
Abstract
Purpose
Preventing chemotherapy-induced nausea and vomiting (CINV) is integral to treatment success in patients with cancer. This analysis was undertaken to assess the relative efficacy and safety of palonosetron versus older 5HT3 RAs in preventing CINV associated with moderately or highly emetogenic chemotherapy.
Methods
Patient-level data from four randomized, double-blind, phase III trials comparing palonosetron 0.25 or 0.75 mg with ondansetron 32 mg, dolasetron 100 mg, or granisetron 40 μg/kg were analyzed. Endpoints included complete response (CR: no emesis and no rescue antiemetics) in the acute (0–24 h), delayed (>24–120 h), and overall (0–120 h) postchemotherapy periods (primary), complete control (CC: no emesis, no rescue antiemetics, and no more than mild nausea), number of emetic episodes, and nausea severity.
Results
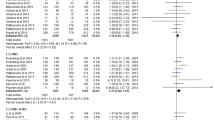
CR rates were significantly higher for palonosetron (n = 1,787) versus older 5HT3 RAs (n = 1,175) in the delayed (57 vs 45 %, P < 0.0001) and overall periods (51 vs 40 %, P < 0.0001); odds ratios (95 % CI) in the acute, delayed, and overall periods were 1.15 (0.98–1.34), 1.62 (1.40–1.88), and 1.56 (1.34–1.81), respectively. Significant differences in CC rates and nausea severity were observed for the delayed and overall periods and in emetic episodes for all three periods. The incidence of treatment-related adverse events was similar with palonosetron (0.25 mg, 20.0 %; 0.75 mg, 26.5 %) and older 5HT3 RAs (27.5 %).
Conclusions
Palonosetron is more effective than older 5HT3 RAs for controlling CINV in the delayed and overall postchemotherapy periods.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Patients with cancer who receive chemotherapy often experience nausea and vomiting (chemotherapy-induced nausea and vomiting, CINV), the onset of which can be acute (starting within minutes to hours following treatment and generally resolving within 24 h) or delayed (starting more than 24 h after treatment and lasting for up to several days) [1]. The time course and severity of CINV vary depending on the specific chemotherapeutic agents administered, their dosages and routes of administration, and patient factors such as age, gender, history of alcohol use, and type of cancer [1–3]. Delayed CINV, which tends to be more common than acute CINV, is less responsive to antiemetic therapy [4, 5]. Delayed nausea also tends to be more severe than acute nausea [4, 5]. Although delayed nausea can occur in the absence of acute CINV [6], both types are important targets for antiemetic therapy because the risk of delayed CINV is greater if acute CINV is poorly controlled [7]. Further, the risk of CINV in general is highly related to its occurrence in a previous cycle of chemotherapy [8, 9].
Adverse consequences of CINV may include metabolic derangements, nutritional deficiencies and anorexia, esophageal tears, wound dehiscence, deterioration of performance and mental status, and degeneration of self-care and functional ability [1]. Further, CINV may lead to the discontinuation of potentially beneficial or curative anticancer treatments [1] and significantly affects quality of life [9]. Controlling CINV is therefore integral to treatment success in patients with cancer.
The first generation of 5HT3 receptor antagonists (5HT3 RAs), such as ondansetron, dolasetron, and granisetron revolutionized CINV management. These antiemetic agents are broadly effective in controlling acute CINV associated with moderately (MEC) or highly emetogenic chemotherapy (HEC) [10].
The 5HT3 RA palonosetron differs from other 5HT3 RAs in its pharmacokinetic/pharmacodynamic profile and may be uniquely suited to treat delayed CINV. Specifically, palonosetron has a longer elimination half-life (t ½) and a distinctly different receptor-binding profile compared with older 5HT3 RAs [11], uniquely triggers 5HT3 receptor internalization, and induces prolonged inhibition of receptor function [12]. Palonosetron also inhibits substance P responses in a serotonin-independent manner [13].
