
Abstract
Background
The purpose of the current study was to clarify the role of the quadriceps tendon (QT) autograft for primary ACL reconstruction. Thus, a Bayesian network meta-analysis comparing patients undergoing a primary ACL reconstruction with QT versus patellar tendon (PT) and hamstring tendon (HT) autografts was conducted.
Material and methods
This Bayesian network meta-analysis was conducted according to the PRISMA extension statement for reporting systematic reviews incorporating network meta-analyses of health care interventions. In January 2020, the main databases were accessed. Articles comparing the outcomes of the QT autograft versus HT autograft and/or PT autograft for primary ACL reconstruction were included in the present study. The statistical analysis was performed with STATA Software/MP, through a Bayesian hierarchical random-effect model analysis.
Results
Data from a total of 2603 knees were analysed. The overall mean follow-up was 35.0 months. Among the different grafts were evidenced comparable values of IKDC, Tegner and Lysholm score. The QT autograft detected comparable rate of Lachman test > 3 mm, Pivot shift test > 3 m and instrumental laxity > 3 mm. The QT autograft showed a lower rate of autograft failure above all. The QT autograft detected the reduced rate of AKP than the PT.
Conclusion
Quadriceps tendon autograft may represent a feasible option for primary ACL reconstruction. These results must be interpret within the limitations of the present network meta-anlaysis.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The anterior cruciate ligament (ACL) stabilizes the knee and prevents anterior translation of the tibia in reference to the femur. According to epidemiological reports estimating 100,000 to 200,000 ACL ruptures per year in the USA alone, it is one of the most common injuries of active people [1]. If not repaired, a torn ACL can lead to joint instability, accelerate degenerative joint degradation and cause damage to meniscus and cartilage [2]. Therefore, surgical reconstruction in selected patients may be necessary [3]. Several surgical techniques such as allografts, autografts and synthetic grafts can be used for ACL reconstruction [4]. In patients with joint instability, the gold standard for ACL surgery is the reconstruction with an autologous tendon autograft [5]. Currently, the patellar tendon (PT) and hamstring (HT) autograft are believed to be the best available solution [6, 7]. Recently, there has been growing clinical interest regarding the role of the quadriceps tendon (QT) autograft for ACL reconstruction. Although this autograft has been used mainly in revision settings, some surgeons believe that this graft can achieve even better outcomes than standard PT and HT autografts also for primary ACL reconstruction. Clinical studies focusing on the use of the QT for primary ACL reconstruction report reliable long-term outcomes and low donor site morbidity rates [8]. Moreover, biomechanical proprieties of QT grafts promise to be the optimal for ACL reconstruction [9,10,11].
Currently, lack of evidence exists regarding the advantages of the QT as a source of autograft compared to PT and HT grafts. The purpose of the current study was to investigate the role of the QT for primary ACL reconstruction. A Bayesian network meta-analysis comparing patients undergoing a primary ACL reconstruction with QT versus PT or HT autograft was conducted.
Material and methods
Search strategy
This Bayesian network meta-analysis was conducted according to the PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions [12]. The preliminary protocol to guide the research was the following:
-
P (Patients): primary ACL rupture;
-
I (Intervention): QT autograft;
-
C (Comparison): PT autograft, HT autograft;
-
O (Outcomes): clinical scores, joint stability, anterior knee pain, failures.
Literature search
Two independent authors (FM and AD) performed the data extraction. In January 2020, the following databases were accessed: Cochrane Systematic Reviews, Scopus, PubMed, EMBASE, CINAHL and Google Scholar. The following keywords were used for search either isolated or in combinations: resulting titles were screened by the authors. The full text of the articles of interest was accessed. The bibliography of the full-text articles was also screened.
Eligibility criteria
Articles comparing the outcomes of the QT autograft versus HT and/or PT autograft for primary ACL reconstruction were included in the present study. According to the Oxford Centre of Evidence-based Medicine [13], level of evidence I to III were included. Articles in English, German, Italian, French and Spanish were considered. Cadaveric, biomechanics, computational and in vitro studies, as well as other meta-analysis or review studies, editorials, letters or expert opinions were excluded. Studies concerning QT autograft in revision settings were excluded. Only studies reporting data from a minimum 12-month follow-up were considered for inclusion. Only studies reporting quantitative data under the outcomes of interest were eligible. To reduce the indirect comparisons and to improve the evidence regarding the present Bayesian network meta-analysis, studies reporting data concerning HT versus PT autograft for primary ACL reconstruction were included. To be eligible for inclusion, high-quality papers were required, with sample randomization, comparability baseline, same techniques and protocols, and quantitative data under the same outcome of interest. Disagreements between the authors were debated and mutually solved.
