
Abstract
While referring to the evidence adopted in the Tokyo Guidelines 2007 (TG07) as well as subsequently obtained evidence, further discussion took place on terminology, etiology, and epidemiological data. In particular, new findings have accumulated on the occurrence of symptoms in patients with gallstones, frequency of severe cholecystitis and cholangitis, onset of cholecystitis and cholangitis after endoscopic retrograde cholangiopancreatography and medications, mortality rate, and recurrence rate. The primary etiology of acute cholangitis/cholecystitis is the presence of stones. Next to stones, the most significant etiology of acute cholangitis is benign/malignant stenosis of the biliary tract. On the other hand, there is another type of acute cholecystitis, acute acalculous cholecystitis, in which stones are not involved as causative factors. Risk factors for acute acalculous cholecystitis include surgery, trauma, burn, and parenteral nutrition. After 2000, the mortality rate of acute cholangitis has been about 10 %, while that of acute cholecystitis has generally been less than 1 %. After the publication of TG07, diagnostic criteria and severity assessment criteria were standardized, and the distribution of cases according to severity and comparison of clinical data among target populations have become more subjective. The concept of healthcare-associated infections is important in the current treatment of infection. The treatment of acute cholangitis and cholecystitis substantially differs from that of community-acquired infections. Cholangitis and cholecystitis as healthcare-associated infections are clearly described in the updated Tokyo Guidelines (TG13).
Free full-text articles and a mobile application of TG13 are available via http://www.jshbps.jp/en/guideline/tg13.html.
Similar content being viewed by others



Introduction
Acute biliary infection comprises manifold disease concepts and is mostly separated into [1] acute cholangitis, a systemic infectious disease that is occasionally life-threatening and requires immediate treatment, and [2] acute cholecystitis, frequently presenting a mild clinical course.
The definition, pathophysiology, and epidemiology of acute cholangitis are presented in the Tokyo Guidelines for the management of acute cholangitis and chlecystitis 2007 (TG07) [1], while the updated Tokyo Guidelines (TG13) present more subjective data acquired throughout the revision of TG07. As for the data of current clinical trials in particular, the data concerning frequency of severe cases, mortality rate, and recurrence rate are introduced along with epidemiological data.
Terminology
Acute cholangitis
Definition
Acute cholangitis is a morbid condition with acute inflammation and infection in the bile duct [1, 2].
Pathophysiology
The onset of acute cholangitis involves two factors: (1) increased bacteria in the bile duct, and (2) elevated intraductal pressure in the bile duct allowing translocation of bacteria or endotoxin into the vascular and lymphatic system (cholangio-venous/lymphatic reflux). Because of its anatomical characteristics, the biliary system is likely to be affected by the elevated intraductal pressure. In acute cholangitis, bile ductules tend to become more permeable to the translocation of bacteria and toxins with the elevated intraductal biliary pressure. This process results in serious and fatal infections such as hepatic abscess and sepsis [1].
Historical aspect of terminology
Signs of hepatic fever
Hepatic fever was a term used for the first time by Charcot in his report published in 1887 [3]. Intermittent fever accompanied by chills, right upper quadrant abdominal pain, and jaundice have been established as Charcot’s triad.
Acute obstructive cholangitis
Acute obstructive cholangitis was defined by Reynolds and Dargan [4] in 1959 as a syndrome consisting of lethargy or mental confusion and shock, as well as fever, jaundice, and abdominal pain caused by biliary obstruction. They indicated that emergency surgical biliary decompression was the only effective procedure for treating the disease. These five symptoms were thus called Reynold’s pentad.
Longmire’s classification
Longmire classified patients with three characteristics of intermittent fever accompanied by chills and shivering, right upper quadrant abdominal pain, and jaundice as acute suppurative cholangitis, and those with lethargy or mental confusion and shock along with the triad as acute obstructive suppurative cholangitis (AOSC). He also reported that the latter corresponded to the morbidity of acute obstructive cholangitis as defined by Reynolds [5].
However, terms such as acute obstructive cholangitis and acute obstructive suppurative cholangitis (AOSC) are not appropriate as current clinical terminology because their definition is conceptual and ambiguous.
Acute cholangitis/cholecystitis as healthcare-associated infections
In the US IDSA/SIS guidelines on abdominal infection, acute cholangitis/cholecystitis refers to biliary tract infection that has developed in any of the following patients: patients with a history of less than 12 months hospital stay, patients undergoing dialysis, patients staying at nursing home/rehabilitation facility, and patients in an immune-compromised state [6].
That concept has been extrapolated, and acute cholangitis/cholecystitis as a healthcare-associated infection in Japan refers to infection that has developed in patients (long-term recumbency, admission to nursing home, gastrostomy, tracheostomy, repeated aspiration pneumonia, bed sore, uretheral catheter placement, history of recent postoperative infection, or undergoing antimicrobial therapy due to other diseases) at risk of having resistant bacteria (bacteria with a high minimum inhibitory concentration, MIC). Those infections should be treated independently from community-required infections.
Acute cholecystitis
Definition
Acute inflammatory disease of the gallbladder, often attributable to gallstones, but many factors, such as ischemia, motility disorders, direct chemical injury, infections by microorganism, protozoon and parasites, collagen disease, and allergic reaction are also involved [1].
Pathophysiology
In the majority of patients, gallstones are the cause of acute cholecystitis. The process is one of physical obstruction of the gallbladder at the neck or in the cystic duct by a gallstone. This obstruction results in increased pressure in the gallbladder. There are two factors which determine the progression to acute cholecystitis—the degree of obstruction and the duration of the obstruction. If the obstruction is partial and of short duration, the patient experiences biliary colic. If the obstruction is complete and of long duration, the patient develops acute cholecystitis. If the patient does not receive early treatment, the disease becomes more serious and complications can occur [1].
Pathological classification
-
(1)
Edematous cholecystitis: 1st stage (2–4 days) The gallbladder has interstitial fluid with dilated capillaries and lymphatics. The gallbladder wall is edematous. Gallbladder tissue is intact histologically with edema in the subserosal layer [1].
-
(2)
Necrotizing cholecystitis: 2nd stage (3–5 days) The gallbladder has edematous changes with areas of hemorrhage and necrosis. When the gallbladder wall is subject to elevated internal pressure, the blood flow is obstructed with histological evidence of vascular thrombosis and occlusion. There are areas of scattered necrosis but they are superficial and do not involve the full thickness of the gallbladder wall [1] (Fig. 1).