In the clinical setting, palonosetron improved rates of CINV prevention relative to older 5HT3 RAs in four phase III trials in patients receiving either MEC (30–90 % frequency of emesis) [14, 15] or HEC (>90 % frequency of emesis) [16, 17]. The present analysis utilized pooled data from these four trials to compare the relative effectiveness of palonosetron versus older 5HT3 RAs for preventing CINV in patients with cancer scheduled to receive either MEC or HEC and to compare the tolerability of palonosetron with that of older 5HT3 RAs. These studies were selected because patient-level data were available for analysis.
Patients and methods
Pooled patient-level data from four multicenter, randomized, double-blind, parallel-group phase III trials were analyzed (Table 1). Two of the trials were conducted in patients scheduled to receive MEC [14, 15] and two in patients scheduled to receive HEC [16, 17]. Of note, 64 % of patients in the study by Eisenberg et al. received anthracycline + cyclophosphamide (AC) [15], which is currently classified as HEC [1] (at the time of the study, AC was classified as MEC). Three trials were conducted in Europe or North America [14–16] and one in Japan [17]. All four studies were approved by institutional review boards or independent ethics committees at each site where they were performed. Written informed consent was obtained from all participating patients before any study-related procedure was initiated.
Methods of included trials
The methods for each study have been described in detail [14–17]. Briefly, patients enrolled in the four studies were required to be at least 18 years of age, have a histologically or cytologically confirmed malignancy, and have a Karnofsky Performance Scale score of ≥50 %. Eligible patients were randomly assigned to receive single intravenous (IV) doses of palonosetron (0.25 or 0.75 mg) or older 5HT3 RAs: ondansetron (32 mg), dolasetron (100 mg), and granisetron (40 μg/kg), all of which were administered 30 min before the scheduled chemotherapy regimens. Consistent with guidelines at the time of the studies, concomitant steroids were permitted [15, 16] or required [17] in three of the four studies. In each study, the primary efficacy endpoint was the complete response (CR) rate (defined as no emesis and no rescue medication) in the acute (0–24 h), delayed (>24–120 h), and/or overall (0–120 h) postchemotherapy treatment periods. Secondary efficacy endpoints included the complete control (CC) rate (defined as no emesis, no rescue medication, and no more than mild nausea) during the acute, delayed, and overall postchemotherapy treatment periods; numbers of emetic and nausea episodes; and nausea severity (rated on a four-point Likert scale from 0 = none to 3 = severe). Safety assessments included adverse events (AEs), vital signs, laboratory test results, and electrocardiographic (ECG) findings.
Statistical analysis
For this analysis, data from patients treated with ondansetron, dolasetron, or granisetron were pooled, and all data from all patients treated with palonosetron were pooled. Because the older 5HT3 RAs have similar efficacy in preventing CINV when administered at therapeutically equivalent doses [10], pooling of the data for these agents was considered valid. Similarly, as there are few differences in efficacy between the 0.25- and 0.75-mg doses of palonosetron [14–16], pooling of data for the two doses was also considered valid.
A logistic regression model was used to analyze pooled data from the four phase III trials and was fitted for CR and CC endpoints with terms for palonosetron 0.25, palonosetron 0.75, HEC, MEC, and Japanese study. In addition, a goodness-of-fit test (Hosmer–Lemeshow) was applied to ensure the consistency of effect of the endpoint across various strata of variables in the model. Interaction terms were assessed for significance. If the term was deemed not significant, it was removed from the model. The model was then refitted, and the model-fit and goodness-of-fit tests were reapplied. This process was repeated, eliminating each nonsignificant variable, one at a time, until all nonsignificant variables had been eliminated or the Hosmer–Lemeshow goodness-of-fit test had become significant. The process also was repeated for the subgroups of patients who had lung cancer or breast cancer. For descriptive purposes, if both the model-fit and Hosmer–Lemeshow goodness-of-fit tests were statistically significant (suggesting poor model fit across the strata, even though the model fit was good), the statistically significant model was displayed with a note of pooled consistency of fit across various strata (i.e., a statistically significant Hosmer–Lemeshow goodness-of-fit test statistic).