Outcomes of interest
Two independent authors performed data extraction (FM and AD). Studies generalities were extracted: author, year, type of study, level of evidence, number of patients and procedures, related mean age and duration of the follow-up. The outcomes of interest were: (1) clinical scores: subjective scale of the International Knee Documentation Committee (IKDC) [14], Lysholm Knee Scoring Scale [15], Tegner Activity Scale [16]; (2) joint laxity: Lachman test > 3 mm, Pivot shift test > 3 mm, arthrometer laxity > 3 mm; (3) post-operative complications: rate of failures and anterior knee pain (AKP). Concerning the instrumental laxity evaluation performed with an arthrometer, it was referred to as both KT-1000 and KT-2000 (MEDmetric Corp, San Diego, California). Both devices reproduce a linear force at 134 N to evaluate the knee laxity. These devices have been validated in other studies [17, 18]. A tibial displacement > 3 mm is considered as failure.
Methodological quality assessment
For the methodological quality assessment, the Review Manager Software Version 5.3 (The Nordic Cochrane Centre, Copenhagen) was used. The risk of bias summary tool was performed according to the authors' judgements about each risk of bias item for each included study.
Statistical analysis
The statistical analyses were performed by the senior author (FM). For the baseline comparability, the analysis of variance (ANOVA) test was performed through the IBM SPSS Software. Values of P > 0.5 were considered satisfactory. The statistical analysis was performed with STATA Software/MP, Version 14.1 (Stata Corporation, College Station, Texas, USA). The Bayesian hierarchical random-effect model analysis was adopted in all the comparisons. For continuous data, the generic inverse variance statistic method was adopted with the standardized mean difference effect measure (SMD). For binary data, the log odds ratio (LOR) effect measure was adopted. All the comparisons were matched with a reference value. Scores were compared with their maximum value, while dichotomic comparisons (rate of laxity and complications) with the null value. The edge network plot described contribution and nature of comparisons among studies. The interval plot was performed to rank the final effect of all the comparisons under the same endpoint. To evaluate the risk of publication bias, the funnel plot was performed in all the comparisons. The confidence interval (CI) and percentile interval (PrI) were set at 0.95 in all the comparisons. The overall inconsistency was evaluated through the equation for global linearity via the Wald test. If the P value > 0.5, the null hypothesis cannot be rejected, and the consistency assumption could be accepted at the overall level of each treatment.
Results
Search result
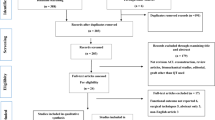
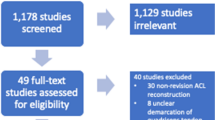
Literature search and cross-references of the bibliography resulted in 436 studies. After excluding duplicates (97), further articles were excluded because they did not focus on the topic (141) or did not provide any comparison between the outcomes of interest (94), leaving 103 articles. After reading the abstracts, further 67 articles were rejected because incompatibility with the eligibility criteria was determined. During the full-text screening, 22 other articles were excluded because of a lack of quantitative data under the outcomes of interest. This left 15 papers treating QT versus PT or HT autografts. A total of 10 high-quality papers treating PT versus HT were added. This last operation left 25 articles for the present study. The flow chart of the literature search is shown in Fig. 1.

Flow chart of the literature search
Methodological quality assessment
The risk of bias summary detected a lack of blinding, especially among the QT autograft studies, improving the risk of detection bias. The randomization was promoted by 42% of the studies; therefore, the risk of selection bias was low in the 60% of the studies included. The risk of attrition and reporting bias was estimated as low in 65% of the studies included. The risk of unknown bias was estimated as low in 70% of the studies included. Therefore, a good quality of methodological assessment can be concluded for this work. The authors' judgement about each risk of bias item for each study included is shown in Fig. 2.