Fig. 1 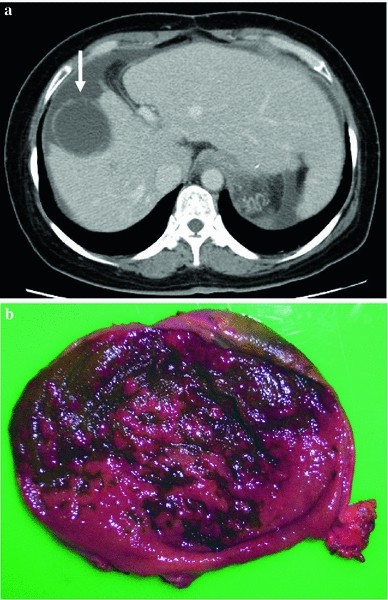
Necrotizing cholecystitis. a Contrast-enhanced CT images show discontinuity of the gallbladder wall, suggesting possible presence of necrosis in a portion of the wall. b Resected specimen showing extensive falling-off of the gallbladder membrane, erosion, ulcer, and exposed fascia. Histologically, necrosis of the gallbladder wall and suppurative inflammation accompanying abscess (data not shown) were observed with fibrillation and regenerating hyperplastic epithelium as background
-
(3)
Suppurative cholecystitis: 3rd stage (7–10 days) The gallbladder wall has white blood cells that present areas of necrosis and suppuration. In this stage, the active repairing process of inflammation is evident. The enlarged gallbladder begins to contract and the wall is thickened due to fibrous proliferation. Intramural abscesses are observed and do not involve the entire thickness of the wall. Pericholecystic abscesses are also present [1] (Fig. 2).
Fig. 2 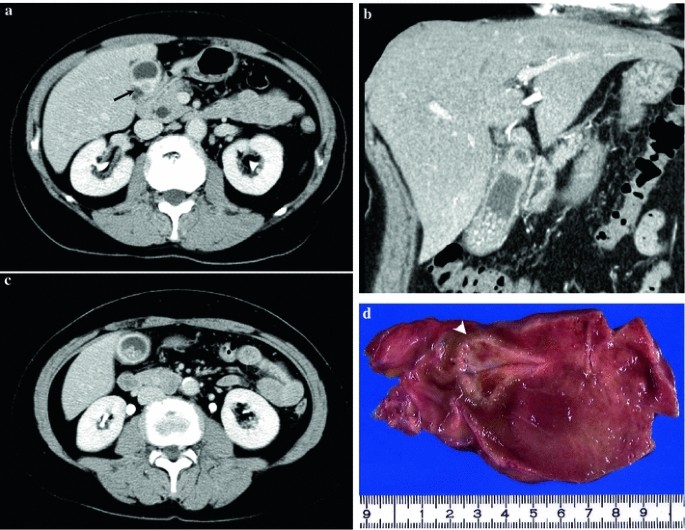
Suppurative cholecystitis. a Contrast-enhanced CT visualizing the gallbladder wall under extrinsic compression (up arrow) suggests possible presence of abscess in a portion of the gallbladder wall. b–c Many minute stones were observed within the gallbladder. d The resected specimen shows the gallbladder membrane accompanying extensive abscess formation within the wall (arrowhead)
-
(4)
Chronic cholecystitis: Chronic cholecystitis occurs after the repeated occurrence of mild cholecystitis attacks, and is characterized by mucosal atrophy and fibrosis of the gallbladder wall. It can also be caused by the chronic irritation of large gallstones and may often induce acute cholecystitis [1]. Acute on chronic cholecystitis refers to acute infection that has occurred in chronic cholecystitis [7, 8] (Fig. 3). Histologically, neutrophil invasion is observed in the gallbladder wall with chronic cholecystitis accompanying lymphocyte/plasma cell infiltration and fibrosis.
Fig. 3 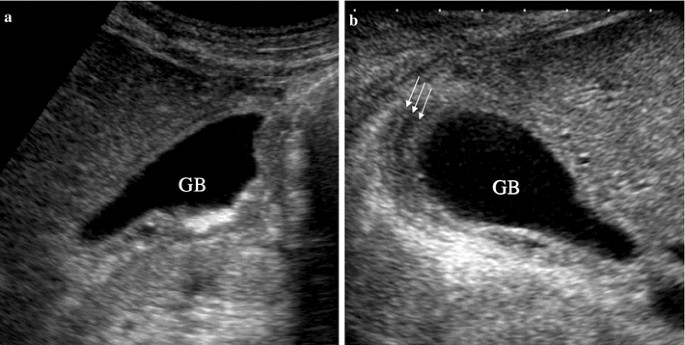
US images of acute-on-chronic cholecystitis patients. a The gallbladder wall is shown to have thickened prior to the onset of acute inflammation. b The gallbladder itself continued to swell after the onset of acute inflammation and the wall has further thickened along with striated intraluminal lucency (up arrow). Only by comparing the images before (a) and after (b) the onset of acute inflammation can a decision of the wall thickening and the swelling of gallbladder be correctly made



Special forms of acute cholecystitis
-
(1)
Acalculous cholecystitis: Acute cholecystitis without cholecystolithiasis
-
(2)
Xanthogranulomatous cholecystitis: Cholecystitis characterized by xanthogranulomatous thickening of the gallbladder wall [9] and elevated intra-gallbladder pressure due to stones with a rupture of the Rokitansky–Achoff sinuses. This causes leakage and entry of bile into the gallbladder wall. It is ingested by histocytes to form granulomas consisting of foamy histocytes. Patients usually have symptoms of acute cholecystitis in the initial stage.
-
(3)
Emphysematous cholecystitis: In emphysematous cholecystitis, air appears in the gallbladder wall due to infection by gas-forming anerobes including Clostridium perfringens. It is often seen in diabetic patients, and is likely to progress to sepsis and gangrenous cholecystitis [1].
-
(4)
Torsion of the gallbladder: Cause of acute cholecystitis [10]. Torsion of the gallbladder is known to occur by inherited, acquired, and other physical causes. The inherited factor is the floating gallbladder, which is very mobile because the gallbladder and cystic ducts are connected with the liver by a fused ligament. The acquired factors include splanchnoptosis, senile humpback, scoliosis, and weight loss. Physical factors causing torsion of the gallbladder include sudden change of intraperitoneal pressure, sudden change of body position, pendulum-like movement in the anteflexion position, hyperperistalsis of the organs near the gallbladder, defecation, and blow to the abdomen.
Advanced forms of and the type of complications of acute cholecystitis [1]
-
(1)
Perforation of gallbladder: Perforation of the gallbladder is caused by acute cholecystitis, injury, or tumors, and occurs most frequently as a result of ischemia and necrosis of the gallbladder wall.
-
(2)
Biliary peritonitis: Biliary peritonitis occurs with the entry into the peritoneal cavity of bile leakage due to various causes including cholecystitis-induced gallbladder perforation, trauma, and a detached catheter during biliary drainage and incomplete suture after biliary operation.
-
(3)
Pericholecystic abscess: A morbid condition in which perforation of the gallbladder wall is covered by the surrounding tissues along with the formation of abscesses around the gallbladder
-
(4)
Biliary fistula: A biliary fistula can occur between the gallbladder and the duodenum following an episode of acute cholecystitis. This is usually caused by a large gallbladder stone eroding through the wall of the gallbladder into the duodenum. If the stone is large in size, the patient can develop gallstone ileus with the stone causing mechanical small bowel obstruction at the ileocecal valve.
Frequency of symptom appearance
Incidence
Q1. What is the incidence proportion of the appearance of symptoms in patients with asymptomatic gallstones or those with mild gallstones?

Incidence in patients with gallstones
Acute cholecystitis is the most frequent complication occurring in patients with cholelithiasis. According to the Comprehensive Survey of Living Conditions of the People on Health and Welfare (conducted by the Medical Statistics Bureau of the Ministry of Health and Welfare), the number of cases with acute cholecystitis has increased from 3.9 million in 1979 to over 10 million in 1993 (Public Welfare Index in Japan, 1993). No large epidemiological study has been conducted to date, but it can be estimated that approximately 10 % of the general population have gallstones [11].
