
Abstract
Purpose
Our aim was to develop a nationwide, computer-based, Spine Register (FinSpine) for monitoring surgical activity, quality of surgery, long-term outcomes, and effectiveness of treatment. In this paper, we describe our experiences in the development and implementation of the register.
Methods
The register was developed by a steering group, consisting of orthopedic surgeons and neurosurgeons from the whole country. We strived to develop a register which would be in active use by spine surgeons and enable collection of Patient Reported Outcome and Experience Measures (PROMs and PREMs) automatically and prospectively. We are actively promoting the use of the register in order to gain a nationwide coverage and achieve high response-rates from both surgeons and patients.
Results
The use of FinSpine started in 2016 and it has been granted continuous funding from the Finnish Institute for Health and Welfare from the 1st of January 2023 onwards. Currently the register is used by 19/23 (83%) public hospitals and the use is expanding to private hospitals as well. The response-rate of surgeons is currently 80%. The response-rate of patients is on average 56% but reaches up to 90% in hospitals using register-coordinators.
Conclusion
The use of FinSpine is increasing. By gaining a larger coverage and completeness, the data can be used for research purposes which we believe will influence decision making and ultimately improve the outcomes and quality of life of the patients. Comparison with other national spine registers is possible, since FinSpine includes similar baseline characteristics and outcome measures (e.g., ODI, EQ-5D, VAS).
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Spine surgery has become a major subspeciality within orthopedic surgery and neurosurgery, covering a variety of different indications including degenerative disorders, traumas, tumors, deformities and infections. Over the last decades there has been an increase in the number of spine surgery performed [1,2,3,4]. During this time the availability of imaging has increased considerably, and there has been an excessive development of new instruments and devices. Especially for degenerative disorders the improvements in imaging have also facilitated the development of minimally invasive techniques [5].
Degenerative disorders are by far the most common indications for surgery (comprising up to 90% of all procedures in large population-based hospitals). While outcome is generally good [6,7,8,9] and evidence of improved quality of life (QoL) is gradually increasing [10], the surgery of degenerative disorders might also be the most likely to express variations in indications and outcome. Within or between countries, variations may occur in the rate of surgeries, patient selection (including eligibility of older patients and patients with less severe symptoms), operating techniques (including use of implants) and timing of surgery [11, 12]. Variations in outcome are likely when it comes to utilization of more complex and novel techniques, where the results from the specialized centers involved in the developing process, do not necessarily translate into generalizable results.
In order to obtain comprehensive and reliable data about the surgical activity and the long-term outcomes, a comprehensive, systematic, register-based follow-up is necessary. This has earlier been performed on a high level, e.g., in Norway by the NORspine[13] and Sweden by the SweSpine [14] registers that have provided important results which have influenced clinical practice [15]. With transparent register-based benchmarking, it could be possible to create more uniform standards among the surgeons and hopefully improve the outcomes and QoL of the patients. The real-world evidence from registers complements the evidence obtained from randomized controlled trials.
There is an increasing recognition of the importance of combining clinical outcomes with Patient Reported Outcome Measures (PROMs) and Patient Reported Experience Measures (PREMs) in order to achieve a more complete understanding of the impact and effectiveness of the treatment [16, 17]. Patients evaluate their own health, quality of life and functional status associated with the treatment they have received [18]. Thoroughly evaluated and effective interventions are more likely to have an advantageous position when prioritizing resources.
In this paper, we focus on describing the development and design of the FinSpine register. We also address the current state of nationwide implementation, compliance among surgeons to use the register and share our experience how to achieve higher response-rates from patients. Furthermore, we describe a validation process comparing the procedure codes in the FinSpine register with the same data pooled from the hospitals’ Electronic Patient Records (EPRs) and show some preliminary results in order to illustrate the potential of the register.
Development and implementation of the register
Finland is a Nordic country with a population of 5.5 million. We have a wide tax funded, public health care system accessible for all citizens. Around 8500 spine surgical procedures are performed annually.
