
Abstract
Purpose
The exact relationship between larger caseload volume and lower morbidity following esophagectomy has not been established. This study investigates the effect of surgical volumes on reducing postoperative complications and length of stay after esophagectomy.
Methods
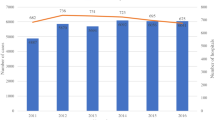
Patient and hospital data were collected electronically via a web-based questionnaire sent to surgeons in the Japan Surgical Society. Data were based on 642 patients treated with esophagectomy at 183 hospitals between November 1, 2006 and February 28, 2007. Multivariate analysis revealed that postoperative morbidity and length of stay regressed against hospital and surgeon volumes, patient characteristics, and details of the procedures.
Results
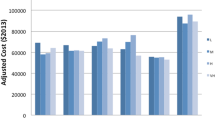
In a logistic regression model, esophagectomies by surgeons performing a high volume of operations (>100 cases; “high case-volume surgeons”) were followed by a significantly lower rate of postoperative complications (odds ratio [OR], 0.49; 95% confidence interval (CI), 0.24–0.98, P = 0.04). In a proportional hazard model, high-volume surgeons reduced the length of stay significantly: the hazard ratio for medium casevolume surgeons (50–99 cases) was 1.53 [95% CI, 1.14–2.06, P = 0.00], whereas that for the highest case-volume surgeons was 1.34 [95% CI, 1.00–1.79, P = 0.05] vs the lowest case-volume surgeons. Neither postoperative complications nor length of stay were significantly associated with hospital volume.
Conclusion
These findings indicate that morbidity after esophagectomy is more dependent on individual surgeon-specific skill than on hospital-based factors.
Similar content being viewed by others
References
Birkmeyer JD, Siewers AE, Finlayson EV, Stukel TA, Lucas FL, Batista I et al. Hospital volume and surgical mortality in the United States. N Engl J Med 2002;346:1128–1137.
Birkmeyer JD, Stukel TA, Siewers AE, Goodney PP, Wennberg DE, Lucas FL. Surgeon volume and operative mortality in the United States. N Engl J Med 2003;349:2117–2127.
Begg CB, Cramer LD, Hoskins WJ, Brennan MF. Impact of hospital volume on the operative mortality for major cancer surgery. JAMA 1998;280:1747–1751.
Urbach DR, Bell CM, Austin PC. Differences in operative mortality between high- and low-volume hospitals in Ontario for 5 major surgical procedures: estimating the number of lives potentially saved through regionalization. CMAJ 2003;168:1409–1414.
Finlayson EV, Goodney PP, Birkmeyer JD. Hospital volume and operative mortality in cancer surgery: a national study. Arch Surg 2003;138:721–725.
Dimick JB, Cattaneo SM, Lipsett PA, Pronovost PJ, Heitmiller RF. Hospital volume is related to clinical and economic outcomes for esophageal resection in Maryland. Ann Thorac Surg 2001;72:334–339.
Dimick JB, Cowan JA Jr, Ailawadi G, Wainess RM, Upchurch GR Jr. National variation in operative mortality rates for esophageal resection and the need for quality improvement. Arch Surg 2003;138:1305–1309.
Gillison EW, Powell J, McConkey CC, Spychal RT. Surgical workload and outcome after resection for carcinoma of the oesophagus and cardia. Br J Surg 2002;89:344–348.
Bachmann MO, Alderson D, Edwards D, Wotton S, Bedford C, Peters TJ et al. Cohort study in South and West England of the influence of specialization on the management and outcome of patients with oesophageal and gastric cancers. Br J Surg 2002;89:914–922.
Patti MG, Corvera CU, Glasgow RE, Way LW. A hospital’s annual rate of esophagectomy influences the operative mortality rate. J Gastrointest Surg 1998;2:186–192.
Okuyama M, Motoyama S, Suzuki H, Saito R, Maruyama K, Ogawa J. Hand-sewn cervical anastomosis versus stapled intrathoracic anastomosis after esophagectomy for middle or lower thoracic esophageal cancer: a prospective randomized controlled study. Surgery Today. 2007;37:947–952.
Diggle PJ, Heagerty P, Liang K-Y, Zeger SL. Analysis of longitudinal data. 2nd ed. Oxford: Oxford University Press; 2001.
Zhang GH, Fujita H, Yamana H, Kakegawa T. A prediction of hospital mortality after surgical treatment for esophageal cancer. Surg Today 1994;24:122–127.
Kazui T, Osada H, Fujita H, Japanese Association for Thoracic Surgery Committee for Scientific Affairs. Thoracic and cardiovascular surgery in Japan during 2004. Jpn J Thorac Cardiovasc Surg 2006;54:363–385.
Birkmeyer JD, Finlayson EV, Birkmeyer CM. Volume standards for high-risk surgical procedures: Potential benefits of the Leapfrog initiative. Surgery 2001;130:415–422.
Author information
Authors and Affiliations
Consortia
Rights and permissions
About this article
Cite this article
Yasunaga, H., Matsuyama, Y., Ohe, K. et al. Effects of hospital and surgeon case-volumes on postoperative complications and length of stay after esophagectomy in Japan. Surg Today 39, 566–571 (2009). https://doi.org/10.1007/s00595-008-3832-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00595-008-3832-5