Observed rates of each efficacy outcome were compared between the palonosetron (pooled doses) and older 5HT3 RA groups using Cochran–Mantel–Haenszel tests.
For the safety analyses, a comparative descriptive assessment of AE rates in the four studies was performed.
Results
A total of 2,962 patients were included in the analysis: 1,787 received palonosetron and 1,175 received older 5HT3 RAs. Demographic and clinical characteristics of the analysis population are shown in Table 2. Data are shown separately for MEC and HEC studies. Additionally, data are shown for patients who received AC treatment in any study. Mean body weight was slightly lower in the groups containing Japanese patients in the study of HEC-induced CINV [17]. The majority of patients receiving HEC also received a corticosteroid (dexamethasone) concomitantly, while the majority of patients receiving MEC did not (Table 2); all patients in the Saito et al. study [17], approximately 67 % of patients in the Aapro et al. study [16], 5 % of patients in the Eisenberg et al. study [15]), and no patients in the Gralla et al. study [14] received corticosteroids.
Complete response rates
CR rates were significantly higher for palonosetron (pooled doses) relative to older 5HT3 RAs during the delayed phase (P < 0.0001), and overall phase (P < 0.0001), but not the acute phase (P = 0.091) (Fig. 1a). Likewise, odds ratios (ORs, 95 % CI) reflected a significantly greater likelihood of CR with palonosetron versus older 5HT3 RAs in the delayed (OR, 1.62 [1.40–1.88]) and overall phases (OR, 1.56 [1.34–1.81]), but not the acute phase (OR, 1.15 [0.98–1.34]).

a, b Complete response rates for all patients/complete control rates for all patients. a Significant differences between the palonosetron and other 5HT3 RAs groups were observed in the delayed and overall phases. Complete response no emetic episodes and no usage of rescue medication, PALO palonosetron, other 5HT 3 RAs other 5HT3 receptor antagonists (ondansetron, dolasetron, and granisetron). *P < 0.0001, palonosetron versus other 5HT3 RAs. b Significant differences between the palonosetron and other 5HT3 RAs groups were observed in the delayed and overall phases. Complete control no emetic episodes, no usage of rescue medication, and no more than mild nausea; PALO palonosetron; other 5HT 3 RAs other 5HT3 receptor antagonists (ondansetron, dolasetron, and granisetron). *P < 0.0001, palonosetron versus other 5HT3 RAs
Complete control rates
Analysis of the CC data showed that palonosetron provided higher CC rates than older 5HT3 RAs in the delayed (P < 0.0001) and overall (P < 0.0001) phases, but not the acute phase (P = 0.137) (Fig. 1b). ORs (95 % CI) for the acute, delayed, and overall phases were 1.12 (0.96–1.31), 1.49 (1.29–1.73), and 1.50 (1.29–1.74), respectively.
Number of emetic episodes
The frequency of emetic episodes was significantly different for palonosetron and older 5HT3 RAs during the acute (P = 0.007), delayed (P < 0.0001), and overall (P < 0.0001) phases (Fig. 2).

Episodes of emesis in the acute, delayed, and overall postchemotherapy phases. Significant differences between the palonosetron and other 5HT3 RAs groups were observed in the acute, delayed, and overall phases. PALO palonosetron, other 5HT 3 RAs other 5HT3 receptor antagonists (ondansetron, dolasetron, and granisetron). *P = 0.0066, palonosetron versus other 5HT3 RAs; † P < 0.0001, palonosetron versus other 5HT3 RAs
Frequency and severity of nausea episodes
The severity of nausea episodes was not significantly different with palonosetron and older 5HT3 RAs during the acute postchemotherapy phase (P = 0.165). However, there were significant differences in the delayed (P = 0.0002) and overall phases (P = 0.011) (Fig. 3). In terms of frequency of nausea, in the acute phase, 56 % of the palonosetron group and 54 % of the older 5HT3 RA group reported no episodes of nausea; in the delayed phase, the rates were 44 and 36 %, respectively, and in the overall phase, the rates were 39 and 33 %, respectively.