Influenced by the other Nordic countries, the idea of developing a Finnish Spine Register (FinSpine) was introduced already when the Finnish Society of Spine Surgery was founded in 2001. The development of FinSpine begun in 2014 and soon it was decided that a steering group should be formed, consisting of both orthopedic surgeons and neurosurgeons from all Hospital districts of the country. The development of the register has been done at the regular meetings of the steering group 4 times a year.
From the very beginning there was clear that the register was going to be computer-based. This would enable:
-
(1)
Automatic data integration from Electronic Patient Records (EPRs).
-
(2)
Higher compliance from surgeons to reliably fill the register with the necessary specifications of the surgeries and possible complications.
-
(3)
Surgeons to easily discover the patients for whom data is missing.
-
(4)
Real-time output of register data.
-
(5)
Patients to report outcome and experience measures online.
A suitable collaborator from the field of medical information technology was recruited. This company (BCBMedical) had the best technical knowledge about developing registers for healthcare in Finland. The collaboration has been good, the software has been updated at least 2 times per year according to the propositions of the steering group.
After completing the design of FinSpine our foremost goal is to validate the data and to gain a nationwide coverage of hospitals using FinSpine (currently 19/23 public hospitals). We also strive to have a high compliance among surgeons and to attain high response-rates from the patients to the PROM and PREM questionnaires. We believe that promoting the use of FinSpine this is best done by educating users at annual meetings of the Finnish Society of Spine Surgery and at dedicated FinSpine user symposiums. We have also incorporated a Report tool function into the register software which enables every surgeon to easily access the register data of their own hospital. We believe that this capability to observe one’s own results and gain real-time feedback will also motivate the surgeons to use FinSpine.
Collaboration with the Finnish institute for health and welfare
In 2018 the Finnish Institute for Health and Welfare (THL), an independent expert agency working under the Ministry of Social Affairs and Health, striving to monitor, and develop measures to promote the well-being and health of the population in Finland, started a pilot for national healthcare registers. It was proposed that the 9 most significant registers would gain a national status.
FinSpine received this lawful national status and will receive government funding from 1st of January 2023 onwards. Furthermore, THL will pool and store the FinSpine data from all the participating hospitals and provide its expertise in data handling, making it possible to easily access the entire national data. Researchers can acquire access the national data by making an application to FinData, (the Social and Health Data Permit Authority operating under the guidance of the Ministry of Social Affairs and Health). The legislation is straightforward, and it is easy to compare data from different hospitals. Moreover, the national data is also accessible for researchers from outside the spine surgery community as well. We have however established a board of advisors from within the spine surgeon community to guide with the interpretation of the data and to facilitate researchers with similar interests to collaborate. Due to the collaboration with THL it is also easier to combine the register data with other national registers such as ones collecting data on drug purchase and sick leaves.
Design of the register
In Fig. 1, we show an overview of the register. Technically the register is accessible for all authorized users via a link from the Electric Patient Record software, which varies between different hospitals. The FinSpine software opens in a web browser.

Overview of the FinSpine register showing how data input is derived A automatically from medical records, B from surgeons filling specific information and C patients reporting PROMs and PREMs. THL is the Finnish Institute for Health and Welfare
Data input
A file for the patient is created real-time into the register automatically when the register software derives information that a patient is undergoing a procedure with a spine specific procedure code. In order for the data to be incorporated in the outcome reports, the register receives further input from the operating room data system. Hereby, the analysis does not include patients, or information from patients who were not eventually operated.
Each patient receives the following input of data:
-
(1)
Basic information of the surgical procedures (e.g., date, time, surgeon) automatically from EPRs
-
(2)
Specific information of the surgical procedures, filled by the surgeon (Table 1)
-
(3)
Implants that have been used (filled automatically or by OR nurse)
-
(4)
In-hospital complications and length of hospitalization (filled by the surgeon, see Table 1)
-
(5)
Later complications (filled by the surgeon if encountered, see Table 1)
-
(6)
Responses to PROM and PREM questionnaires filled by patients (Table 2)
The 3 steps of data the surgeon needs to fill is presented in Table 1, we have been careful only to include data we believe is relevant. On the other hand, for the listing of procedures and diseases, we have been much more detailed than what the ICD codes and procedure codes would provide. This listing corresponds with the nomenclature and definitions frequently used in scientific spine surgery publications other spine registers.