Natural history of patients with asymptomatic gallstones
According to a review by Friedman, 1–2 % of patients with asymptomatic gallstones and 1–3 % of patients with mild symptoms annually presented severe symptoms or complications (acute cholecystitis, acute cholangitis, severe jaundice, or pancreatitis (Table 1)). The risk of such complications was high during the first few years after gallstones had been detected and it decreased subsequently. The probability of undergoing operation due to subsequent severe symptoms was 6–8 %/year in patients initially presenting moderate symptoms and the symptoms decreased year by year [12]. Observational studies involving patients with mild cholecystolithiasis have found that, during 5–7 years’ observation, 15 % of the subjects presenting mild or nonspecific symptoms developed complications associated with gallstones, 12 % developed acute cholecystitis (n = 153), 21.9 % of the subjects were without symptoms during 8.7 years’ observation (median), and 42 % of those with mild symptoms developed abdominal pain of higher than mild severity (n = 856), respectively. The above data show that 20–40 % of patients with asymptomatic cholelithiasis have a risk for developing some type of symptoms/signs (1–3 % annually) [12–18].
Incidence of severe cases of acute cholecystitis and cholangitis
Q2. What is the incidence proportion of severe cases of acute cholangitis?

Severe cases (grade III) in TG07 refer to those having poor prognostic factors including shock, consciousness disturbance, organ failure, and disseminated intravascular coagulation. The definition was ambiguous before the publication of TG07, which, after review of the frequency of acute cholangitis, reported that the incidence of severe cases was 7–25.5 % for shock, 7–22.2 % for consciousness disturbance, and 3.5–7.7 % for Reynold’s pentad [19].
The proportion of cases diagnosed as severe (grade III) according to the TG07 severity assessment criteria was 12.3 % or 23 of the 187 cases of acute cholangitis due to bile duct stones [20].
Q3. What is the proportion of severe cases of acute cholecystitis?

“Severe” in TG07 refers to acute cholecystitis accompanying organ dysfunction (grade III), and the proportion of the above cases was 6.0 % (14 of 235 cases) [21].
Acute cholangitis and cholecystitis as complications following ERCP
Q4. What is the proportion of acute cholangitis and cholecystitis following ERCP?

The incidence of complications following endoscopic retrograde cholangiopancreatography (ERCP) is 0.8–12.1 % and the mortality rate is 0.0023–1.5 % [22–37]. The most frequently encountered complication is acute pancreatitis, although mild to moderate cases account for the greater part (Supplementary Table 1).
The proportion of acute cholangitis and cholecystitis after ERCP is 0.5–2.4 % for cholangitis and 0.2–1.0 % for cholecystitis [22–26, 29–33].
There are differences in the proportion of complications between diagnostic ERCP and therapeutic ERCP, and those of cholangitis and overall complications associated with therapeutic ERCP are more likely to become elevated [31, 33, 42].
Due to the diffusion of procedures and improved techniques of operators, complications following ERCP have increased in recent years, although no change has been observed in the frequency of the occurrence of acute cholecystitis, so its occurrence is unpredictable [31].
Etiology
Acute cholangitis
Q5. What are the etiology and mechanism of acute cholangitis?

The onset of acute cholangitis requires two factors, [1] biliary obstruction and [2] bacterial growth in bile (bile infection). Causes of frequent biliary obstruction are choledocholithiasis, benign biliary stenosis, stricture of the biliary anastomosis, and stenosis by malignant diseases [38, 39]. Choledocholithiasis used to be the most frequent cause, but recently the incidence of acute cholangitis caused by malignant disease, sclerosing cholangitis, and non-surgical instrumentation of the biliary tract has been increasing. It is reported that malignant disease accounts for about 10–30 % of cases with acute cholangitis [38, 39]. Tables 2 and 3 show the results of studies on the causes of acute cholangitis.
Acute cholecystitis
Q6. What are the etiology and mechanism of acute cholecystitis?

Gallstones account for 90–95 % of the causes of acute cholecystitis [46–49]. Following cystic duct obstruction and cholestasis within the gallbladder due to the torsion of stones, gallbladder mucosa disorder occurs, thereby inducing the activation of infectious mediator [50]. On the other hand, acute acalculous cholecystitis accounts for 3.7–14 % of acute cholecystitis [51–55]. Risk factors include surgery, trauma, long-term intensive care unit stay, infection, thermal burn, and parenteral nutrition [56, 57].
Risk factors
Q7. What are the factors for which association with the development of acute cholangitis/cholecystitis is suggested?

“4Fs” and “5Fs”
Acute cholecystitis and four (or five) “Fs”
The “4Fs” (forties, female, fat, fair) and “5Fs” (4Fs plus fecund or fertile) have been shown to be associated with lithogenesis in the gallbladder [50]. However, it has not been established whether or not all these factors are associated with the development of acute cholangitis/cholecystitis.
Age and female gender
There is no evidence to suggest the association of age/sex with the onset of acute cholangitis/cholecystitis.
According to the Framingham study which examined risk factors of cholelithiasis in subjects 30–59 years of age followed for 10 years, the risk for the development of cholelithiasis was largest in those subjects in the age range 55–62 years, and the incidence of onset in females was more than twice as large as in males in any age range, and increased with age [58].
Obesity
Patients with cholelithiasis are more likely to be obese than those without [58], and cholelithiasis is a major comorbidity of obesity. The proportion of cholelithiasis and cholecystitis in the obese aged 37–60 years (female BMI > 34 [(weight kg)/(height m)2], and male BMI > 38) was significantly higher than that in the non-obese (cholelithiasis: 5.8 vs. 1.5 %, odds ratio [OR] = 4.9; cholecystitis: 0.8 vs. 3.4 %, OR = 5.2) [59].
Role of pregnancy, fecundity, and fertility
No evidence exists to suggest an association between pregnancy/fecundity and the onset of acute cholangitis/cholecystitis.
The risk for cholecystectomy due to gallbladder diseases in middle-aged females (50–64 years of age) increased with the frequency of delivery and decreased in proportion to the duration of lactation [60]. Cholelithiasis accounted for more than 90 % of the causes of cholelithiasis in pregnancy and cholelithiasis was the most frequently encountered surgical disease next to appendicitis [61]. Gallstones were detected by routine ultrasound imaging in 3.5 % of pregnant women, although it is not known whether or not pregnancy is associated with an increased risk of cholangitis [61].
Drugs as etiological agents
According to a review by Michielsen et al., drugs promoting the generation of gallbladder stones were indirectly associated with a risk of acute cholecystitis [62]. A developmental mechanism of drug-associated gallbladder diseases in that review is presented in Table 4.
Statins, which are drugs for hyperlipidemia, may decrease the risk for cholecystectomy due to gallbladder stones [63–66]. There are also reports suggesting that thiazide was involved in the increased risk for cholecystectomy due to acute cholecystitis/gallbladder diseases [67–69], although there is a report that failed to detect an association [70]. Transcatheter hepatic arterial chemotherapy has been indicated to potentially induce chemical cholecystitis due to direct toxicity [62, 71]. The relative risk for the onset of cholecystitis or cholecystectomy due to hormone replacement therapy was two-fold larger [72, 73].
