
Abstract
Although robotic telesurgery is growing in popularity, the benefits of telesurgery compared to local surgery are unclear. This study aimed to evaluate the performance of robotic tele-cholecystectomy with a commercial line using the Saroa™ (Riverfield, Inc., Tokyo, Japan) system. The operation rooms of the Hokkaido University Hospital and Kushiro City General Hospital were connected using a best effort-type line (1 Gbps), with a distance of 250 km between the two hospitals. In this experimental single-blind randomized crossover trial, eight expert robotic surgeons performed robotic cholecystectomy in an artificial organ model using the Saroa™ system and were randomized to begin with either local surgery or telesurgery. All surgeons were assessed on task completion time, total path length of the right- and left- hand forceps and camera, Global Evaluative Assessment of Robotic Skills (GEARS), Global Operative Assessment of Laparoscopic Skills (GOALS), and System and Piper Fatigue Scale-12 (PFS-12). In all experiments, the communication environment was stable and the mean communication delay was 8 ms (3–31 ms). All tele-cholecystectomies were performed safely. There was no significant difference in completion time (P = 0.495), score of GEARS (P = 0.258), GOALS (P = 0.180), or PFS-12 (P = 0.528) between local surgery and telesurgery. The total path of the forceps tended to be longer in tele-cholecystectomy, particularly with significantly longer left-hand forceps total path length (P = 0.041). Robotic tele-cholecystectomy using a commercial line can be performed safely as same as local robotic surgery, but the total path of the left-hand forceps was prolonged in robotic tele-cholecystectomy due to overshoot. Therefore, a solution for overshooting will be required in the future.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In recent years, surgical robots have been deployed in a large number of hospitals worldwide and have become increasingly popular in Japan. Furthermore, the development of high-speed, high-capacity communication technology using optical fiber and 5th generation mobile communication systems (5G) along with the development of new surgical robots has made remote surgery a reality [1]. Telerobotic surgery has been studied since the 1970s, and the world's first tele-laparoscopic cholecystectomy was performed between the US and France in 2001 [2]. This was followed by a number of remote surgeries in Canada [3], all of which were reported to be successful, and experiments with remote robotics were also reported in Japan [4]. However, there are still many problems to be solved before robotic telesurgery may be implemented in society. Few reports have examined telesurgery in comparison to local surgery, and existing evidence is insufficient. The aim of this study was to assess the technical evaluation of robotic tele-cholecystectomy with a commercial line using a Saroa™ (Riverfield, Inc., Tokyo, Japan).
Materials and methods
Participants and experimental design
We used a prospective, single-blind, randomized, crossover study to compare the technical evaluation of robotic tele-cholecystectomy and robotic local-cholecystectomy. Eight expert robotic surgeons with endoscopic surgical skill qualification systems from the Japan Society for Endoscopic Surgery (JSES) [5] participated in this experiment. The technical evaluation was conducted by two surgeons certified in the JSES proctor system [6]. The study was conducted from July to September 2021. Participants were consecutively enrolled from affiliated hospitals. Surgeons with conflicting schedules on the day of the experiment were excluded. Participants were randomly assigned to group A or group B sequentially in a 1:1 ratio by recruitment number. The participants in Group A performed local-cholecystectomy initially followed by tele-cholecystectomy (n = 4), and the participants in Group B performed tele-cholecystectomy initially followed by local-cholecystectomy (n = 4). No practice was allowed before evaluation of performance, which was supervised and recorded. One day was allowed to elapse (i.e., the washout period) before each participant performed the next task. A flowchart of the trial is shown in Fig. 1.