The PROMs and PREMs are presented in detail in Table 2. To obtain PROMs and PREMs, patients automatically receive a link to these questionnaires via SMS or e-mail. The link to the preoperative questionnaires is sent as soon as the operation is planned (max 60 days preoperatively) and it expires on the day of the operation. The postoperative links are sent 30 days prior to each postoperative time point (3 months, 1 year, 2 years, 5 years and 10 years) and expire 30 days past each time point. A reminder is sent 30 days after the initial link to the patients that have not responded. If a patient is re-operated within 30 days from the initial operation the time points of the following questionnaires will be according to the time points of the initial operation. However, if a re-operation is performed after 30 days, the patient will receive postoperative questionnaires with time points in reference to the last operation and will not receive duplicates from the initial operation.
Data output
The content of the register can be displayed and analyzed in different ways (Table 3).
-
(1)
The “Patient sheet” of individual patients, displays all details of the patient’s spine surgeries and all the responses to the PROM and PREM questionnaires. Data input by surgeons is also performed in the “Patient sheet” viewing.
-
(2)
The “Patient list” view enables users to easily view and sort all the patients from their own hospital by a simple set of variables (e.g., Patient name, Main diagnosis, Main procedure, Operating surgeon).
-
(3)
By using the “Report tool” function, the user can create real-time charts or plots of 20 different outcome variables (e.g., different surgeries performed, intraoperative complications, VAS, ODI, NDI), which can be filtered with 22 filters (e.g., Smoking (Y/N), Sex (F/M), Age (Range), Surgeon (Name)). This is an easy way to get insight to one’s own work and compare results with other surgeons in the same hospital (Fig. 2). Statistical testing is possible by extracting the data and using a regular statistical analysis program. For nation-wide research, the complete national register data can be accessed by making an application to FinData.

Screenshot from the Report tool in FinSpine. The Report tool can be used by surgeons to view their own results. This particular histogram displays the answers to 4 PREM questions regarding postoperative satisfaction of one particular surgeon’s patients undergoing primary spine surgery. Data can be further filtered by using filters in the right-sided column (See Table 3 for listing of filters and outcome report options)
Ethical issues and data security
Data handling in hospitals and at a national level is done according to national and EU guidelines. The data is securely protected, the professionals access the register upon signing into the EPRs by using an ID and a password. Data filled by patients is GDPR compliant.
Since the PROM and PREM questionnaires are regarded general follow-up of clinical practice, no additional informed consent is needed from the patient. The patients have the right to refuse to receive the questionnaires. In order to access the national data the researcher needs to make an application to FinData, which provides expertise in data handling and data security and assures that the secondary use of data is in concordance to EU legislation and GDPR.
Validation
Validation of FinSpine against “hospital discharge register” (HILMO)
THL maintains a “hospital discharge register” (HILMO) to which all contacts, treatment periods and procedures in the whole country are registered from the hospitals’ EPRs. The HILMO register is considered highly reliable when it comes to describing these basic demographics of the Finnish health care.
In 2019 we compared all spine procedure codes from 2017–2018 in FinSpine with the ones in the HILMO register. Our hypothesis was that the FinSpine data could prove to be more accurate (since the input is generated only when both the procedure code and the trigger from the operating room data system coexist). The validation was then repeated in opposite direction.
Our hypothesis proved to be correct. The FinSpine register data proved to be 100% accurate, in terms that no patients were found to be missing compared to HILMO. HILMO on the other hand included unnecessary duplets of patient procedures, which distorts the overall statistics. This can be explained by the fact that the input to the HILMO register can be done twice if for example the patient awaiting surgery moves from one hospital to another. This validation will be repeated.