Severity of nausea in the acute, delayed, and overall postchemotherapy phases. Significant differences between the palonosetron and other 5HT3 RAs groups were observed in the delayed and overall phases. PALO palonosetron, other 5HT3 RAs other 5HT3 receptor antagonists (ondansetron, dolasetron, and granisetron). *P = 0.0002, palonosetron versus other 5HT3 RAs; † P = 0.0112, palonosetron versus other 5HT3 RAs
Safety and tolerability
The incidence of treatment-related AEs was similar for the three overall treatment groups: palonosetron 0.25 mg (20.0 %), palonosetron 0.75 mg (26.5 %), and older 5HT3 RAs (27.5 %) (Table 3). The percentages of patients with treatment-related AEs was less than one third of the percentages of patients with all-cause AEs, suggesting that most reported AEs were likely due to the patients’ cancer and/or the chemotherapy regimens (Table 3). The most common treatment-related AEs were constipation (palonosetron 0.25 mg [4.4 %], palonosetron 0.75 mg [11.5 %], older 5HT3 RAs [9.2 %]) and headache (palonosetron 0.25 mg [9.0 %], palonosetron 0.75 mg [7.4 %], older 5HT3 RAs [7.4 %]) (Table 3).
Discussion
This analysis of pooled patient-level data from four multicenter, phase III, randomized, double-blind, comparative trials demonstrates that palonosetron has a safety profile similar to that of older 5HT3 RAs but provides superior prophylaxis of CINV. Palonosetron demonstrated significantly higher complete response (CR) and complete control (CC) rates than older 5HT3 RAs (ondansetron, dolasetron, and granisetron) during the delayed (>24-120 h), and overall (0–120 h) postchemotherapy periods. The number of emetic episodes and severity of nausea were also significantly different for palonosetron compared with older 5HT3 RAs.
The most noteworthy differences between palonosetron and older 5HT3 RAs occurred in the delayed phase and throughout the overall 5-day evaluation period. Palonosetron therefore provides an effective option for delayed onset CINV, an effect of chemotherapy that previously had been more difficult to manage due to the limited efficacy of older 5HT3 RAs in this context [5, 6]. Further, palonosetron may be more effective in controlling nausea [18] (particularly delayed nausea), which remains a challenge despite the antiemetic efficacy of the older 5HT3 RAs [19, 20]. The observed advantage of palonosetron in efficacy during the delayed phase may be explained by differences in binding characteristics of palonosetron (i.e., a longer elimination half-life relative to other 5HT3 RAs [11] and triggering of receptor internalization leading to prolonged inhibition of receptor function and NK1 cross talk [12]). All of the studies evaluated outcomes following a single dose of palonosetron or other 5HT3 RAs given on day 1 of chemotherapy; outcomes may differ with the use of multi-day antiemetic treatment regimens.
The incidence of treatment-related AEs with palonosetron in this analysis was similar to that of older 5HT3 RAs, with a lower incidence of AEs associated with the 0.25 mg dose of palonosetron relative to the 0.75 mg dose. The most common treatment-related AEs were constipation and headache. Safety concerns with 5HT3 RAs include the potential for QTc prolongation [21], which has been the subject of recent safety communications from the US FDA (dolasetron: http://www.fda.gov/Drugs/DrugSafety/ucm237081.htm; ondansetron: http://www.fda.gov/Drugs/DrugSafety/ucm271913.htm). Notably, QTc prolongation with ondansetron appears to be dose dependent, which led to the removal of the 32-mg IV single daily dose from the ondansetron label (http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm310219.htm). IV dolasetron is no longer recommended due to an increased risk of cardiac arrhythmias [1]. Notably, recent studies evaluating the electrocardiographic effects of palonosetron in cancer patients found no significant changes in QTc interval [22, 23], and a thorough ECG study using moxifloxacin as a positive control found that doses up to 2.25 mg were not associated with clinically significant changes in QTc or other ECG parameters [24].