Flowchart of the trial
Network connections
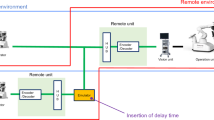
The operation rooms of the Hokkaido University Hospital and Kushiro City General Hospital, located about 250 km apart, were connected using a commercial best effort-type line (FLET’S VPN PRIO) provided by NTT East (Nippon Telegraph and Telephone East Corporation, Tokyo, Japan). The maximum communication bandwidth was set at 1-Gbps. For CODEC, we used the Zao-SH encoder and Zao-View decoder of Soliton Systems (Tokyo, Japan). This CODEC has a function that reserves 1-Mbps of communication bandwidth preferentially for robot operation signals and allocates the remaining bandwidth to video transmission. We defined communication delay time as round-trip time (RTT) or the combined transmission delay of three steps: (1) the encoding delay; (2) the round-trip delay of the communication line; and (3) the decoding delay (Fig. 2).

Network system. Round trip time (RTT) is composed of three steps: (1) the encoding delay; (2) the round-trip delay of the communication line; and (3) the decoding delay
Robot system
We used a Saroa™ surgical robot system (Riverfied, Inc., Tokyo, Japan). The robot uses a pneumatically powered robotic system from Riverfield, which is being developed in Japan [7]. An Olympus 3D scope (Olympus, Tokyo, Japan) was installed in the system. The surgeon cockpit was installed at Hokkaido University, and the operation unit was installed at Hokkaido University Hospital and Kushiro City General Hospital. The surgeon cockpit was installed outside the operation room so that the participants were not aware which operation unit was connected.
Skill test and evaluation
We used a gallbladder model manufactured by FASOTEC Co., Ltd. (Chiba, Japan). The right hand was used as a monopolar scissors that dissected using electrocautery, and the left hand used fenestrated forceps. After identifying the cystic duct and the cystic artery, both were clipped proximally and distally, once each by the assistant surgeon. The gallbladder was then removed from the gallbladder bed to complete the task (Fig. 3). We measured task completion time, total path length of the right and left -hand forceps and camera, and robotic surgical skill using the Global Evaluative Assessment of Robotic Skills (GEARS) [8] and Global Operative Assessment of Laparoscopic Skills (GOALS) [9]; subjective evaluation of the surgeon was validated using the System and Piper Fatigue Scale-12 (PFS-12) [10].

Skill test (Cholecystectomy). A The gallbladder model was manufactured by FASOTEC Co., Ltd. (Chiba, Japan). B The right hand was used as a monopolar scissors that dissected using electrocautery, and the left hand was used as a fenestrated forceps. After identifying the cystic duct and the cystic artery, both were clipped proximally and distally, once each by an assistant surgeon. C The gallbladder was then removed from the gallbladder bed to complete the task. D Photograph after completion of cholecystectomy
Statistical analysis
The task completion time, total path length of the right and left-hand forceps and camera, and each test score were compared between the groups using the Mann–Whitney U test for continuous variables. Statistical analyses comparing tele-cholecystectomy and local-cholecystectomy data of the same surgeons were performed using a paired two-tailed Student’s t test. Statistical significance was set at P < 0.05. Statistical analysis was performed using the JMP® 15 software (SAS Institute Inc., Cary, NC, USA).
Results
In all experiments, the communication environment was stable without image degradation, and the mean RTT was 8 ms (3–31 ms). All tele-cholecystectomies were performed safely and without gallbladder injury. The cholecystectomy completion time was as follows: local, 620.5 s (346.0–1097.0); tele: 625.5 s (411.0–1030.0) (P = 0.495) (Table 1). An individual examination of completion time was prolonged in six out of eight (75%) of the surgeons in tele-cholecystectomy, although no significant difference was observed (P = 0.119). The GEARS score (local: 29.0 [24–30], tele: 26.5 [20–30], P = 0.180), GOALS score (local: 23.5 [20,21,22,23,24,25], tele: 21.5 [18,19,20,21,22,23,24,25], P = 0.258), and PFS-12 score (local: 35.0 [12–63], tele: 51.0 [11–69], P = 0.528) were not found to be significantly different between local- and tele-cholecystectomy (Table 1). The total path of the forceps in tele-cholecystectomy was significantly longer for the left-hand forceps (local: 5924.5 mm [4151–8602], tele: 8742.0 mm [4151–8602], P = 0.041), and the total path length of the right hand (local: 6051.5 mm [4413–8189], tele: 8826.0 mm [6690–13718], P = 0.089), camera (local: 6138.5 mm [1744–12821], tele: 7491.5 mm [5185–12821], P = 0.126), and both-hand forceps and camera (local: 15,988 mm [11674–23262], tele: 25,783.0 mm [18565–39079], P = 0.061) were not significantly different between local- and tele-cholecystectomy (Table 2). Figure 4 shows a radar chart of the items examined in the present study. The measurements of tele-cholecystectomy are shown as a percentage of local-cholecystectomy. There was no difference with regard to skill assessment, although a large gap was found in the areas of total path length of the forceps between local- and tele-cholecystectomy.