Intra- and interobserver validation
Intra- and interobserver validation has started and will be the subject of our future paper. We want to assess how consistent the selection of, e.g., diagnosis and procedures is among surgeons using the register.
Utility and results
The development of the register has been successful and has resulted in a computer based, user-friendly system, that has been implemented into use in the foremost departments performing spine surgery in Finland.
The first hospitals started using the register in 2016, the number of participating hospitals significantly increased in 2017 with the initiation of the collection of PROMs and PREMs. Currently 19/23 (83%) public hospitals performing spine surgery, use FinSpine and the coverage is further expanding into private hospitals, with the first ones starting to use FinSpine in the end of 2022. 7553 surgeries were included into FinSpine during 2022, which accounts for 86% of all spine surgeries performed in the whole country last year and over 90% of the surgeries performed in public hospitals.
Compliance of surgeons to use FinSpine has been steadily increasing, in 2022 80% of the cases in the register included data input from the surgeon.
The response-rates of the patients have been increasing during the last years (Fig. 3), reaching 54–58% at all the time points. However, for the patient reported data to be useful, it is necessary to obtain as high response-rates as possible. We have enhanced this by including the option of collecting responses on paper-based questionnaires and in-hospital iPads. Furthermore, we have found that up to 90% preoperative and 80% postoperative response-rates have been achieved in hospitals that have been able to hire register coordinators, who contact the patients by phone and remind the about the questionnaires and can systematically send them paper-based questionnaires if the responses are lacking.

The development of the response rate for the PROM and PREM questionnaires in the FinSpine register. The baseline data has increased from < 30% in 2017 to 58% in 2021. The same is observed also for 3 mos and 12 mos timepoints
Examples of outcomes
In Table 4, we show the cumulative data from 2017 to the present, showing the 5 most common diagnosis for Lumbar and Cervical surgeries in FinSpine. For lumbar spine the 5 most common diagnosis showed to account for 84,2% of all lumbar surgeries (16700/19834). For cervical spine the 5 most common diagnosis accounted for 87,6% of all cervical surgeries (5142/6178).
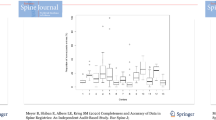
In order to demonstrate the utility of the follow-up PROM data, we display in Fig. 4 the favorable progression of the ODI score of all patients undergoing surgery for lumbar spinal stenosis at 18 different hospitals.

The pre- and postoperative (3 mos, 12 mos, 24 mos) ODI Scores in the FinSpine register for all patients undergoing surgery for lumbar spinal stenosis is shown for each hospital. In the lower right corner is the combined overall result. An overall of 9129 patients were operated, case-mix has not been taken into account
Discussion
Spine surgery exhibits a lot of variations, e.g., in operation rates within and between different countries [11, 12]. In order to achieve more uniform standards and eventually improve the outcome of the patients, it is important to comprehensively monitor the surgical activity, quality of surgery and long-term outcomes and to be able to display these results transparently. The well-known, SweSpine [14], NORspine [13] and Spine tango [22] are excellent examples of this. The studies using these registers have had a substantial impact on how we treat spine patients [15].
We describe our experience in the development process of the FinSpine register. FinSpine has had influence from the other Nordic registers, we have included similar baseline characteristics and outcome measures (e.g., ODI, EQ-5D, VAS) to make inter-registry comparison possible. A prerequisite for the development of a national register is a common consensus between the leading clinicians on the need and content of the register. A steering group consisting of experienced surgeons working in close contact with both the spine surgery community and the IT-company responsible for the technical development, proved to be a conductive way of working. However, after finishing the designing of the register, continuous work is needed for the implementation of the register and utilization of the data.
During the designing process of the register, we discovered several possible pitfalls and reacted accordingly:
1. Technical solutions can include bugs. Our IT collaborator has been flexible and has skillfully performed their work in order to get the software to work with different computer programs in different departments. All possible wishes in the design could however not be met.