AIDS as a risk factor
Typical gallbladder diseases in AIDS patients are AIDS cholangiopathy and acute acalculous cholecystitis [74]. The former showed higher frequency similar to sclerosing cholangititis while the latter showed relatively low frequency. Abdominal operations in AIDS patients have found that the most frequently encountered causative disease was acute cholecystitis [75].
AIDS cholangiopathy is frequently observed in middle-aged patients (mean age 37 years; 21–59) with a mean 15 ± 2.2 month history of AIDS, and 90 % of chief complaints occur in the right upper quadrant abdomen. Biochemical examination demonstrates a marked elevation in the level of alkaline phosphatase [74]. Abdominal ultrasound, computed tomography (CT) [74], magnetic resonance imaging/magnetic resonance cholangiopancreatography (MRI/MRCP) [76], CT [74], and MRI/MRCP [76] shows imaging (occasionally, beading) of stenosis/dilatation in the intra-/extrahepatic bile duct.
Acute acalculous cholecystitis in AIDS patients was characterized by young age, availability of oral intake, pain in the right upper quadrant abdomen, marked elevation in the level of alkaline phosphatase and a slight increase in the serum bilirubin level, and accompanying cytomegalovirus infection or cryptosporidium infection [74].
Other etiologies of acute cholangitis
There are two other etiologies of acute cholangitis: Mirizzi syndrome and Lemmel syndrome. Mirizzi syndrome is a morbid condition with stenosis of the common bile duct caused by mechanical pressure and/or inflammatory changes caused by the stones present in the gallbladder neck and cystic ducts [77]. Two types have been described: type I, which is a morbid condition with the bile duct compressed from the left by the stones present in the gallbladder neck and cystic ducts and pericholecystic inflammatory changes (Fig. 4a–c, Supplementary Fig. 1a–c); and type II, which is a morbid condition with biliobilary fistulation caused by pressure necrosis of the bile duct due to cholecystolithiasis [77]. Lemmel syndrome (Fig. 5a, b; Supplementary Fig. 2a, b) is a series of morbid conditions in which the duodenal parapapillary diverticulum compresses or displaces the opening of the bile duct or pancreatic duct and obstructs the passage of bile in the bile duct or hepatic duct, thereby causing cholestasis, jaundice, gallstone, cholangitis, and pancreatitis [78].

Mirizzi syndrome. a MRCP showed the obstructed common hepatic duct but failed to visualize the gallbladder. b Cholangiography with an ENBD tube showed the stenosed common hepatic duct but failed to visualize the gallbladder. c Coronal images by contrast-enhanced CT clearly showing that stones impacted in the gallbladder duct have expanded the common hepatic duct, thereby inducing stenosis

Lemmel syndrome. a Upper gastrointestinal endoscopy showing a diverticulum just above the papilla of Vater (right arrow). b ERCP demonstrating findings of extrinsic compression in the lower biliary tract (right arrow)
Prognosis
Mortality
Q8. What is the mortality rate of acute cholangitis/cholecystitis?

Acute cholangitis (Table 5)
It has been reported that the mortality rate of acute cholangitis was higher than 50 % before 1980, 10–30 % in 1981–1990s, and 2.7–10 % after 2000 [42, 45, 79–97]. Such differences in mortality rate are assumed to have arisen from differences in severity and diagnostic criteria for the accumulated cases.
Acute cholecystitis (Table 6)
The mortality rate in patients with acute cholecystitis has been reported to be 0–10 % [17, 21, 98–115]. According to reports after 2000, the mortality rate was less than 1 % [17, 105–115], and no marked difference according to eras and communities is present.
The mortality rate according to severity in TG07 was classified as mild (grade I) (1/161, 0.6 %), moderate (grade II) (0/60, 0 %), or severe (grade III) (3/14, 21.4 %). Overall, acute cholecystitis accounts for 1.7 % [21].
Recurrence
Recurrence rate of acute cholecystitis
Q9. What is the recurrence rate for cases having undergone conservative treatment for acute cholecystitis?

Fundamentally, no recurrence has occurred for cases undergoing cholecystectomy for acute cholecystitis.
(1) Recurrence of acute cholecystitis for which remission was achieved with conservative treatment
According to randomized controlled trials comparing outcomes of cholecystectomy and follow-up after remission of acute cholecystitis, 36 % of the cases in the follow-up group subsequently required emergency hospitalization due to pain and gallstone-associated complications (acute cholecystitis, bile duct stones, acute pancreatitis) [116, 117] and 24–30 % required cholecystectomy [116–118].
On the other hand, the recurrence rate of acute cholecystitis cases waiting for cholecystectomy was 2.5–22 % [104, 116, 117, 119], and 19 % required emergency hospitalization [116, 117]. It has been reported that, of these recurrence cases, the recurrence of acute cholecystitis accounted for 2.5 % [104], 22 % [119], and gallbladder perforation 6 %, respectively [119].
(2) Recurrence of acute cholecystitis for which no cholecystectomy was carried out for some reason
Recurrence occurred in 22–47 % of acute cholecystitis cases undergoing follow-up without cholecystectomy subsequent to percutaneous gallbladder drainage [120–122].
Recurrence rate after treatment for gallbladder stones
Q10. What is the recurrence rate after endoscopic treatment for cholelithiasis?

Recurrence of complications in the biliary system
Following endoscopic sphincterectomy (EST), recurrence occurred in 7–47 % of cases with complications in the biliary tract system (cholelithiasis, biliary tract colic, cholangitis) within the 2.5–15-year follow-up period [123–129].
Recurrence of acute cholecystitis
It has been reported that the proportion of symptom appearance of acute cholecystitis (including cases in which symptoms have appeared) was 5.6–22 % [123, 125, 126, 128–130] when calculous gallbladder was left untreated after EST [123–126, 128–133] and 0–7 % for cases with acalculous gallbladder or after cholecystectomy [123–126, 130, 133] (Supplementary Table 2).
A risk factor for recurrence after endoscopic treatment for bile duct stones by means of endoscopic papillary balloon dilation (EPBD) is the occurrence of calculous gallbladder [134, 135]. Compared with treatment by means of EST, the incidence of acute cholecystitis a long time after treatment with EPBD is lower [136], although the recurrence rates of bile duct stones are the same (5.5 and 8.8 %) for both treatment methods [137].
References
Kimura Y, Takada T, Kawarada Y, Nimura Y, Hirata K, Sekimoto M, et al. Definitions, pathophysiology, and epidemiology of acute cholangitis and cholecystitis: Tokyo Guidelines. J Hepatobiliary Pancreat Surg. 2007;14(1):15–26 (clinical practice guidelines CPGs).
Ahrendt S, Pitt H. The biliary tract. In: Sabiston textbook of surgery. 17th edn. Philadelphia: W. B. Saunders; 2004. p. 1625.
Charcot M. De la fievre hepatique symptomatique—comparaison avec la fievre uroseptique. Lecons sur les maladies du foie des voies biliares et des reins). Paris: Bourneville et Sevestre; 1877. p. 176–185.
Reynolds BM, Dargan EL. Acute obstructive cholangitis—a distinct syndrome. Ann Surg. 1959;150:299–303.