A radar chart of the items examined in the present study. The measurements of tele-cholecystectomy are shown as a percentage of local-cholecystectomy. There was no difference with regard to skill assessment, although a large gap was found in the areas of total path length of the forceps between local- and tele-cholecystectomy. GEARS Global Evaluative Assessment of Robotic Skills; GOALS Global Operative Assessment of Laparoscopic Skills; PFS-12: Piper Fatigue Scale-12; Right forceps: The total path length of the right-hand forceps; Left forceps: The total path length of the left-hand forceps; Camera: The total path length of the camera; Both forceps and camera: The total path length of the both-hand forceps and camera
Discussion
In this pilot study, we set up the Japanese-made surgical robot system, Saroa™, in an operating room 250 km away from the operator by connecting a best effort-type line to investigate the technical impact of robotic tele-cholecystectomy. No technical differences were observed between tele-cholecystectomy or local cholecystectomy performed by expert robotic surgeons.
Almost 20 years ago, Marescaux [2, 11] performed the first clinical tele-cholecystectomy using the ZEUS robotic system and the Transatlantic Optical Faber Network. This operation, also known as the Lindbergh operation, is considered the gold standard for tele-surgery. Twenty-two subsequent telesurgeries were performed at a hospital in North Bay, approximately 400 km north of Hamilton, Canada [3]. Both surgeries were successful, but the transatlantic connection used expensive leased lines, while the Canadian clinical cases used Internet Protocol-Virtual Private Network lines, a special government-developed inter-hospital network. In the USA, Florida Hospital has successfully used the internet for robot-assisted tele-surgery; surgeons in Texas, 1200 miles away from Florida, operated on a simulated patient by remote control of a da Vinci robot via the internet [12]. In Japan, a robot teleoperation simulation for training was reported by Hashizume et al. [13]. However, the underdevelopment of information and communication technology became a decisive factor, and research on tele-surgery was suspended for a long time [14]. In recent years, the development of high-speed and high-capacity communication technologies using fiber optics and 5G along with the development of new surgical robots have made teleoperation a reality [15].
Regarding transmission delay, it has been reported that operability decreases when the delay time perceived by the surgeon exceeds 200 ms, that errors increase when it exceeds 300 ms [16, 17], and that work becomes almost impossible when it exceeds 700 ms [18]. Many reports suggest that the delay time should be less than 200 ms, and ideally less than 100 ms, to perform normal robot operations [19, 20]. Morohashi H et al. reported that the mean RTT for the guaranteed-type lines was 4 (4–7) ms, and the mean RTT for the best effort-type line was 10 (9–13) ms for connecting hospitals 150 km apart [4]. In the present study, the communication environment was stable, and the mean RTT for the best effort-type line (1 Gbps) was 8 ms (3–31 ms). Recent advances in telecommunications technology have helped resolve communication delays. In this study, we used a commercial best-effort type line, which advertises the maximum communication bandwidth among closed circuits with guaranteed security. It is inexpensive and widely used, but has the risk of falling below the minimum bandwidth because the available bandwidth is affected by communication congestion. The reason stable communication is provided by a commercial best-effort type line is that advances in encoder and decoder technology have enabled low-bandwidth communication, and the required communication bandwidth, including the images in this case, has always been less than 5-Mbps. In the future, studies assessing surgical procedures that demand more precise skill and those determining the limits of communication delay for each procedure are required.