2. Data filled by surgeon can be irrelevant or not valid. We strived to make the dataset the surgeon needs to fill as relevant as possible for our goal. We are in the process of creating example cases which will be used for validation.
3. Data filled by surgeon can be missing or incomplete. The dataset filled by the surgeon can be easily filled (Table 1), as we have discarded data that is in our opinion of secondary importance, and only the most important data is to be recorded. In the “Patient list” view we have a column indicating the cases with missing data. We have strived to teach and motivate the surgeons at annual meetings.
4. Data filled by patients can be missing. Patients receive an electronic link via SMS or e-mail to the PROM questionnaires and a reminder 30 days later. Hospitals have hired full- or part-time coordinators who directly contact the patients, remind them and send paper-based questionnaires if needed. Patients can also give their response while visiting the hospital by using a portable devise (iPad) that connects to the register software.
5. Including data from conservatively treated spine patients.
This data would be imprecise and incomplete since most conservatively treated patients are treated elsewhere. Only patients undergoing surgery are included.
6. Expenses of development.
All participating departments initially needed to acquire funding from the hospitals. We were able to perform this quite easily by backing up each other and by making the importance of the content clear to the hospital board. The large number of participating departments also lowered the expenses.
Technically FinSpine was developed to be computer-based in order for it to be easy to use and in order to automatically send questionnaires to the patents. During the years of use it has become apparent that though patient response-rates have steadily increased the average response-rate of 54–58% is not sufficient for detailed analysis of the results. Therefore, we found it necessary to hire coordinators who contact the patients and if necessary, send patients paper-based questionnaires as well. In hospitals with full-time coordinators response rates of up to 90% preoperatively and 80% postoperatively have been achieved. However, our data does not show a difference in response rates between younger and older patients, but we will do further analysis on which different patient related factors can affect the response rate. With government funding we hope to introduce coordinators to the hospitals still lacking one.
Better compliance among surgeons has been achieved by motivating and educating the surgeons regularly at annual meetings of the Finnish Society of Spine Surgery and at dedicated FinSpine symposiums. We also believe that presenting results is a way to motivate the users, e.g., by displaying inter-hospital variations in the completeness of the register to surgeons and coordinators. Surgeons can also acquire real-time feedback by using the Report tool of FinSpine. Surgeons are also compelled to fill information regarding possible in-hospital and later complications meticulously. We do not know yet whether there is inconsistency between surgeons in reporting possible complications.
Validation of the variables within the register has been started. So far, we found that the FinSpine register data included all the cases reported to the national hospital discharge register, with no patients missing. We are currently performing an intra- and interobserver validation to assess how consistent the use of FinSpine is. Accumulating national data, collected identically in each hospital allows valid benchmarking between hospitals. On the THL website, the first report regarding outcome after lumbar discectomy will be displayed, depicting intraoperative complications and the postoperative VAS reported by the patients for from the different hospitals.
In modern medicine there is an increasing interest in studying the effectiveness of care of different disorders. The assessment of real-life effectiveness and real-life cost-effectiveness requires the existence of patient group specific quality registers which document data on patients, interventions and outcomes in ordinary health and social care [19,20,21]. We believe that data from national spine registers will influence decision-making and improve the outcomes and QoL of the patients.
Thoroughly evaluated and effective interventions are likely to confirm their position in future. Displaying reliable and transparent reports of register data is set to add confidence toward spine surgery. Spine surgeons in different countries are urged to develop similar registers.
Conclusions
FinSpine has established its position in the Finnish spine surgery community, while further work to achieve higher response-rates and even wider coverage is being done. We believe that FinSpine could be as influential as the other national spine registers. Utilization of FinSpine data in order to assess quality and perform scientific research is already being done. First reports of outcomes will be displayed on the THL website. FinSpine can serve as a reference for national or international studies. In future, we hope to collaborate with other national registers and conduct inter-register analysis.