Risk of bias summary
Patient demographic
Data from a total of 2603 knees were analysed. The overall mean follow-up was 35.0 ± 24.8 months. In the QT group, a total of 856 knees were analysed. The mean age was 29.16 ± 1.6 years. In the HT and PT group, a total of 729 and 967 patients were analysed, respectively. The mean age in the HT and PT was 28.83 ± 3.4 and 28.60 ± 5.0, respectively. The ANOVA detected good comparability with regard to patients’ age (P = 0.8). Characteristics of the studies included and the demographic data are shown in Table 1.
Results of the network comparisons: scores
The QT scored worst in terms of IKDC (SMD:−15.38; 95% CI:−19.53,−11.24). Tegner (SMD:−3.89; 95% CI:−4.90,−2.88) and Lysholm scores (SMD:−10.18; 95% CI:−13.42,−6.95) were similar. The funnel plots resulted acceptable. The test for overall inconsistency found statistically significant similarity (P = 0.03, P = 0.09, P = 0.1, respectively). The analysis of these endpoints is shown in Fig. 3.

Overall network comparisons regarding the endpoint: scores
Results of the network comparisons: laxity
Analysis of laxity resulted similar between the groups. The QT detected the reduced rate of instrumental laxity > 3 mm (LOR: 4.02; 95% CI: 2.48, 5.57) and intermediate values of Lachman (LOR: 5.06; 95% CI: 2.93, 7.18) and Pivot shift (LOR: 5.50; 95% CI: 3.38, 7.61) test > 3 mm. The funnel plots detected good and symmetrical distribution. The test for overall inconsistency found statistically significant similarity (P = 0.008, P = 0.02, P = 0.01, respectively). The analysis of these endpoints is shown in Fig. 4.

Overall network comparisons regarding the endpoint: laxity
Results of the network comparisons: complication
The results showed the lower rate of autograft failure (LOR: 1.39; 95% CI: 0.49, 2.29), followed by the PT (LOR: 1.54; 95% CI: 0.76, 2.32) and HT (LOR: 1.85; 95% CI: 1.08, 2.62). The rate of anterior knee pain for the QT (LOR: 2.23; 95% CI: 0.84, 3.63) was greater than that for the HT (LOR: 2.00; 95% CI: 0.62, 3.38) but lower than that for the PT (LOR: 3.75; 95% CI: 2.37, 5.14). The funnel plots were symmetric and very good distributed under the range of acceptability. The test for overall inconsistency through the equation for global linearity evidenced optimal transitivity in the network AKP and failures (P = 0.6, P = 0.6). The analysis of these endpoints is shown in Fig. 5.

Overall network comparisons regarding the endpoint: complications
Discussion
The main findings of this Bayesian network meta-analysis are that the quadriceps tendon autograft may represent a feasible option for primary ACL reconstruction. The QT autograft reported lower rate of failure compared to both PT and HT autografts. Moreover, a reduced rate of AKP compared to the PT autograft has been observed. Analysis of joint laxity and clinical scores found comparability among the grafts.
The scores Lysholm and IKDC represent two valid and responsive patient-reported outcome measures (PROMs) to assess patients after ALC reconstruction [16, 43]. Tegner scale is one of the most frequent used activity rating score and is been validated also in studies on ACL reconstruction [16]. In the present network analysis, these scores detected similarity among the grafts. It is controversial and not fitfully clarified which autograft provides the best clinical outcome [23, 44, 45]. As evidenced by the funnel plots, low level of heterogeneity was observed. The assumptions through the equation for global linearity via the Wald test were refused, and the final result detected similarity between the autografts in terms of clinical scores of interests.
With regard to joint laxity, Lachman and Pivot shift tests were analysed as manual; the arthrometer KT-1000 and KT-2000 were used as an instrumental test to evaluate joint laxity. Reducing the articular laxity after an ACL rupture is one of the main objectives of surgery [46, 47]. In short term, joint laxity compromises the articular forces distribution, increasing the tendency to acute sprains and soft tissue lesions. Laxity can lead to articular degenerative changes such as osteoarthritis in the long term [48,49,50]. As evidenced by the funnel plots, low level of heterogeneity was observed. The assumptions through the equation for global linearity via the Wald test were refused, and the final result detected similarity between the autografts in terms of clinical scores of interests.