In the present study, there were no significant differences between the local-cholecystectomy and tele-cholecystectomy in completion times (P = 0.495), technical evaluation score (GEARS: P = 0.180, GOALS: P = 0.258), and surgeon fatigue score (PFS-12: P = 0.528). However, a prolongation of the total path length of left-hand forceps was observed in tele-cholecystectomy (P = 0.041) even when the RTT was equal to or less than 30 ms. Orosco et al. reported that under time delayed conditions, the surgeon perceives the delayed visual feedback as inadequate instrument displacement, causing them to advance their robotic controller even further [21]. This results in the instrument overshooting the intended position. When the time-delayed video feed reaches the surgeons, they become aware of the overshoot and attempt to correct it. Under conditions of communication delays, the total path length of the forceps increases due to overshoot. In the present study, an extension of the total path length of the forceps was also observed in the slightly more complex task of cholecystectomy, even with a small communication delay, and overshooting should be noted. We believe that a prolongation of the total path length of forceps was due to overshoot, and that there may be two reasons for the greater effect on the left-hand forceps than on the right-hand forceps. One is that the left-hand forceps was needed for more frequent and detailed work for grasping tissue at its most adequate point before dissection, in contrast to the right hand, which was only used for the simple motion of dissection. The second reason is that the participants’ dominant hands were all on the right side, so precise manipulation with the non-dominant left hand was affected by overshoot, even with short delay time. Tremor compensation [22, 23], virtual fixtures [24, 25], and robotic arm motion scaling have been reported to be useful for improving the accuracy, safety, and control of telerobotic systems. Moreover, it has been considered necessary to develop a system that would overcome overshoot in more complex skills. Advanced motion scaling functions and virtual fixers need to be developed to solve overshoot in robotic tele-surgery. In the future, it is expected that surgeon training, motion scaling, the use of augmented reality and advanced surgeon visual interfaces, as well as semi-autonomous robotic capabilities will be incorporated to optimize the performance of robotic tele-surgery.
The robotic tele-surgery using 5G communications is expected to be feasible on remote islands, developing regions, and in disaster-affected areas where it is difficult to install wired internet cables. In addition, for surgeries performed in the current coronavirus disease 2019 pandemic environment, precautions to prevent infectious disease spread through human contact are needed. In this context, 5G-based robotic tele-surgery is expected to support regional hospitals across Japan and help train young surgeons. In recent years, a number of experimental results have been reported on remote robotic surgery using surgical robots. Tele-robotic surgery is expected to spread rapidly and widely throughout the world; however, its safe spread will require common rules. The Society of American Gastrointestinal Endoscopic Surgeons has provided guidelines for the surgical practice of telemedicine and has advised that telemedicine surgery be performed under strict institutional review board supervision with careful design and methodology [26]. In Japan, guidelines are being developed for optimal communication systems for the clinical application of robotic telesurgery, focusing on safety, ethics, and cost.
This study has several limitations. Because of the limited duration of the experiment, the number of participating surgeons and tasks was small, and the time to operation for robot surgery was short. The current experiment was a study conducted by expert surgeons only, and judgments about introduction in clinical practice should be made with caution. A well-designed randomized controlled trial is required to validate our findings. In the future, a large-scale comparative study is anticipated based on the data from this pilot study.
Conclusion
No technical differences were observed in expert robotic surgeons, either tele-cholecystectomy or local cholecystectomy in this system, but it was found that the total path of the left-hand forceps was prolonged in robotic tele-cholecystectomy due to the overshoot. In the future, a solution to overshooting will be necessary.
Availability of data and material
The datasets during and/or analysed during the current study available from the corresponding author on reasonable request.