Longmire WP. Suppurative cholangitis. In: Hardy JD, editor. Critical surgical illness. New York: Saunders; 1971. p. 397–424.
Solomkin JS, Mazuski JE, Bradley JS, Rodvold KA, Goldstein EJ, Baron EJ, et al. Diagnosis and management of complicated intra-abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Disease Society of America. Clin Infect Dis. 2010;50:133–64 (clinical practice guidelines CPGs).
Fitzgibbons RJ Jr, Tseng A, Wang H, Ryberg A, Nguyen N, Sims KL. Acute cholecystitis. Does the clinical diagnosis correlate with the pathological diagnosis? Surg Endosc. 1996;10:1180–4.
Yacoub WN, Petrosyan M, Sehgal I, Ma Y, Chandrasoma P, Mason RJ. Prediction of patients with acute cholecystitis requiring emergent cholecystectomy: a simple score. Gastroenterol Res Pract. 2010. doi:901739
Goodman ZD, Ishak KG. Xanthogranulomatos cholecystitis. Am J Surg Pathol. 1981;5:653–9.
Gross RE. Congenital anomalies of the gallbladder. Arch Surg. 1936;32:131–62.
Tazuma S. Gallstone disease: epidemiology, pathogenesis, and classification of biliary stones (common bile duct and intrahepatic). Best Pract Res Clin Gastroenterol. 2006;20:1075–83.
Friedman GD. Natural history of asymptomatic and symptomatic gallstones. Am J Surg. 1993;165:399–404.
Persson GE. Expectant management of patients with gallbladder stones diagnosed at planned investigation. A prospective 5- to 7-year follow-up study of 153 patients. Scand J Gastroenterol. 1996;31:191–9.
Festi D, Reggiani ML, Attili AF, Loria P, Pazzi P, Scaioli E, Capodicasa S, Romano F, Roda E, Colecchia A. Natural history of gallstone disease: expectant management or active treatment? Results from a population-based cohort study. J Gastroenterol Hepatol. 2010;25:719–24.
Ransohoff DF, Gracie WA, Wolfenson LB, et al. Prophylactic cholecystectomy or expectant management for silent gallstones. A decision analysis to assess survival. Ann Intern Med. 1983;99:199–204.
Stinton LM, Myers RP, Shaffer EA. Epidemiology of gallstones. Gastroenterol Clin North Am. 2010;39:157–9.
Portincasa P, Moschetta A, Palasciano G. Cholesterol gallstone disease. Lancet. 2006;15(368):230–9.
Portincasa P, Moschetta A, Petruzzelli M, Palasciano G, Di Ciaula A, Pezzolla A. Gallstone disease: symptoms and diagnosis of gallbladder stones. Best Pract Res Clin Gastroenterol. 2006;20:1017–29.
Wada K, Takada T, Kawarada Y, Nimura Y, Miura F, Yoshida M, et al. Diagnostic criteria and severity assessment of acute cholangitis: Tokyo Guidelines. J Hepatobiliary Pancreat Surg. 2007;14:52–8 (clinical practice guidelines CPGs).
Kiriyama S, Kumada T, Tanikawa M, Hisanaga Y, Toyota H, Kanamori A, et al. Verification of the current JPN guidelines for the management of acute cholangitis and cholecystitis: diagnostic criteria and severity assesment. J Abdom Emerg Med. 2011;31:475–82 (in Japanese).
Lee SW, Yang SS, Chang CS, Yeh HJ. Impact of the Tokyo guidelines on the management of patients with acute calculous cholecystitis. J Gastroenterol Hepatol. 2009;24:1857–61.
Andriulli A, Loperfido S, Napolitano G, Niro G, Valvano MR, Spirito F, et al. Incidence rates of post-ERCP complications: a systematic survey of prospective studies. Am J Gastroenterol. 2007;102:1781–817.
Vitte RL, Morfoisse JJ. Evaluation of endoscopic retrograde cholangiopancreatography procedures performed in general hospitals in France. Gastroenterol Clin Biol. 2007;31:740–9.
Williams EJ, Taylor S, Fairclough P, Hamlyn A, Logan RF, Martin D, et al. Are we meeting the standards set for endoscopy? Results of a large-scale prospective survey of endoscopic retrograde cholangio-pancreatograph practice. Gut. 2007;56:821–9.
Chong VH, Yim HB, Lim CC. Endoscopic retrograde cholangiopancreatography in the elderly: outcomes, safety and complications. Singapore Med J. 2005;46:621–6.
Ong TZ, Khor JL, Selamat DS, Yeoh KG, Ho KY. Complications of endoscopic retrograde cholangiography in the post-MRCP era: a tertiary center experience. World J Gastroenterol. 2005;11:5209–12.
Thompson AM, Wright DJ, Murray W, Ritchie GL, Burton HD, Stonebridge PA. Analysis of 153 deaths after upper gastrointestinal endoscopy: room for improvement? Surg Endosc. 2004;18:22–5.
Kaneko E. Complications of digestive endoscopy. Nihon Shokakibyo Gakkai Zasshi. 2004;101:571–7 (in Japanese).
Vandervoort J, Soetikno RM, Tham TC, Wong RC, Ferrari AP Jr, Montes H, et al. Risk factors for complications after performance of ERCP. Gastrointest Endosc. 2002;56:652–6.
Freeman ML, Nelson DB, Sherman S, Haber GB, Herman ME, Dorsher PJ, et al. Complications of endoscopic biliary sphincterotomy. N Engl J Med. 1996;335:909–18.
Lenriot JP, Le Neel JC, Hay JM, Jaeck D, Millat B, Fagniez PL. Retrograde cholangiopancreatography and endoscopic sphincterotomy for biliary lithiasis. Prospective evaluation in surgical circle. Gastroenterol Clin Biol. 1993;17:244–50.
Benchimol D, Bernard JL, Mouroux J, Dumas R, Elkaim D, Chazal M, et al. Infectious complications of endoscopic retrograholangio-pancreatography managed in a surgical unit. Int Surg. 1992;77:270–3.
Cotton PB, Lehman G, Vennes JA, Geenen JE, Russell RCG, Meyers WC, et al. Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointest Endosc. 1991;37:255–8.
Reiertsen O, Skjoto J, Jacobsen CD, Rosseland AR. Complications of fiberoptic gastrointestinal endoscopy; five years’ experience in a central hospital. Endoscopy. 1987;19:1–6.
Roszler MH, Campbell WL. Post-ERCP pancreatitis: association with urographic visualization during ERCP. Radiology. 1985;157:595–8.
Escourrou J, Cordova JA, Lazorthes F, Frexinos J, Ribet A. Early and late complications after endoscopic sphincterotomy for biliary lithiasis with and without the gall bladder ‘in situ’. Gut. 1984;25:598–602.
Bilbao MK, Dotter CT, Lee TG, Katon RM. Complications of endoscopic retrograde cholangiopancreatography (ERCP). A study of 10,000 cases. Gastroenterology. 1976;70:314–20.
Lipsett PA, Pitt HA. Acute cholangitis. Surg Clin North Am. 1990;70:1297–312.
Gigot JF, Leese T, Dereme T, Coutinho J, Castaing D, Bismuth H. Acute cholangitis: multivariate analysis of risk factors. Ann Surg. 1989;209:435–8.