The efficacy findings are similar to those reported in other recent meta-analyses of the efficacy of palonosetron versus older 5HT3 RAs (ondansetron, dolasetron, and granisetron) in preventing CINV in patients receiving MEC or HEC [25–27]. For example, the analysis by Botrel, which included data from 2,057 patients from five randomized, double-blind, comparative trials, showed that palonosetron 0.25 mg is significantly more effective than older 5HT3 RAs in preventing both acute and delayed nausea and vomiting, regardless of the concomitant use of corticosteroids [25]. The relative risks (RRs, 95 % CI) were 0.86 (0.76–0.96, P = 0.007) for acute nausea, 0.82 (0.75–0.89; P < 0.00001) for delayed nausea, 0.76 (0.66–0.88; P = 0.0002) for acute vomiting, and 0.76 (0.68–0.85, P < 0.00001) for delayed vomiting [25]. Likun et al. [27] analyzed data from eight clinical trials (n = 3,592) and found that palonosetron (0.25 and 0.75 mg, combined) was significantly more effective than first-generation 5HT3 RAs in preventing CINV in the acute (OR: 0.76 [0.66–0.88], P = 0.0003), delayed (OR: 0.62 [0.54–0.71], P < 0.00001), and overall phases (OR 0.64 [0.56–0.74], P < 0.00001). Most recently, an analysis of data from nine studies (n = 3,463) demonstrated significantly greater efficacy with palonosetron 0.25 mg (based on RR for complete response) compared with first-generation 5HT3 RAs in the acute (1.11 [1.05–1.17]), delayed (1.26 [1.16–1.36]), and overall phases (1.25 [1.14–1.37]) [26]. Results were similar for palonosetron 0.75 mg [26]. These previous meta-analyses included data from the four studies analyzed here, as well as data from additional studies. Limiting our analysis to the pivotal clinical trials that formed the basis for FDA approval of palonosetron potentially introduces some degree of bias, as not all publicly available data were included. Other meta-analyses, which analyzed both abstracted (literature-based) data and patient-level data, yielded similar results, demonstrating similar efficacy and safety of the 0.25 and 0.75 mg doses of palonosetron. This analysis is generally in agreement with other meta-analyses and utilizes patient-level data to demonstrate a benefit for palonosetron compared with older 5HT3 RAs. We would not expect substantially different results were the other published studies included.
The overall body of evidence supporting the efficacy of palonosetron in managing CINV has led to its inclusion in several clinical practice guidelines. Specifically, the Multinational Association of Supportive Care in Cancer (MASCC), the European Society of Medical Oncology (ESMO) [19], the American Society of Clinical Oncology (ASCO) [20], and the National Comprehensive Cancer Network (NCCN) [1] recommend palonosetron as the preferred 5HT3 RA for prevention of CINV associated with MEC. In addition, MASCC and ESMO recommend palonosetron as the preferred 5HT3 RA for AC (doxorubicin or epirubicin and cyclophosphamide) regimens when an NK1 RA is not available [19]. MASCC/ESMO and ASCO guidelines recommend palonosetron among other 5HT3 RAs for HEC [19, 20], while NCCN guidelines denote palonosetron 0.25 mg as the preferred 5HT3 RA for acute and delayed emesis prevention during intravenous chemotherapy with high emetic risk [1]. Adherence to practice guidelines improves CINV prevention outcomes; a recent study demonstrated that guideline-consistent CINV prophylaxis was associated with significantly greater odds of CR (OR 1.43 [1.04–1.97]; P = 0.027) [28].
The substantial economic burden associated with management of CINV includes resource utilization and costs related to inpatient, outpatient, and emergency department visits [29, 30]. Improved CINV prevention, therefore, may result in economic benefits. For example, among patients with breast or lung cancer on HEC or MEC, the risk of CINV events requiring hospital or emergency department visits was significantly reduced with palonosetron as compared to other 5-HT3 RA-based regimens [31]. Another study demonstrated that palonosetron was associated with significantly fewer extreme CINV events, resulting in a substantial reduction in both the use of rescue antiemetics and staff management time [32]. In addition, because patients who experience CINV during one cycle of chemotherapy are more likely to experience CINV in subsequent cycles [33], the economic benefits of preventing CINV during an initial cycle of chemotherapy would be expected to extend to subsequent cycles.