References
Grøvle L, Fjeld OR, Haugen AJ, Helgeland J, Småstuen MC, Solberg TK, Zwart JA, Grotle M (2019) The rates of LSS surgery in norwegian public hospitals: a threefold increase from 1999 to 2013. Spine (Phila Pa 1976) 44(6):E372–E378. https://doi.org/10.1097/BRS.0000000000002858. (PMID: 30234811)
Kotkansalo A, Leinonen V, Korajoki M, Salmenkivi J, Korhonen K, Malmivaara (2019) Surgery for degenerative cervical spine disease in Finland, 1999–2015. A. Acta Neurochir (Wien) 161(10):2147–2159. https://doi.org/10.1007/s00701-019-03958-6. (Epub 2019 Jun 1PMID: 31154519)
Ponkilainen VT, Huttunen TT, Neva MH, Pekkanen L, Repo JP, Mattila VM (2021) National trends in lumbar spine decompression and fusion surgery in Finland, 1997–2018. Acta Orthop 92(2):199–203. https://doi.org/10.1080/17453674.2020.1839244. (Epub 2020 Oct 27PMID: 33106074)
Kotkansalo A, Leinonen V, Korajoki M, Korhonen K, Rinne J, Malmivaara A (2021) Occurrence, risk factors, and time trends for late reoperations due to degenerative cervical spine disease: a finnish national register study of 19 377 patients operated on between 1999 and 2015. Neurosurgery 88(3):558–573. https://doi.org/10.1093/neuros/nyaa464. (PMID:33372210;PMCID:PMC8133327)
Momin AA, Steinmetz MP (2020) Evolution of minimally invasive lumbar spine surgery. World Neurosurg 140:622–626. https://doi.org/10.1016/j.wneu.2020.05.071. (Epub 2020 May 17.PMID: 32434014 Review)
Lagerbäck T, Fritzell P, Hägg O, Nordvall D, Lønne G, Solberg TK, Andersen MØ, Eiskjær S, Gehrchen M, Jacobs WC, van Hooff ML, Gerdhem P (2019) (2019) Effectiveness of surgery for sciatica with disc herniation is not substantially affected by differences in surgical incidences among three countries: results from the Danish, Swedish and Norwegian spine registries. Eur Spine J 28(11):2562–2571. https://doi.org/10.1007/s00586-018-5768-9. (Epub 2018 Sep 29PMID: 30269234)
Lønne G, Fritzell P, Hägg O, Nordvall D, Gerdhem P, Lagerbäck T, Andersen M, Eiskjaer S, Gehrchen M, Jacobs W, van Hooff ML, Solberg TK (2019) Lumbar spinal stenosis: comparison of surgical practice variation and clinical outcome in three national spine registries. Spine J 19(1):41–49. https://doi.org/10.1016/j.spinee.2018.05.028. (Epub 2018 May 21PMID: 29792994)
Malmivaara A, Slätis P, Heliövaara M, Sainio P, Kinnunen H, Kankare J, Dalin-Hirvonen N, Seitsalo S, Herno A, Kortekangas P, Niinimäki T, Rönty H, Tallroth K, Turunen V, Knekt P, Härkänen T, Hurri H (2007) Surgical or nonoperative treatment for lumbar spinal stenosis? A randomized controlled trial Finnish Lumbar Spinal Research Group. Spine Phila Pa (1976) 32(1):1–8. https://doi.org/10.1097/01.brs.0000251014.81875.6d. (PMID: 17202885)
Slätis P, Malmivaara A, Heliövaara M, Sainio P, Herno A, Kankare J, Seitsalo S, Tallroth K, Turunen V, Knekt P, Hurri H (2011) Long-term results of surgery for lumbar spinal stenosis: a randomised controlled trial. Eur Spine J 20(7):1174–1181. https://doi.org/10.1007/s00586-010-1652-y. (Epub 2011 Jan 15PMID: 2124053)
Hirvonen T, Siironen J, Marjamaa J, Niemelä M, Koski-Palkén A (2020) Anterior cervical discectomy and fusion in young adults leads to favorable outcome in long-term follow-up. Spine J 20(7):1073–1084. https://doi.org/10.1016/j.spinee.2020.03.016. (Epub 2020 Apr 8PMID: 32276052)
Mäntymäki H, Ponkilainen VT, Huttunen TT, Mattila VM (2021) Regional variations in lumbar spine surgery in Finland. Arch Orthop Trauma Surg. https://doi.org/10.1007/s00402-021-04313-0. (PMID: 34971438)