Saharia PC, Cameron JL. Clinical management of acute cholangitis. Surg Gynecol Obstet. 1976;142:369–72.
Pitt HA, Couse NF. Biliary sepsis and toxic cholangitis. In: Moody FG, Carey LC, editors. Surgical treatment of digestive diseases. 2nd ed. Chicago: Year Book Medical Publishers; 1990. p. 332.
Thompson JE Jr, Pitt HA, Doty JE, Coleman J, Irving C. Broad spectrum penicillin as an adequate therapy for acute cholangitis. Surg Gynecol Obstet. 1990;171:275–82.
Basoli A, Schietroma M, De Santis A, Colella A, Fiocca F, Speranza V. Acute cholangitis: diagnostic and therapeutic problems. Ital J Surg Sci. 1986;16:261–7.
Daida A, Miki M, Yoshioka M, Moriyama Y. Collective study results on the bacteriological examination during biliary surgery. Jpn J Gastroenterol Surg. 1980;13:445–9 (in Japanese).
Salek J, Livote E, Sideridis K, Bank S. Analysis of risk factors predictive of early mortality and urgent ERCP in acute cholangitis. J Clin Gastroenterol. 2009;43:171–5.
Gouma DJ, Obertop H. Acute calculous cholecystitis. What is new in diagnosis and therapy? HPB Surg. 1992;6:69–78.
Mack E. Role of surgery in the management of gallstones. Semin Liver Dis. 1990;10:222–31.
Hermann RE. Surgery for acute and chronic cholecystitis. Surg Clin North Am. 1990;70:1263–75.
Sharp KW. Acute cholecystitis. Surg Clin North Am. 1988;68:269–79.
Jpn. Societ. Gastroenterol. Practice guidelines of the gallstone disease. Tokyo: Dai Nippon Printing Co., Ltd., 2009. p. 30–1 (in Japanese, clinical practice guidelines CPGs).
Williamson RC. Acalculous disease of the gall bladder. Gut. 1988;29:860–72.
Barie PS, Fischer E. Acute acalculous cholecystitis. J Am Coll Surg. 1995;180:232–44.
Ryu JK, Ryu KH, Kim KH. Clinical features of acute acalculous cholecystitis. J Clin Gastroenterol. 2003;36:166–9.
Wang AJ, Wang TE, Lin CC, Lin SC, Shih SC. Clinical predictors of severe gallbladder complications in acute acalculous cholecystitis. World J Gastroenterol. 2003;9:2821–3.
Matsusaki S, Maguchi H, Takahashi K, Katanuma A, Osanai M, Urata T, et al. Clinical features of acute acalculous cholecystitis––nosocomial manner and community-acquired manner. Nihon Shokakibyo Gakkai Zasshi. 2008;105:1749–57 (in Japanese).
Laurila J, Syrjala H, Laurila PA, Saarnio J, Ala-Kokko TI. Acute acalculous cholecystitis in critically ill patients. Acta Anaesthesiol Scand. 2004;48:986–91.
Theodorou P, Maurer CA, Spanholtz TA, Phan TQ, Amini P, Perbix W, et al. Acalculous cholecystitis in severely burned patients: incidence and predisposing factors. Burns. 2009;35:405–11.
Friedman GD, Kannel WB, Dawber TR. The epidemiology of gallbladder disease: observations in the Framingham Study. J Chronic Dis. 1966;19:273–92.
Torgerson JS, Lindroos AK, Naslund I, Peltonen M. Gallstones, gallbladder disease, and pancreatitis: cross-sectional and 2-year data from the Swedish Obese Subjects (SOS) and SOS reference studies. Am J Gastroenterol. 2003;98:1032–41.
Liu B, Beral V, Balk Will A. Million Women Study Collaborators. Childbearing, breastfeeding, other reproductive factors and the subsequent risk of hospitalization for gallbladder disease. Int J Epidemiol. 2009;38:312–8.
Sharp HT. The acute abdomen during pregnancy. Clin Obstet Gynecol. 2002;45:405–13.
Michielsen PP, Fierens H, Van Maercke YM. Drug-induced gallbladder disease. Incidence, aetiology and management. Drug Saf. 1992;7:32–45.
Tsai CJ, Leitzmann MF, Willett WC, Giovannucci EL. Statin use and the risk of cholecystectomy in women. Gastroenterology. 2009;136:1593–600.
Bodmer M, Brauchli YB, Krahenbuhl S, Jick SS, Meier CR. Statin use and risk of gallstone disease followed by cholecystectomy. JAMA. 2009;302:2001–7.
Merzon E, Weiss NS, Lustman AJ, Elhayani A, Dresner J, Vinker S. Statin administration and risk of cholecystectomy: a population-based case-control study. Expert Opin Drug Saf. 2010;9:539–43.
Erichsen R, Frøslef T, Lash TL, Pedersen L, Sørensen HT. Long-term statin use and the risk of gallstone disease: A population-based case-control study. Am J Epidemiol. 2011;173:162–70.
Rosenberg L, Shapiro S, Slone D, Kaufman DW, Miettinen OS, Stolley PD. Thiazides and acute cholecystitis. N Engl J Med. 1980;303:546–8.
Gonzalez-Perez A, Garcia Rodriguez LA. Gallbladder disease in the general population: association with cardiovascular morbidity and therapy. Pharmacoepidemiol Drug Saf. 2007;16:524–31.
Leitzmann MF, Tsai CJ, Stampfer MJ, Willett WC, Giovannucci E. Thiazide diuretics and the risk of gallbladder disease requiring surgery in women. Arch Intern Med. 2005;165:567–73.
Porter JB, Jick H, Dinan BJ. Acute cholecystitis and thiazides. N Engl J Med. 1981;304:954–5.
Wagnetz U, Jaskolka J, Yang P, Jhaveri KS. Acute ischemic cholecystitis after transarterial chemoembolization of hepatocellular carcinoma: incidence and clinical outcome. J Comput Assist Tomogr. 2010;34:348–53.
Nelson HD, Humphrey LL, Nygren P, Teutsch SM, Allan JD. Postmenopausal hormone replacement therapy: scientific review. JAMA. 2002;288:872–81.
Cirillo DJ, Wallace RB, Rodabough RJ, Greenland P, LaCroix AZ, Limacher MC, et al. Effect of estrogen therapy on gallbladder disease. JAMA. 2005;293:330–9.
Cello JP. AIDS-related biliary tract disease. Gastrointest Endosc Clin North Am. 1998;8:963.
LaRaja RD, Rothenberg RE, Odom JW, Mueller SC. The incidence of intra-abdominal surgery in acquired immunodeficiency syndrome: a statistical review of 904 patients. Surgery. 1989;105:175–9.
Bilgin M, Balci NC, Erdogan A, Momtahen AJ, Alkaade S, Rau WS. Hepatobiliary and pancreatic MRI and MRCP findings in patients with HIV infection. AJR Am J Roentgenol. 2008;191:228–32.
McSherry CK, Ferstenberg H, Virshup M. The Mirizzi syndrome: suggested classification and surgical therapy. Surg Gastroenterol. 1982;1:219–25.
Lemmel G. Die kliniscle Bedeutung der Duodenal Divertikel. Arch Venduungskrht. 1934;46:59–70.
