet and 100 times wider than that of the satellite network [1]. It is expected that robotic surgery using the Internet will develop further with the evolution of technology.
Despite this promising outlook, there are problems with RRS that need to be solved, one of which is the establishment of a stable communication environment. Communication delays during RRS can be a major obstacle to safe surgical procedures [2,3,4,5]. It has been reported that operability decreases when the transmission delay time perceived by the surgeon exceeds 200 ms, that errors increase when the delay time exceeds 300 ms [25, 26], and that surgery becomes almost impossible when the delay time exceeds 700 ms [27]. Many reports suggest that the delay time should be less than 200 ms, and ideally less than 100 ms, for a successful robot operation to be completed normally [28, 29].
In this study, it was possible to operate with minimal delay (< 30 ms) at all CBs; however, image degradation was observed at 145 Mbps CB. When robot control signals and audio signals were included in addition to the image signals, the traffic from all the signals exceeded 145 Mbps, and image degradation was observed. Because of the degraded images, the task completion time increased and the surgeon became more fatigued. The reason why image degradation rather than image delay occurred when reducing the CB was thought to be the adoption of traffic policing, which cuts off some of the traffic that exceeds the rate limit on SINET lines. At 145 Mbps, by changing the VC amount (VC 2: 40 Mbps, VC 3: 20 Mbps), image degradation disappeared at the same CB and we could not discern any decrease in image quality. In addition to image degradation, information and communication processing technology to compress and decompress transmission data are also important. The largest volume of transmission signals in the RRS is the video signal, which is strongly affected by the CB. Therefore, information and compression processing technologies are essential; however, the compression and decompression processes also cause delays. Because there is a trade-off between the compression ratio and time required for compression and decompression, it is necessary to develop encoders and decoders that achieve high compression and low delay. In this study, excessive image capacity load might cause image degradation, and the amount of VC needed to be adjusted as a countermeasure.
In this study, despite the long communication distance of approximately a 4000 km round-trip, we were able to communicate 3D 2 K images without image degradation with an RTT of 30 ms, which hardly affected the surgeon’s performance. Furthermore, even with a CB of 145 Mbps, we were able to perform the task without any image degradation or delay, using image compression technology. In the future, the limitations of CB may be overcome by the development of encoders, decoders, and 5G communication technologies that enable low-latency transmission of high-precision images, such as 8 K and 16 K.
In this study, we demonstrated that hinotori™ can be used in commercial communications by selecting a bandwidth type of service of more than 150 Mbps. Currently, there are two types of commercial communication networks, open and closed networks, which differ in their degree of security assurance, communication quality, and cost. In RRS, it is important to select a communication network based on the premise of sufficient communication quality and security, while considering economic efficiency. For future clinical applications of RRS, it would be desirable to develop guidelines for optimal communication systems focusing on safety, ethics, and costs.
In recent years, 5G communication technology has been reported to have advantages such as high speed and large capacity communication, high mobility, multiple connections, and wide bandwidth, which will be beneficial for robots that require a wide bandwidth for high-quality transmission, such as 4 K/8 K video [1]. The advantages of a 5G network over a 4G network also include wider bandwidth and lower latency time and, unlike the wired Internet, the 5G wireless network has high mobility and eliminates the regional restriction of special network cables. Therefore, it is expected that RSS will be realized in isolated islands and disaster areas, where it is difficult to lay wired Internet cables. Moreover, surgeries performed during the coronavirus disease pandemic era need to avoid infection crises from the flow of people. In this situation, RSS using 5G will support remote surgeries in regional hospitals throughout Japan and help train young surgeons.
This study has several limitations. First, because of the limited duration of the experiment, the number of tasks was small and the time to practice the robot operation was short. Second, the image quality was evaluated based on the surgeon’s impression, and no objective data analysis was conducted. In the future, remote surgery using high-precision images will be possible, and a universal image evaluation method will be necessary.
Conclusion
RRS using the novel hinotori™ surgical robot system can be performed safely if the CB is ≥ 150 Mbps. RRS can be implemented in society using currently available commercial communication networks.
References
Zheng J, Wang Y, Zhang J, Guo W, Yang X, Luo L, et al. 5G ultra-remote robot-assisted laparoscopic surgery in China. Surg Endosc. 2020;34(11):5172–80. https://doi.org/10.1007/s00464-020-07823-x (PMID: 32700149).
Sterbis JR, Hanly EJ, Herman BC, Marohn MR, Broderick TJ, Shih SP, et al. Transcontinental telesurgical nephrectomy using the da Vinci robot in a porcine model. Urology. 2008;71(5):971–3. https://doi.org/10.1016/j.urology.2007.11.027 (PMID: 18295861).