In summary, the data from the current analysis support previous findings of improved prevention of CINV relative to older 5HT3 RAs and further demonstrate an advantage of palonosetron in preventing delayed CINV. Improved prophylaxis against CINV, especially in the first cycle of chemotherapy, might provide additional benefit in helping to prevent the occurrence of CINV in subsequent cycles of chemotherapy, thereby facilitating treatment adherence.
References
National Comprehensive Cancer Network (2012). NCCN clinical practice guidelines in oncology (NCCN Guidelines™): antiemesis. v1.2012. National Comprehensive Cancer Network, Fort Washington, PA
Roscoe JA, Morrow GR, Colagiuri B, Heckler CE, Pudlo BD, Colman L, Hoelzer K, Jacobs A (2010) Insight in the prediction of chemotherapy-induced nausea. Support Care Cancer 18:869–876
Grunberg SM, Warr D, Gralla RJ, Rapoport BL, Hesketh PJ, Jordan K, Espersen BT (2011) Evaluation of new antiemetic agents and definition of antineoplastic agent emetogenicity—state of the art. Support Care Cancer 19(suppl 1):S43–S47
Hickok JT, Roscoe JA, Morrow GR, Bole CW, Zhao H, Hoelzer KL, Dakhil SR, Moore T, Fitch TR (2005) 5-Hydroxytryptamine-receptor antagonists versus prochlorperazine for control of delayed nausea caused by doxorubicin: a URCC CCOP randomised controlled trial. Lancet Oncol 6:765–772
Hickok JT, Roscoe JA, Morrow GR, King DK, Atkins JN, Fitch TR (2003) Nausea and emesis remain significant problems of chemotherapy despite prophylaxis with 5-hydroxytryptamine-3 antiemetics: a University of Rochester James P. Wilmot Cancer Center Community Clinical Oncology Program Study of 360 cancer patients treated in the community. Cancer 97:2880–2886
Grunberg SM, Deuson RR, Mavros P, Geling O, Hansen M, Cruciani G, Daniele B, De PG, Rubenstein EB, Daugaard G (2004) Incidence of chemotherapy-induced nausea and emesis after modern antiemetics: perception versus reality. Cancer 100:2261–2268
Gralla RJ, Osoba D, Kris MG, Kirkbride P, Hesketh PJ, Chinnery LW, Clark-Snow R, Gill DP, Groshen S, Grunberg S, Koeller JM, Morrow GR, Perez EA, Silber JH, Pfister DG (1999) Recommendations for the use of antiemetics: evidence-based, clinical practice guidelines. Am Soc Clin Oncol J Clin Oncol 17:2971–2994
Morrow G, Roscoe JA, Hickok JT, Stern RM, Pierce HI, King DB, Banerjee TK, Weiden P (1998) Initial control of chemotherapy-induced nausea and vomiting in patient quality of life. Oncology (Williston Park) 12:32–37
Cohen L, de Moor CA, Eisenberg P, Ming EE, Hu H (2007) Chemotherapy-induced nausea and vomiting: Incidence and impact on patient quality of life at community oncology settings. Support Care Cancer 15:497–503
Hesketh PJ (2000) Comparative review of 5-HT3 receptor antagonists in the treatment of acute chemotherapy-induced nausea and vomiting. Cancer Invest 18:163–173
Rojas C, Stathis M, Thomas AG, Massuda EB, Alt J, Zhang J, Rubenstein E, Sebastiani S, Cantoreggi S, Snyder SH, Slusher B (2008) Palonosetron exhibits unique molecular interactions with the 5-HT3 receptor. Anesth Analg 107:469–478
Rojas C, Thomas AG, Alt J, Stathis M, Zhang J, Rubenstein EB, Sebastiani S, Cantoreggi S, Slusher BS (2010) Palonosetron triggers 5-HT(3) receptor internalization and causes prolonged inhibition of receptor function. Eur J Pharmacol 626:193–199
Rojas C, Slusher BS (2012) Pharmacological mechanisms of 5-HT3 and tachykinin NK1 receptor antagonism to prevent chemotherapy-induced nausea and vomiting. Eur J Pharmacol 684:1–7