Andrew DJ, Johnson SE. Acute suppurative cholangitis, a medical and surgical emergency. A review of ten years. Am J Gastroenterol. 1970;54:141–54.
Shimada H, Nakagawara G, Kobayashi M, Tsuchiya S, Kudo T, Morita S. Pathogenesis and clinical features of acute cholangitis accompanied by shock. Jpn J Surg. 1984;14:269–77 (in Japanese).
Csendes A, Diaz JC, Burdiles P, Maluenda F, Morales E. Risk factors and classification of acute suppurative cholangitis. Br J Surg. 1992;79:655–8.
Himal HS, Lindsay T. Ascending cholangitis: surgery versus endoscopic or percutaneous drainage. Surgery. 1990;108:629–33.
Chijiiwa K, Kozaki N, Naito T, Kameoka N. Treatment of choice for choledocholithiasis in patients with acute obstructive suppurative cholangitis and liver cirrhosis. Am J Surg. 1995;170:356–60.
Liu TJ. Acute biliary septic shock. HPB Surg. 1990;2:177–83.
Lai EC, Tam PC, Paterson IA, Ng MM, Fan ST, Choi TK, et al. Emergency surgery for severe acute cholangitis. The high risk patients. Ann Surg. 1990;211:55–9.
Arima N, Uchiya T, Hishikawa R, Saito M, Matsuo T, Kurisu S, et al. Clinical characteristics of impacted bile duct stone in eldery. Jpn J Geriat. 1993;30:964–8 (in Japanese).
Kunisaki C, Kobayashi S, Kido Y, Imai S, Harada H, Moriwaki Y, et al. Clinical evaluation of acute cholangitis with speciaal reference to detection of prognostic factor for acute obstructive supprative cholangitis. J Abdom Emerg Med. 1997;17:261–6 (in Japanese).
Tai DI, Shen FH, Liaw YF. Abnormal pre-drainage serum creatinine as a prognostic indicator in acute cholangitis. Hepatogastroenterology. 1992;39:47–50.
Thompson J, Bennion RS, Pitt HA. An analysis of infectious failures in acute cholangitis. HPB Surg. 1994;8:139–45.
Sharma BC, Kumar R, Agarwal N, Sarin SK. Endoscopic biliary drainage by nasobiliary drain or by stent placement in patients with acute cholangitis. Endoscopy. 2005;37:439–43.
Lee CC, Chang IJ, Lai YC, Chen SY, Chen SC. Epidemiology and prognostic determinants of patients with bacteremic cholecystitis or cholangitis. Am J Gastroenterol. 2007;102:563–9.
Rahman SH, Larvin M, McMahon MJ, Thompson D. Clinical presentation and delayed treatment of cholangitis in older people. Dig Dis Sci. 2005;50:2207–10.
Pang YY, Chun YA. Predictors for emergency biliary decompression in acute cholangitis. Eur J Gastroenterol Hepatol. 2006;18:727–31.
Agarwal N, Sharma BC, Sarin SK. Endoscopic management of acute cholangitis in elderly patients. World J Gastroenterol. 2006;12:6551–5.
Tsujino T, Sugita R, Yoshida H, Yagioka H, Kogure H, Sasaki T, et al. Risk factors for acute suppurative cholangitis caused by bile duct stones. Eur J Gastroenterol Hepatol. 2007;19:585–8.
Rosing DK, De Virgilio C, Nguyen AT, El Masry M, Kaji AH, Stabile BE. Cholangitis: analysis of admission prognostic indicators and outcomes. Am Surg. 2007;73:949–54.
Yeom DH, Oh HJ, Son YW, Kim TH. What are the risk factors for acute suppurative cholangitis caused by common bile duct stones? Gut Liver. 2010;4:363–7.
Meyer KA, Capos NJ, Mittelpunkt AI. Personal experiences with 1261 cases of acute and chronic cholecystitis and cholelithiasis. Surgery. 1967;61:661–8.
Ransohoff DF, Miller GL, Forsythe SB, Hermann RE. Outcome of acute cholecystitis in patients with diabetes mellitus. Ann Intern Med. 1987;106:829–32.
Gagic N, Frey CF, Galness R. Acute cholecystitis. Surg Gynecol Obstet. 1975;140:868–74.
Girard RM, Morin M. Open cholecystectomy: its morbidity and mortality as a reference standard. Can J Surg. 1993;36:75–80.
Addison NV, Finan PJ. Urgent and early cholecystectomy for acute gallbladder disease. Br J Surg. 1988;75:141–3.
Bedirli A, Sakrak O, Sozuer EM, Kerek M, Guler I. Factors effecting the complications in the natural history of acute cholecystitis. Hepatogastroenterology. 2001;48:1275–8.
Gharaibeh KI, Qasaimeh GR, Al-Heiss H, Ammari F, Bani-Hani K, Al-Jaberi TM, Al-Natour S. Effects of timing of surgery, type of inflammation, and sex on outcome of laparoscopic cholecystectomy for acute cholecystitis. J Laparoendosc Adv Surg Tech. 2002;12:193–8.
Russo MW, Wei JT, Thiny MT, Gangarosa LM, Brown A, Ringel Y, Shaheen NJ, Sandler RS. Digestive and liver diseases statistics, 2004. Gastroenterology. 2004;126:1448–53.
Papi C, Catarci M, D’Ambrosio L, Gili L, Koch M, Grassi GB, Capurso L. Timing of cholecystectomy for acute calculous cholecystitis: a meta-analysis. Am J Gastroenterol. 2004;99:147–55.
Giger U, Michel JM, Vonlanthen R, Becker K, Kocher T, Krahenbuhl L. Laparoscopic cholecystectomy in acute cholecystitis: indication, technique, risk and outcome. Langenbecks Arch Surg. 2005;390:373–80.
Johansson M, Thune A, Nelvin L, Stiernstam M, Westman B, Lundell L. Randomized clinical trial of open versus laparoscopic cholecystectomy in the treatment of acute cholecystitis. Br J Surg. 2005;92:44–9.
Al Salamah SM. Outcome of laparoscopic cholecystectomy in acute cholecystitis. J Coll Phys Surg Pak. 2005;15:400–3.
Gurusamy KS, Samraj K. Early versus delayed laparoscopic cholecystectomy for acute cholecystitis. Cochrane Database Syst Rev. 2006;4:CD005440.
Borzellino G, Sauerland S, Minicozzi AM, Verlato G, Di Pietrantonj C, de Manzoni G, et al. Laparoscopic cholecystectomy for severe acute cholecystitis. A meta-analysis of results. Surg Endosc. 2008;22:8–15.
Lee AY, Carter JJ, Hochberg MS, Stone AM, Cohen SL, Pachter HL. The timing of surgery for cholecystitis: a review of 202 consecutive patients at a large municipal hospital. Am J Surg. 2008;195:467–70.
Csikesz N, Ricciardi R, Tseng JF, Shah SA. Current status of surgical management of acute cholecystitis in the United States. World J Surg. 2008;32:2230–6.
Gurusamy K, Samraj K, Gluud C, Wilson E, Davidson BR. Meta-analysis of randomized controlled trials on the safety and effectiveness of early versus delayed laparoscopic cholecystectomy for acute cholecystitis. Br J Surg. 2010;97:141–50.