Nguan C, Miller B, Patel R, Luke PP, Schlachta CM. Pre-clinical remote telesurgery trial of a da Vinci telesurgery prototype. Int J Med Robot. 2008;4(4):304–9. https://doi.org/10.1002/rcs.210 (PMID: 18803341).
Raison N, Khan MS, Challacombe B. Telemedicine in surgery: what are the opportunities and hurdles to realising the potential? Curr Urol Rep. 2015;16(7):43. https://doi.org/10.1007/s11934-015-0522-x (PMID: 26025497).
Korte C, Nair SS, Nistor V, Low TP, Doarn CR, Schaffner G. Determining the threshold of time-delay for teleoperation accuracy and efficiency in relation to telesurgery. Telemed J E Health. 2014;20(12):1078–86. https://doi.org/10.1089/tmj.2013.0367 (PMID: 25290465).
Okrainec A, Soper NJ, Swanstrom LL, Fried GM. Trends and results of the first 5 years of Fundamentals of Laparoscopic Surgery (FLS) certification testing. Surg Endosc. 2011;25(4):1192–8. https://doi.org/10.1007/s00464-010-1343-0 (PMID: 20872021).
Kurimoto T., Urushidani S., Yamada H., Yamanaka K., Nakamura M., Abe S. et al., SINET5: a low-latency and high-bandwidth backbone network for SDN/NFV Era. In: IEEE International Conference on Communications (ICC); 2017. https://doi.org/10.1109/ICC.2017.7996843.
Uhrina M, Holesova A, Bienik J, Sevcik L. Impact of scene content on high resolution video quality. Sensors (Basel). 2021;21(8):2872. https://doi.org/10.3390/s21082872 (PMID: 33921877, PMCID: PMC8073500).
Aghazadeh MA, Jayaratna IS, Hung AJ, Pan MM, Desai MM, Gill IS, et al. External validation of Global Evaluative Assessment of Robotic Skills (GEARS). Surg Endosc. 2015;29(11):3261–6. https://doi.org/10.1007/s00464-015-4070-8 (PMID: 25609318).
Japanese Society for Endoscopic Surgery. Guidelines for the management of endoscopic surgery. Tokyo: Japanese Soc for Endosc Surg; 2014.
Reeve BB, Stover AM, Alfano CM, Smith AW, Ballard-Barbash R, Bernstein L, et al. The Piper Fatigue Scale-12 (PFS-12): psychometric findings and item reduction in a cohort of breast cancer survivors. Breast Cancer Res Treat. 2012;136(1):9–20. https://doi.org/10.1007/s10549-012-2212-4 (PMID: 22933027, PMCID: PMC3739964).
Martinez AW, Phillips ST, Carrilho E, Thomas SW 3rd, Sindi H, Whitesides GM. Simple telemedicine for developing regions: camera phones and paper-based microfluidic devices for real-time, off-site diagnosis. Anal Chem. 2008;80(10):3699–707. https://doi.org/10.1021/ac800112r (PMID: 18407617, PMCID:PMC3761971).
Weinstein RS, Lopez AM, Joseph BA, Erps KA, Holcomb M, Barker GP, et al. Telemedicine, telehealth, and mobile health applications that work: opportunities and barriers. Am J Med. 2014;127(3):183–7. https://doi.org/10.1016/j.amjmed.2013.09.032 (PMID: 24384059).
Kim DK, Yoo SK, Park IC, Choa M, Bae KY, Kim YD, et al. A mobile telemedicine system for remote consultation in cases of acute stroke. J Telemed Telecare. 2009;15(2):102–7. https://doi.org/10.1258/jtt.2008.080713 (PMID: 19246612).
Bolsi A, Lomax AJ, Pedroni E, Goitein G, Hug E. Experiences at the Paul Scherrer Institute with a remote patient positioning procedure for high-throughput proton radiation therapy. Int J Radiat Oncol Biol Phys. 2008;71(5):1581–90. https://doi.org/10.1016/j.ijrobp.2008.02.079 (PMID: 18640501).
Heslop L, Weeding S, Dawson L, Fisher J, Howard A. Implementation issues for mobile-wireless infrastructure and mobile health care computing devices for a hospital ward setting. J Med Syst. 2010;34(4):509–18. https://doi.org/10.1007/s10916-009-9264-y (PMID: 20703905).
Chan FY, Whitehall J, Hayes L, Taylor A, Soong B, Lessing K, et al. Minimum requirements for remote realtime fetal tele-ultrasound consultation. J Telemed Telecare. 1999;5(3):171–6. https://doi.org/10.1258/1357633991933585 (PMID: 10628032).