Gralla R, Lichinitser M, Van der Vegt S, Sleeboom H, Mezger J, Peschel C, Tonini G, Labianca R, Macciocchi A, Aapro M (2003) Palonosetron improves prevention of chemotherapy-induced nausea and vomiting following moderately emetogenic chemotherapy: results of a double-blind randomized phase III trial comparing single doses of palonosetron with ondansetron. Ann Oncol 14:1570–1577
Eisenberg P, Figueroa-Vadillo J, Zamora R, Charu V, Hajdenberg J, Cartmell A, Macciocchi A, Grunberg S (2003) Improved prevention of moderately emetogenic chemotherapy-induced nausea and vomiting with palonosetron, a pharmacologically novel 5-HT3 receptor antagonist: results of a phase III, single-dose trial versus dolasetron. Cancer 98:2473–2482
Aapro M, Grunberg S, Manikhas G, Olivares G, Suarez T, Tjulandin S, Bertoli L, Yunus F, Morrica B, Lordick F, Macciocchi A (2006) A phase III, double-blind, randomized trial of palonosetron compared with ondansetron in preventing chemotherapy-induced nausea and vomiting following highly emetogenic chemotherapy. Ann Oncol 17:1441–1449
Saito M, Aogi K, Sekine I, Yoshizawa H, Yanagita Y, Sakai H, Inoue K, Kitagawa C, Ogura T, Mitsuhashi S (2009) Palonosetron plus dexamethasone versus granisetron plus dexamethasone for prevention of nausea and vomiting during chemotherapy: a double-blind, double-dummy, randomised, comparative phase III trial. Lancet Oncol 10:115–124
Sato Y, Hayakawa Y, Tatematsu M, Muro K, Noma H, Okamoto H (2012) Antiemetic effect of palonosetron in advanced colorectal cancer patients receiving mFOLFOX6 and FOLFIRI: a retrospective survey. Article in Japanese. Gan To Kagaku Ryoho 39:1215–1219
Roila F, Herrstedt J, Aapro M, Gralla RJ, Einhorn LH, Ballatori E, Bria E, Clark-Snow RA, Espersen BT, Feyer P, Grunberg SM, Hesketh PJ, Jordan K, Kris MG, Maranzano E, Molassiotis A, Morrow G, Olver I, Rapoport BL, Rittenberg C, Saito M, Tonato M, Warr D (2010) Guideline update for MASCC and ESMO in the prevention of chemotherapy- and radiotherapy-induced nausea and vomiting: results of the Perugia consensus conference. Ann Oncol 21(suppl 5):v232–v243
Basch E, Prestrud AA, Hesketh PJ, Kris MG, Feyer PC, Somerfield MR, Chesney M, Clark-Snow RA, Flaherty AM, Freundlich B, Morrow G, Rao KV, Schwartz RN, Lyman GH (2011) Antiemetics: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol 29:4189–4198
Benedict CR, Arbogast R, Martin L, Patton L, Morrill B, Hahne W (1996) Single-blind study of the effects of intravenous dolasetron mesylate versus ondansetron on electrocardiographic parameters in normal volunteers. J Cardiovasc Pharmacol 28:53–59
Yavas C, Dogan U, Yavas G, Araz M, Ata OY (2011) Acute effect of palonosetron on electrocardiographic parameters in cancer patients: a prospective study. Support Care Cancer 20:2343–2347
Gonullu G, Demircan S, Demirag MK, Erdem D, Yucel I (2012) Electrocardiographic findings of palonosetron in cancer patients. Support Care Cancer 20:1435–1439
Morganroth J, Parisi S, Moresino C, Thorn M, Cullen MT (2007) High dose palonosetron does not alter ECG parameters including QTc interval in healthy subjects: results of a dose–response, double blind, randomized, parallel El4 study of palonosetron vs. moxifloxacin or placebo [abstract]. Eur J Cancer Suppl 5:158–159
Botrel TE, Clark OA, Clark L, Paladini L, Faleiros E, Pegoretti B (2011) Efficacy of palonosetron (PAL) compared to other serotonin inhibitors (5-HT3R) in preventing chemotherapy-induced nausea and vomiting (CINV) in patients receiving moderately or highly emetogenic (MoHE) treatment: systematic review and meta-analysis. Support Care Cancer 19:823–832