Sekimoto M, Okuma K, Imanaka Y, Yoshida M, Hirata K, Mayumi T, et al. The practical guideline for acute cholecystitis and acute cholangitis were published in 2005. In this study, we utilized administrative data to examine trends in patients characteristics, process of care, patient outcome, and medical resource utilization for patients with acute cholecustitis. J Abdom Emerg Med. 2010;30:413–9 (in Japanese).
Vetrhus M, Soreide O, Eide GE, Nesvik I, Sondenaa K. Quality of life and pain in patients with acute cholecystitis. Results of a randomized clinical trial. Scand J Surg. 2005;94:34–9.
Vetrhus M, Soreide O, Nesvik I, Sondenaa K. Acute cholecystitis: delayed surgery or observation. A randomized clinical trial. Scand J Gastroenterol. 2003;38:985–90.
Sondenaa K, Nesvik I, Solhaug JH, Soreide O. Randomization to surgery or observation in patients with symptomatic gallbladder stone disease. The problem of evidence-based medicine in clinical practice. Scand J Gastroenterol. 1997;32:611–6.
Lahtinen J, Alhava EM, Aukee S. Acute cholecystitis treated by early and delayed surgery. A controlled clinical trial. Scand J Gastroenterol. 1978;13:673–8.
Andren-Sandberg A, Haugsvedt T, Larssen TB, Sondenaa K. Complication and late outcome following percutaneous drainage of the gallbladder in acute calculous cholecystitis. Dig Surg. 2001;18:393–8.
Granlund A, Karlson BM, Elvin A, Rasmussen I. Ultrasound-guided percutaneous cholecystectomy in high-risk surgical patients. Langenbecks Arch Surg. 2001;386:212–7.
McLoughlin RF, Patterson EJ, Mathieson JR, Cooperberg PL, MacFarlane JK. Radiologically guided percutaneous cholecystectomy for acute cholecystitis: long-term outcome in 50 patients. Can Assoc Radiol J. 1994;45:455–9.
Ando T, Tsuyuguchi T, Saito M, Ishihara T, Yamaguchi T, Saisho H. Risk factors for recurrent bile duct stones after endoscopic papillotomy. Gut. 2003;52:116–21.
Sugiyama M, Atomi Y. Risk factors predictive of late complications after endoscopic sphincterotomy for bile duct stones: long-term (more than 10 years) follow-up study. Am J Gastroenterol. 2002;97:2763–7.
Costamagna G, Tringali A, Shah SK, Mutignani M, Zuccala G, Perri V. Long-term follow-up of patients after endoscopic sphincterotomy for choledocholithiasis, and risk factors for recurrence. Endoscopy. 2002;34:273–9.
Tanaka M, Takahata S, Konmi H, Matsunaga H, Yokohata K, Takeda T, et al. Long-term consequence of endoscopic sphincterotomy for bile duct stones. Gastrointest Endosc. 1998;48:465–9.
Prat F, Malak NA, Pelletier G, Buffet C, Fritsch J, Choury AD, et al. Biliary symptoms and complications more than 8 years after endoscopic sphincterotomy for choledocholithiasis. Gastroenterology. 1996;110:894–9.
Schreurs WH, Vles WJ, Stuifbergen WH, Oostvogel HJ. Endoscopic management of common bile duct stones leaving the gallbladder in situ. A cohort study with long-term follow- up. Dig Surg. 2004;21:60–4.
Boerma D, Rauws EA, Keulemans YC, Janssen IM, Bolwerk CJ, Timmer R, Boerma EJ, Obertop H, Huibregtse K, Gouma DJ. Wait-and-see policy or laparoscopic cholecystectomy after endoscopic sphincterotomy for bile-duct stones: a randomised trial. Lancet. 2002;360:761–5.
Lau JY, Leow CK, Fung TM, Suen BY, Yu LM, Lai PB, et al. Cholecystectomy or gallbladder in situ after endoscopic sphincterotomy and bile duct stone removal in Chinese patients. Gastroenterology. 2006;130:96–103.
Lee KM, Paik CN, Chung WC, Kim JD, Lee CR, Yang JM. Risk factors for cholecystectomy in patients with gallbladder stones after endoscopic clearance of common bile duct stones. Surg Endosc. 2009;23:1713–9.
Lee JK, Ryu JK, Park JK, Yoon WJ, Lee SH, Lee KH, et al. Risk factors of acute cholecystitis after endoscopic common bile duct stone removal. World J Gastroenterol. 2006;12:956–60.
Kwon SK, Lee BS, Kim NJ, Lee HY, Chae HB, Youn SJ, et al. Is cholecystectomy necessary after ERCP for bile duct stones in patients with gallbladder in situ? Korean J Intern Med. 2001;16:254–9.
Tsujino T, Kawabe T, Komatsu Y, Yoshida H, Isayama H, Sasaki T, et al. Endoscopic papillary balloon dilation for bile duct stone: immediate and long-term outcomes in 1000 patients. Clin Gastroenterol Hepatol. 2007;5:130–7.
Tsujino T, Kawabe T, Isayama H, Yashima Y, Yagioka H, Kogure H, et al. Management of late biliary complications in patients with gallbladder stones in situ after endoscopic papillary balloon dilation. Eur J Gastroenterol Hepatol. 2009;21:376–80.
Bergman JJ, Rauws EA, Fockens P, van Berkel AM, Bossuyt PM, Tijssen JG, et al. Randomised trial of endoscopic balloon dilation versus endoscopic sphincterotomy for removal of bileduct stones. Lancet. 1997;349:1124–9.
Liu Y, Su P, Lin S, Xiao K, Chen P, An S, et al. Endoscopic papillary balloon dilatation vs endoscopic sphincterotomy in the treatment for choledocholithiasis: a meta-analysis. J Gastroenterol Hepatol. 2012;27:464–471.
Acknowledgments
We would like to express our deep gratitude to the Japanese Society of Hepato-Biliary-Pancreatic Surgery, the Japanese Society of Abdominal Emergency Medicine, the Japanese Society of Surgical Infection, the Japan Biliary Association, and the Japan Radiological Society for their substantial support and guidance in the preparation of this article.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
534_2012_564_MOESM2_ESM.ppt
Supplementary Fig. 1. Intraoperative pictures of laparoscopic subtotal cholecystectomy in a patient with Mirizzi syndrome (Fig. 4 case). a The presence of stones was confirmed by incision of the gallbladder neck and the Hartmann pouch (Δ). b Stones impacted in the pouch (Δ) were removed using a forceps followed by closure with intracorporeal sutures. c Following intraoperative cholangiography through an endoscopic naso-biliary drainage tube, common hepatic duct stricture was confirmed to have been almost released
Supplementary Fig. 2. Lemmel syndrome. a Contrast-enhanced CT showing dilatation of intrahepatic and extrahepatic bile ducts (→). b A large duodenal diverticulum (Δ) is shown to be compressing the common bile duct (CBD) (PPT 1386 kb)
About this article
Cite this article
Kimura, Y., Takada, T., Strasberg, S.M. et al. TG13 current terminology, etiology, and epidemiology of acute cholangitis and cholecystitis. J Hepatobiliary Pancreat Sci 20, 8–23 (2013). https://doi.org/10.1007/s00534-012-0564-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00534-012-0564-0