As far as stability is concerned, some biomechanical studies support the use of the QT autograft [11, 51]. Anatomical evidence states that QT is 50% thicker than the PT, providing an optimal stability of femoral condyles to the tibial plateau [52]. The PT autograft is considered the best choice in terms of its biomechanical properties and reduced revision rate [53]. However, the higher donor site morbidity (AKP) and the extension strength deficit led several surgeons to choose the HT autograft [54, 55]. Concern about the HT autograft is the flexion strength deficit in isokinetic testing [56,57,58,59]. Previous studies comparing the QT versus PT found a decreased incidence of donor site morbidity in the QT group [25, 33]. Several studies agree that HT autograft resulted in higher failure rate. Since the activation of the hamstring tendon reduces the load of the ACL providing knee stability [60, 61], its integrity may support the knee in valgus pivoting sport activities [62, 63], preventing autograft failure. In the present analysis, the use of QT grafts scored better in terms of both AKP with respect to the PT autograft and failure rate with respect to the HT autograft. These observations support the current use of QT for revision procedures but also improve future prospective as primary autograft.
The present study has some limitations. First, there are a limited number of eligible studies included. This is explained by the fact that the QT autograft procedure is still preliminary and not widespread. In support of this, our encouraging results should stimulate further studies, implementing the evidence of this procedure, the number of patients and the duration of follow-up. Moreover, the studies included provide a low level of evidence. In fact, there were eight retrospective cohort studies, impacting negatively to the overall evidence. Further studies should improve the scientific evidence, providing also a randomization method, thus reducing the risk of publication’s bias and the level of heterogeneity. The strength of the present study may be represented by the good baseline comparability and decent homogeneity of the results. Even though the level of evidence of this study is low, it provides a good set-up and analysis of the results.
Conclusion
Quadriceps tendon autograft may represent a feasible option for primary ACL reconstruction. This autograft reported a lower rate of failure compared to both PT and HT grafts. Moreover, a reduced rate of anterior knee pain compared to the PT autograft has been observed. The analysis of joint laxity and clinical scores found comparability among the autografts. Orthopedic surgeon should consider these results in light of the evidence and limitations of this Bayesian network meta-analysis.
Change history
21 June 2021
A Correction to this paper has been published: https://doi.org/10.1007/s00590-021-03028-7
References
Mall NA, Chalmers PN, Moric M et al (2014) Incidence and trends of anterior cruciate ligament reconstruction in the United States. Am J Sports Med 42:2363–2370
Filbay SR, Grindem H (2019) Evidence-based recommendations for the management of anterior cruciate ligament (ACL) rupture. Best Pract Res Clin Rheumatol 33(1):33–47. https://doi.org/10.1016/j.berh.2019.01.018
Achtnich A, Metzlaff S, Zantop T (2013) Technique of anatomical footprint reconstruction of the ACL with oval tunnels and medial portal aimers. Arch Orthop Trauma Surg 133(6):827–833
Legnani C, Ventura A, Terzaghi C, Borgo E, Albisetti W (2010) Anterior cruciate ligament reconstruction with synthetic grafts. a review of literature. Int Orthop 34:465–471
Pinczewski LA, Lyman J, Salmon LJ, Russell VJ, Roe J, Linklater J (2007) A 10-year comparison of anterior cruciate ligament reconstructions with hamstring tendon and patellar tendon autograft: a controlled, prospective trial. Am J Sports Med 35(4):564–574. https://doi.org/10.1177/0363546506296042