References
Zheng J, Wang Y, Zhang J, Guo W, Yang X, Luo L et al (2020) 5G ultra-remote robot-assisted laparoscopic surgery in China. Surg Endosc 34:5172–5180. https://doi.org/10.1007/s00464-020-07823-x
Marescaux J, Leroy J, Gagner M, Rubino F, Mutter D, Vix M et al (2001) Transatlantic robot-assisted telesurgery. Nature 414:379–380. https://doi.org/10.1038/35096636. Erratum in: Nature (2001) 414:710. https://doi.org/10.1038/414710a
Anvari M, McKinley C, Stein H (2005) Establishment of the world’s first telerobotic remote surgical service: for provision of advanced laparoscopic surgery in a rural community. Ann Surg 241:460–464. https://doi.org/10.1097/01.sla.0000154456.69815.ee
Morohashi H, Hakamada K, Kanno T, Kawashima K, Akasaka H, Ebihara Y et al (2022) Social implementation of a remote surgery system in Japan: a field experiment using a newly developed surgical robot via a commercial network. Surg Today 52:705–714. https://doi.org/10.1007/s00595-021-02384-5
Japanese Society for Endoscopic Surgery (2014) Guidelines for the management of endoscopic surgery. Japanese Society for Endoscopic Surgery, Tokyo
Shibasaki S, Suda K, Kadoya S, Ishida Y, Nakauchi M, Nakamura K et al (2022) The safe performance of robotic gastrectomy by second-generation surgeons meeting the operating surgeon’s criteria in the Japan Society for Endoscopic Surgery guidelines. Asian J Endosc Surg 15:70–81. https://doi.org/10.1111/ases.12967
Tadano K, Kawashima K, Kojima K, Tanaka N (2010) Development of a pneumatic surgical manipulator ibis IV. J Robot Mechatron 22:179–188. https://doi.org/10.20965/jrm.2010.p0179
Aghazadeh MA, Jayaratna IS, Hung AJ, Pan MM, Desai MM, Gill IS, Goh AC (2015) External validation of global evaluative assessment of robotic skills (GEARS). Surg Endosc 29:3261–3266. https://doi.org/10.1007/s00464-015-4070-8
Vassiliou MC, Feldman LS, Andrew CG, Bergman S, Leffondré K, Stanbridge D, Fried GM (2005) A global assessment tool for evaluation of intraoperative laparoscopic skills. Am J Surg 190:107–113. https://doi.org/10.1016/j.amjsurg.2005.04.004
Reeve BB, Stover AM, Alfano CM, Smith AW, Ballard-Barbash R, Bernstein L et al (2012) The piper fatigue scale-12 (PFS-12): psychometric findings and item reduction in a cohort of breast cancer survivors. Breast Cancer Res Treat 136:9–20. https://doi.org/10.1007/s10549-012-2212-4
Marescaux J, Leroy J, Rubino F, Smith M, Vix M, Simone M et al (2002) Transcontinental robot-assisted remote telesurgery: feasibility and potential applications. Ann Surg 235:487–492. https://doi.org/10.1097/00000658-200204000-00005
Sterbis JR, Hanly EJ, Herman BC, Marohn MR, Broderick TJ, Shih SP et al (2008) Transcontinental telesurgical nephrectomy using the da Vinci robot in a porcine model. Urology 71:971–973. https://doi.org/10.1016/j.urology.2007.11.027
Suzuki S, Suzuki N, Hayashibe M, Hattori A, Konishi K, Kakeji Y, Hashizume M (2005) Tele-surgical simulation system for training in the use of da Vinci surgery. Stud Health Technol Inform 111:543–548
Choi PJ, Oskouian RJ, Tubbs RS (2018) Telesurgery: past, present, and future. Cureus 10:e2716. https://doi.org/10.7759/cureus.2716
Hakamada K, Mori M (2021) The changing surgical scene: from the days of Billroth to the upcoming future of artificial intelligence and telerobotic surgery. Ann Gastroenterol Surg 5:268–269. https://doi.org/10.1002/ags3.12466
Kim T, Zimmerman PM, Wade MJ, Weiss CA 3rd (2005) The effect of delayed visual feedback on telerobotic surgery. Surg Endosc 19(5):683–686. https://doi.org/10.1007/s00464-004-8926-6
Xu S, Perez M, Yang K, Perrenot C, Felblinger J, Hubert J (2015) Effect of latency training on surgical performance in simulated robotic telesurgery procedures. Int J Med Robot 11:290–295. https://doi.org/10.1002/rcs.1623