Deyo RA, Mirza SK (2006) Trends and variations in the use of spine surgery. Clin Orthop Relat Res 443:139–146. https://doi.org/10.1097/01.blo.0000198726.62514.75. (PMID:16462438Review)
Austevoll IM, Gjestad R, Brox JI, Solberg TK, Storheim K, Rekeland F, Hermansen E, Indrekvam K, Hellum C (2017) The effectiveness of decompression alone compared with additional fusion for lumbar spinal stenosis with degenerative spondylolisthesis: a pragmatic comparative non-inferiority observational study from the Norwegian Registry for Spine Surgery. Eur Spine J 26(2):404–413. https://doi.org/10.1007/s00586-016-4683-1. (Epub 2016 Jul 15PMID: 27421276)
Strömqvist B, Fritzell P, Hägg O, Jönsson B, SwedishSocietyofSpinalSurgeons (2009) The Swedish spine register: development, design and utility. Eur Spine J 18(Suppl3):294–304. https://doi.org/10.1007/s00586-009-1043-4
Försth P, Michaelsson K, Sanden B (2013) Does fusion improve the outcome after decompressive surgery for lumbar spinal stenosis?: A two-year follow-up study involving 5390 patients. Bone Joint J 95(B7):960–965. https://doi.org/10.1302/0301-620X.95B7.30776
Pekkanen L, Kautiainen H, Ylinen J, Salo P, Häkkinen A (2011) Reliability and validity study of the Finnish version 2.0 of the oswestry disability index. Spine Phila Pa 1976 36(4):332–338. https://doi.org/10.1097/BRS.0b013e3181cdd702. (PMID: 20823785)
Rudolfsen JH, Solberg TK, Ingebrigtsen T, Olsen JA (2020) Associations between utilization rates and patients’ health: a study of spine surgery and patient-reported outcomes (EQ-5D and ODI). BMC Health Serv Res 20(1):135. https://doi.org/10.1186/s12913-020-4968-2. (PMID:32087710FreePMCarticle)
EuroQol Research Foundation (2018) EQ-5D-3L user guide [Online]. Accessed 17 Nov 2019
Malmivaara A (2015) Benchmarking controlled trial-a novel concept covering all observational effectiveness studies. Ann Med 47:332–340
Malmivaara A (2016) Clinical impact research—How to choose experimental or observational intervention study? Ann Med 48:492–495
Malmivaara A (2016) System impact research—increasing public health and health care system performance. Ann Med 48(1–5):33
Fritzell P (2002) Spine Tango Spine registry. Eur Spine J 11(4):301–302. https://doi.org/10.1007/s00586-002-0456-0. (Epub 2002 Jun 28PMID: 12193989)
Acknowledgements
The authors thank Denisa Hirkic (M.Eng.) and her team from BCB Medical for their work in the technical development of the register. The authors are also thankful to the following members of the Finnish Society of Spine Surgery: Jussi Antinheimo (Helsinki), Jarkko Halme (Kuopio), Mikko Kauppinen (Oulu), Pietari Kinnunen (Oulu), Anna Kotkansalo (Turku), Raul Laasik (Tampere), Heikki Mäntymäki (Tampere), Kari Salo (Helsinki), Tuomo Tessleff (Tampere), who have in addition to the authors been developing the register.
Funding
Open Access funding provided by University of Helsinki including Helsinki University Central Hospital.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors have no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Marjamaa, J., Huttunen, J., Kankare, J. et al. The Finnish spine register (FinSpine): development, design, validation and utility. Eur Spine J 32, 3731–3743 (2023). https://doi.org/10.1007/s00586-023-07874-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-023-07874-3