Duquin T, Wind W, Fineberg M, Smolinski R, Buyea C (2009) Current trends in anterior cruciate ligament reconstruction. Knee Surg 22:7–12
Ejerhed L, Kartus J, Sernert N, Kohler K, Karlsson J (2003) Patellar tendon or semitendinosus tendon autografts for anterior cruciate ligament reconstruction? A prospective randomized study with a two-year follow-up. Am J Sports Med 31:19–25
DeAngelis JP, Fulkerson JP (2007) Quadriceps tendon—a reliable alternative for reconstruction of the anterior cruciate ligament. Clin Sports Med 26:587–596
Romanini E, D’Angelo F, Masi SD et al (2010) Graft selection in arthroscopic anterior cruciate ligament reconstruction. J Orthop Traumatol 11:211–219
Sasaki N, Farraro KF, Kim KE, Woo SL (2014) Biomechanical evaluation of the quadriceps tendon autograft for anterior cruciate ligament reconstruction: a cadaveric study. Am J Sports Med 42(3):723–730. https://doi.org/10.1177/0363546513516603
Harris NL, Smith D, Lamoreaux L, Purnell M (1997) Central quadriceps tendon for anterior cruciate ligament reconstruction. Part I: morphometric and biomechanical evaluation. Am J Sports Med 25:23–28
Hutton B, Salanti G, Caldwell DM, Chaimani A, Schmid CH, Cameron C, Ioannidis JP, Straus S, Thorlund K, Jansen JP, Mulrow C, Catala-Lopez F, Gotzsche PC, Dickersin K, Boutron I, Altman DG, Moher D (2015) The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med 162(11):777–784. https://doi.org/10.7326/M14-2385
Howick J CI, Glasziou P, Greenhalgh T, Heneghan C, Liberati A, Moschetti I, Phillips B, Thornton H, Goddard O, Hodgkinson M (2011) The 2011 Oxford levels of evidence. oxford centre for evidence-based medicine. Available at https://www.cebmnet/indexaspx?o=5653
Irrgang JJ, Anderson A, Boland AL et al (2001) Development and valida- tion of the international knee documentation committee subjective knee form. Am J Sports Med 29:600–613
Lysholm J, Gillquist J (1982) Evaluation of knee ligament surgery results with special emphasis on use of a scoring scale. Am J Sports Med 10(3):150–154
Briggs KK, Lysholm J, Tegner Y, Rodkey WG, Kocher MS, Steadman JR (2009) The reliability, validity, and responsiveness of the Lysholm score and Tegner activity scale for anterior cruciate ligament injuries of the knee: 25 years later. Am J Sports Med 37(5):890–897. https://doi.org/10.1177/0363546508330143
Arneja S, Leith J (2009) Review article: Validity of the KT-1000 knee ligament arthrometer. J Orthop Surg (Hong Kong) 17(1):77–79. https://doi.org/10.1177/230949900901700117
Paine R, Lowe W (2012) Comparison of Kneelax and KT-1000 knee ligament arthrometers. J Knee Surg 25(2):151–154
Aglietti P, Giron F, Buzzi R, Biddau F, Sasso F (2004) Anterior cruciate ligament reconstruction: bone-patellar tendon-bone compared with double semitendinosus and gracilis tendon grafts. A prospective, randomized clinical trial. J Bone Joint Surg Am 86(10):2143–2155
Akoto R, Albers M, Balke M, Bouillon B, Hoher J (2019) ACL reconstruction with quadriceps tendon graft and press-fit fixation versus quadruple hamstring graft and interference screw fixation—a matched pair analysis after one year follow up. BMC Musculoskelet Disord 20(1):109. https://doi.org/10.1186/s12891-019-2499-y
Barenius B, Nordlander M, Ponzer S, Tidermark J, Eriksson K (2010) Quality of life and clinical outcome after anterior cruciate ligament reconstruction using patellar tendon graft or quadrupled semitendinosus graft: an 8-year follow-up of a randomized controlled trial. Am J Sports Med 38(8):1533–1541. https://doi.org/10.1177/0363546510369549
Cavaignac E, Coulin B, Tscholl P, Nik Mohd Fatmy N, Duthon V, Menetrey J (2017) Is quadriceps tendon autograft a better choice than hamstring autograft for anterior cruciate ligament reconstruction? A comparative study with a mean follow-up of 3.6 years. Am J Sports Med 45(6):1326–1332. https://doi.org/10.1177/0363546516688665