Jin Y, Sun W, Gu D, Yang J, Xu Z, Chen J (2013) Comparative efficacy and safety of palonosetron with the first 5-HT3 receptor antagonists for the chemotherapy-induced nausea and vomiting: a meta-analysis. Eur J Cancer Care (Engl) 22:41–50
Likun Z, Xiang J, Yi B, Xin D, Tao ZL (2011) A systematic review and meta-analysis of intravenous palonosetron in the prevention of chemotherapy-induced nausea and vomiting in adults. Oncologist 16:207–216
Aapro M, Molassiotis A, Dicato M, Pelaez I, Rodriguez-Lescure A, Pastorelli D, Ma L, Burke T, Gu A, Gascon P, Roila F (2012) The effect of guideline-consistent antiemetic therapy on chemotherapy-induced nausea and vomiting (CINV): the Pan European Emesis Registry (PEER). Ann Oncol 23:1986–1992
Burke TA, Wisniewski T, Ernst FR (2011) Resource utilization and costs associated with chemotherapy-induced nausea and vomiting (CINV) following highly or moderately emetogenic chemotherapy administered in the US outpatient hospital setting. Support Care Cancer 19:131–140
Craver C, Gayle J, Balu S, Buchner D (2011) Clinical and economic burden of chemotherapy-induced nausea and vomiting among patients with cancer in a hospital outpatient setting in the United States. J Med Econ 14:87–98
Hatoum HT, Lin SJ, Buchner D, Cox D (2012) Comparative clinical effectiveness of various 5-HT3 RA antiemetic regimens on chemotherapy-induced nausea and vomiting associated with hospital and emergency department visits in real world practice. Support Care Cancer 20:941–949
Feinberg BA, Gilmore J, Haislip S, Gondesen T, Saleh MN, Lenz WH (2009) Data-driven medical decision-making in managing chemotherapy-induced nausea and vomiting. Commun Oncol 6:62–67
Schwartzberg L, Szabo S, Gilmore J, Haislip S, Jackson J, Jain G, Balu S, Buchner D (2011) Likelihood of a subsequent chemotherapy-induced nausea and vomiting (CINV) event in patients receiving low, moderately or highly emetogenic chemotherapy (LEC/MEC/HEC). Curr Med Res Opin 27:837–845
Acknowledgments
The authors wish to thank Sherri Jones, PharmD, of MedVal Scientific Information Services, LLC, for providing medical writing and editorial assistance, which was funded by Eisai Inc. This manuscript was prepared according to the International Society for Medical Publication Professionals’ Good Publication Practice for Communicating Company-Sponsored Medical Research: the GPP2 Guidelines. This study was sponsored by Eisai Inc., Woodcliff Lake, NJ, USA.
Conflict of interest
The authors disclose the following conflicts of interest: LS: a consultant for Eisai Inc; SYB: none; GRM: none; GB: an employee of Helsinn Healthcare SA; MDT: a consultant for Helsinn Healthcare SA and Lugano Switzerland; and DC: an employee of Eisai Inc.
Authorship contributions
All authors contributed equally and each was involved in study design, data acquisition, or data analysis/interpretation and in drafting or critically revising the manuscript. All authors reviewed the final manuscript and gave approval for submission.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
About this article
Cite this article
Schwartzberg, L., Barbour, S.Y., Morrow, G.R. et al. Pooled analysis of phase III clinical studies of palonosetron versus ondansetron, dolasetron, and granisetron in the prevention of chemotherapy-induced nausea and vomiting (CINV). Support Care Cancer 22, 469–477 (2014). https://doi.org/10.1007/s00520-013-1999-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-013-1999-9