Marescaux J, Leroy J, Gagner M, Rubino F, Mutter D, Vix M, et al. Transatlantic robot-assisted telesurgery. Nature. 2001;414(6865):379–80. https://doi.org/10.1038/35096636 (Erratum. In: Nature. 2001 Dec 13;414(6865):710. PMID: 11574874).
Marescaux J, Leroy J, Rubino F, Smith M, Vix M, Simone M, et al. Transcontinental robot-assisted remote telesurgery: feasibility and potential applications. Ann Surg. 2002;235(4):487–92. https://doi.org/10.1097/00000658-200204000-00005 (PMID: 11923603, PMCID: PMC1422462).
Anvari M, McKinley C, Stein H. Establishment of the world’s first telerobotic remote surgical service: for provision of advanced laparoscopic surgery in a rural community. Ann Surg. 2005;241(3):460–4. https://doi.org/10.1097/01.sla.0000154456.69815.ee (PMID: 15729068, PMCID:PMC1356984).
Sterbis JR, Hanly EJ, Herman BC, Marohn MR, Broderick TJ, Shih SP, Harnett B, Doarn C, Schenkman NS. Transcontinental telesurgical nephrectomy using the da Vinci robot in a porcine model. Urology. 2008;71(5):971–3. https://doi.org/10.1016/j.urology.2007.11.027 (PMID: 18295861).
Suzuki S, Suzuki N, Hayashibe M, Hattori A, Konishi K, Kakeji Y, et al. Tele-surgical simulation system for training in the use of da Vinci surgery. Stud Health Technol Inform. 2005;111:543–8 (PMID: 15718794).
Choi PJ, Oskouian RJ, Tubbs RS. Telesurgery: Past, Present, and Future. Cureus. 2018;10(5): e2716. https://doi.org/10.7759/cureus.2716. (PMID:30079282; PMCID: PMC6067812).
Hakamada K, Mori M. The changing surgical scene: From the days of Billroth to the upcoming future of artificial intelligence and telerobotic surgery. Ann Gastroenterol Surg. 2021;5(3):268–9. https://doi.org/10.1002/ags3.12466. (PMID: 34095715; PMCID :PMC8164454).
Kim T, Zimmerman PM, Wade MJ, Weiss CA 3rd. The effect of delayed visual feedback on telerobotic surgery. Surg Endosc. 2005;19(5):683–6. https://doi.org/10.1007/s00464-004-8926-6 (PMID: 15776211).
Xu S, Perez M, Yang K, Perrenot C, Felblinger J, Hubert J. Effect of latency training on surgical performance in simulated robotic telesurgery procedures. Int J Med Robot. 2015;11(3):290–5. https://doi.org/10.1002/rcs.1623 (PMID: 25328078).
Perez M, Xu S, Chauhan S, Tanaka A, Simpson K, Abdul-Muhsin H, et al. Impact of delay on telesurgical performance: study on the robotic simulator dV-Trainer. Int J Comput Assist Radiol Surg. 2016;11(4):581–7. https://doi.org/10.1007/s11548-015-1306-y (PMID: 26450105).
Wirz R, Torres LG, Swaney PJ, Gilbert H, Alterovitz R, Webster RJ 3rd, et al. An experimental feasibility study on robotic endonasal telesurgery. Neurosurgery. 2015;76(4):479–84. https://doi.org/10.1227/NEU.0000000000000623, (PMID: 25599203, PMCID: PMC4366329, discussion 484).
Xu S, Perez M, Yang K, Perrenot C, Felblinger J, Hubert J. Determination of the latency effects on surgical performance and the acceptable latency levels in telesurgery using the dV-Trainer(®) simulator. Surg Endosc. 2014;28(9):2569–76. https://doi.org/10.1007/s00464-014-3504-z (PMID: 24671353).
Acknowledgements
This study was conducted as part of the Advanced Telemedicine Network Research Project of the Japan Agency for Medical Research and Development (AMED), and we are grateful for their financial support. We thank all physicians including the gastroenterological and thoracic surgeons, urologists, gynecologists, and engineers, who participating in this study. We also express our deepest gratitude to the Medicaroid Corporation for their cooperation in the experiments.
Funding
This work was supported by a grant from the Japan Agency for Medical Research and Development (AMED) (Grant Number 21hs0122001h0002).
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Eiji Oki is co-first author.
Rights and permissions
About this article

Cite this article
Ebihara, Y., Oki, E., Hirano, S. et al. Tele-assessment of bandwidth limitation for remote robotics surgery. Surg Today 52, 1653–1659 (2022). https://doi.org/10.1007/s00595-022-02497-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00595-022-02497-5