Drogset JO, Strand T, Uppheim G, Odegard B, Boe A, Grontvedt T (2010) Autologous patellar tendon and quadrupled hamstring grafts in anterior cruciate ligament reconstruction: a prospective randomized multicenter review of different fixation methods. Knee Surg Sports Traumatol Arthrosc 18(8):1085–1093. https://doi.org/10.1007/s00167-009-0996-5
Feller JA, Webster KE, Gavin B (2001) Early post-operative morbidity following anterior cruciate ligament reconstruction: patellar tendon versus hamstring graft. Knee Surg Sports Traumatol Arthrosc 9(5):260–266. https://doi.org/10.1007/s001670100216
Geib TM, Shelton WR, Phelps RA, Clark L (2009) Anterior cruciate ligament reconstruction using quadriceps tendon autograft: intermediate-term outcome. Arthroscopy 25(12):1408–1414. https://doi.org/10.1016/j.arthro.2009.06.004
Gorschewsky O, Klakow A, Putz A, Mahn H, Neumann W (2007) Clinical comparison of the autologous quadriceps tendon (BQT) and the autologous patella tendon (BPTB) for the reconstruction of the anterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc 15(11):1284–1292. https://doi.org/10.1007/s00167-007-0371-3
Han HS, Seong SC, Lee S, Lee MC (2008) Anterior cruciate ligament reconstruction : quadriceps versus patellar autograft. Clin Orthop Relat Res 466(1):198–204. https://doi.org/10.1007/s11999-007-0015-4
Haner M, Bierke S, Petersen W (2016) Anterior cruciate ligament revision surgery: ipsilateral quadriceps versus contralateral semitendinosus-gracilis autografts. Arthroscopy 32(11):2308–2317. https://doi.org/10.1016/j.arthro.2016.03.020
Hart R, Kucera B, Safi A (2010) Hamstring versus quadriceps tendon graft in double-bundle anterior cruciate ligament reconstruction. Acta Chir Orthop Traumatol Cech 77(4):296–303
Kim SJ, Kumar P, Oh KS (2009) Anterior cruciate ligament reconstruction: autogenous quadriceps tendon-bone compared with bone-patellar tendon-bone grafts at 2-year follow-up. Arthroscopy 25(2):137–144. https://doi.org/10.1016/j.arthro.2008.09.014
Kim SJ, Lee SK, Choi CH, Kim SH, Kim SH, Jung M (2014) Graft selection in anterior cruciate ligament reconstruction for smoking patients. Am J Sports Med 42(1):166–172. https://doi.org/10.1177/0363546513505191
Lee JK, Lee S, Lee MC (2016) Outcomes of anatomic anterior cruciate ligament reconstruction: bone-quadriceps tendon graft versus double-bundle hamstring tendon graft. Am J Sports Med 44(9):2323–2329. https://doi.org/10.1177/0363546516650666
Lund B, Nielsen T, Fauno P, Christiansen SE, Lind M (2014) Is quadriceps tendon a better graft choice than patellar tendon? a prospective randomized study. Arthroscopy 30(5):593–598. https://doi.org/10.1016/j.arthro.2014.01.012
Maletis GB, Cameron SL, Tengan JJ, Burchette RJ (2007) A prospective randomized study of anterior cruciate ligament reconstruction: a comparison of patellar tendon and quadruple-strand semitendinosus/gracilis tendons fixed with bioabsorbable interference screws. Am J Sports Med 35(3):384–394. https://doi.org/10.1177/0363546506294361
Martin-Alguacil JL, Arroyo-Morales M, Martin-Gomez JL, Monje-Cabrera IM, Abellan-Guillen JF, Esparza-Ros F, Lozano ML, Cantarero-Villanueva I (2018) Strength recovery after anterior cruciate ligament reconstruction with quadriceps tendon versus hamstring tendon autografts in soccer players: a randomized controlled trial. Knee 25(4):704–714. https://doi.org/10.1016/j.knee.2018.03.011
Mohtadi N, Chan D, Barber R, Oddone Paolucci E (2015) A randomized clinical trial comparing patellar tendon, hamstring tendon, and double-bundle acl reconstructions: patient-reported and clinical outcomes at a minimal 2-year follow-up. Clin J Sport Med 25(4):321–331. https://doi.org/10.1097/JSM.0000000000000165