Perez M, Xu S, Chauhan S, Tanaka A, Simpson K, Abdul-Muhsin H, Smith R (2016) Impact of delay on telesurgical performance: study on the robotic simulator dV-Trainer. Int J Comput Assist Radiol Surg 11:581–587. https://doi.org/10.1007/s11548-015-1306-y
Wirz R, Torres LG, Swaney PJ, Gilbert H, Alterovitz R, Webster RJ 3rd et al (2015) An experimental feasibility study on robotic endonasal telesurgery. Neurosurgery 76:479–484. https://doi.org/10.1227/NEU.0000000000000623. (discussion 484)
Xu S, Perez M, Yang K, Perrenot C, Felblinger J, Hubert J (2014) Determination of the latency effects on surgical performance and the acceptable latency levels in telesurgery using the dV-Trainer(®) simulator. Surg Endosc 28:2569–2576. https://doi.org/10.1007/s00464-014-3504-z
Orosco RK, Lurie B, Matsuzaki T, Funk EK, Divi V, Holsinger FC et al (2021) Compensatory motion scaling for time-delayed robotic surgery. Surg Endosc 35:2613–2618. https://doi.org/10.1007/s00464-020-07681-7.Erratum.In:SurgEndosc(2020)
Ang WT, Pradeep PK, Riviere CN (2004) Active tremor compensation in microsurgery. Conf Proc IEEE Eng Med Biol Soc 2004:2738–2741. https://doi.org/10.1109/IEMBS.2004.1403784
Riviere CN, Gangloff J, De Mathelin M (2006) Robotic compensation of biological motion to enhance surgical accuracy. Proc IEEE 94:1705–1716. https://doi.org/10.1109/JPROC.2006.880722
Becker BC, MacLachlan RA, Lobes LA, Hager GD, Riviere CN (2013) Vision-based control of a handheld surgical micromanipulator with virtual fixtures. IEEE Trans Robot 29:674–683. https://doi.org/10.1109/TRO.2013.2239552
Park S, Howe RD, Torchiana DF (2001) Virtual fixtures for robotic cardiac surgery. In: Niessen WJ, Viergever MA (eds) Lecture Notes in Computer Science International conference on medical image computing and computer-assisted intervention. Springer, New York, pp 1419–1420
Society of American Gastrointestinal and Endoscopic Surgeons (2000) Guidelines for the surgical practice of telemedicine. Surg Endosc 14:975–979. https://doi.org/10.1007/s004640000290
Acknowledgements
This study was conducted as part of the Advanced Telemedicine Network Research Project of the Japan Agency for Medical Research and Development (AMED), and we are grateful for the financial support. We thank all surgeons and engineers participating in this study. We would also like to express our deepest gratitude to the NIPPON TELEGRAPH AND TELEPHONE EAST CORPORATION, and Riverfied, Inc. for their cooperation in the experiments. We would like to thank Editage (www.editage.com) for English language editing.
Funding
This work was supported by a grant from the Japan Agency for Medical Research and Development (AMED) (Grant Number 21hs0122001h0002).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by YE, HT and SH. The first draft of the manuscript was written by YE and SH and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no relevant financial or non-financial interests to disclose.
Ethical approval
This is an observational study. The Hokkaido University Research Ethics Committee has confirmed that no ethical approval is required.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent to publish
All authors were confirmed that consent to publish has been received.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ebihara, Y., Hirano, S., Takano, H. et al. Technical evaluation of robotic tele-cholecystectomy: a randomized single-blind controlled pilot study. J Robotic Surg 17, 1105–1111 (2023). https://doi.org/10.1007/s11701-023-01522-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11701-023-01522-0