Runer A, Wierer G, Herbst E, Hepperger C, Herbort M, Gfoller P, Hoser C, Fink C (2018) There is no difference between quadriceps- and hamstring tendon autografts in primary anterior cruciate ligament reconstruction: a 2-year patient-reported outcome study. Knee Surg Sports Traumatol Arthrosc 26(2):605–614. https://doi.org/10.1007/s00167-017-4554-2
Sofu H, Sahin V, Gursu S, Yildirim T, Issin A, Ordueri M (2013) Use of quadriceps tendon versus hamstring tendon autograft for arthroscopic anterior cruciate ligament reconstruction: a comparative analysis of clinical results. Eklem Hastalik Cerrahisi 24(3):139–143. https://doi.org/10.5606/ehc.2013.31
Taylor DC, DeBerardino TM, Nelson BJ, Duffey M, Tenuta J, Stoneman PD, Sturdivant RX, Mountcastle S (2009) Patellar tendon versus hamstring tendon autografts for anterior cruciate ligament reconstruction: a randomized controlled trial using similar femoral and tibial fixation methods. Am J Sports Med 37(10):1946–1957. https://doi.org/10.1177/0363546509339577
Todor A, Nistor DV, Caterev S (2019) Clinical outcomes after ACL reconstruction with free quadriceps tendon autograft versus hamstring tendons autograft. A retrospective study with a minimal follow-up two years. Acta Orthop Traumatol Turc 53(3):180–183. https://doi.org/10.1016/j.aott.2019.03.004
Wipfler B, Donner S, Zechmann CM, Springer J, Siebold R, Paessler HH (2011) Anterior cruciate ligament reconstruction using patellar tendon versus hamstring tendon: a prospective comparative study with 9-year follow-up. Arthroscopy 27(5):653–665. https://doi.org/10.1016/j.arthro.2011.01.015
Zaffagnini S, Marcacci M, Lo Presti M, Giordano G, Iacono F, Neri MP (2006) Prospective and randomized evaluation of ACL reconstruction with three techniques: a clinical and radiographic evaluation at 5 years follow-up. Knee Surg Sports Traumatol Arthrosc 14(11):1060–1069. https://doi.org/10.1007/s00167-006-0130-x
Agel J, LaPrade RF (2009) Assessment of differences between the modified cincinnati and international knee documentation committee patient outcome scores: a prospective study. Am J Sports Med 37(11):2151–2157. https://doi.org/10.1177/0363546509337698
Sajovic M, Stropnik D, Skaza K (2018) Long-term comparison of semitendinosus and gracilis tendon versus patellar tendon autografts for anterior cruciate ligament reconstruction: a 17-year follow-up of a randomized controlled trial. Am J Sports Med 46(8):1800–1808. https://doi.org/10.1177/0363546518768768
Webster KE, Feller JA, Hartnett N, Leigh WB, Richmond AK (2016) Comparison of patellar tendon and hamstring tendon anterior cruciate ligament reconstruction: a 15-year follow-up of a randomized controlled trial. Am J Sports Med 44(1):83–90. https://doi.org/10.1177/0363546515611886
Ryan J, Magnussen RA, Cox CL, Hurbanek JG, Flanigan DC, Kaeding CC (2014) ACL reconstruction: do outcomes differ by sex? A systematic review. J Bone Joint Surg Am 96(6):507–512. https://doi.org/10.2106/JBJS.M.00299
Rezende FC, de Moraes VY, Martimbianco AL, Luzo MV, da Silveira Franciozi CE, Belloti JC (2015) Does combined intra- and extraarticular acl reconstruction improve function and stability? A Meta-analysis Clin Orthop Relat Res 473(8):2609–2618. https://doi.org/10.1007/s11999-015-4285-y
Thorlund JB, Creaby MW, Wrigley TV, Metcalf BR, Bennell KL (2014) Knee joint laxity and passive stiffness in meniscectomized patients compared with healthy controls. Knee 21(5):886–890. https://doi.org/10.1016/j.knee.2014.06.001
Dejour H, Walch G, Deschamps G, Chambat P (2014) Arthrosis of the knee in chronic anterior laxity. Orthop Traumatol Surg Res 100(1):49–58. https://doi.org/10.1016/j.otsr.2013.12.010
Miyazaki T, Uchida K, Sato M, Watanabe S, Yoshida A, Wada M, Shimada S, Kuiper JH, Baba H (2012) Knee laxity after staircase exercise predicts radiographic disease progression in medial compartment knee osteoarthritis. Arthritis Rheum 64(12):3908–3916. https://doi.org/10.1002/art.34662
Stäubli HU, Schatzmann L, Brunner P, Rincón L, Nolte LP (1996) Quadriceps tendon and patellar ligament: cryosectional anatomy and structural properties in young adults. Knee Surg Sports Traumatol Arthrosc 4:100–110
Fulkerson JP, Langeland R (1995) An alternative cruciate reconstruction graft: the central quadriceps tendon. Arthroscopy 11:252–254
Reinhardt KR, Hetsroni I, Marx RG (2010) Graft selection for anterior cruciate ligament reconstruction: a level I systematic review comparing failure rates and functional outcomes. Orthop Clin North Am 41(2):249–262. https://doi.org/10.1016/j.ocl.2009.12.009
Feller JA, Webster KE (2003) A randomized comparison of patellar tendon and hamstring tendon anterior cruciate ligament reconstruction. Am J Sports Med 31(4):564–573. https://doi.org/10.1177/03635465030310041501
Walden M, Hagglund M, Magnusson H, Ekstrand J (2011) Anterior cruciate ligament injury in elite football: a prospective three-cohort study. Knee Surg Sports Traumatol Arthrosc 19(1):11–19. https://doi.org/10.1007/s00167-010-1170-9
Ardern CL, Webster KE, Taylor NF, Feller JA (2010) Hamstring strength recovery after hamstring tendon harvest for anterior cruciate ligament reconstruction: a comparison between graft types. Arthroscopy 26(4):462–469. https://doi.org/10.1016/j.arthro.2009.08.018
Burks RT, Crim J, Fink BP, Boylan DN, Greis PE (2005) The effects of semitendinosus and gracilis harvest in anterior cruciate ligament reconstruction. Arthroscopy 21(10):1177–1185. https://doi.org/10.1016/j.arthro.2005.07.005
Nakamura N, Horibe S, Sasaki S, Kitaguchi T, Tagami M, Mitsuoka T, Toritsuka Y, Hamada M, Shino K (2002) Evaluation of active knee flexion and hamstring strength after anterior cruciate ligament reconstruction using hamstring tendons. Arthroscopy 18(6):598–602
Keays SL, Bullock-Saxton J, Keays AC, Newcombe P (2001) Muscle strength and function before and after anterior cruciate ligament reconstruction using semitendonosus and gracilis. Knee 8(3):229–234
Renstrom P, Arms SW, Stanwyck TS, Johnson RJ, Pope MH (1986) Strain within the anterior cruciate ligament during hamstring and quadriceps activity. Am J Sports Med 14(1):83–87. https://doi.org/10.1177/036354658601400114
Withrow TJ, Huston LJ, Wojtys EM, Ashton-Miller JA (2008) Effect of varying hamstring tension on anterior cruciate ligament strain during in vitro impulsive knee flexion and compression loading. J Bone Joint Surg Am 90(4):815–823. https://doi.org/10.2106/JBJS.F.01352
Alentorn-Geli E, Myer GD, Silvers HJ, Samitier G, Romero D, Lazaro-Haro C, Cugat R (2009) Prevention of non-contact anterior cruciate ligament injuries in soccer players. Part 1: mechanisms of injury and underlying risk factors. Knee Surg Sports Traumatol Arthrosc 17(7):705–729. https://doi.org/10.1007/s00167-009-0813-1
Kremen TJ, Polakof LS, Rajaee SS, Nelson TJ, Metzger MF (2018) The effect of hamstring tendon autograft harvest on the restoration of knee stability in the setting of concurrent anterior cruciate ligament and medial collateral ligament injuries. Am J Sports Med 46(1):163–170. https://doi.org/10.1177/0363546517732743
Funding
Open Access funding enabled and organized by Projekt DEAL. No external source of funding was used.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
For this type of study, informed consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised due to a retrospective Open Access order.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Migliorini, F., Eschweiler, J., Mansy, Y.E. et al. Quadriceps tendon autograft for primary ACL reconstruction: a Bayesian network meta-analysis. Eur J Orthop Surg Traumatol 30, 1129–1138 (2020). https://doi.org/10.1007/s00590-020-02680-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00590-020-02680-9