
Abstract
Goal
Oral-dental infection foci should be eradicated before the ablative chemo-radiotherapy regimen of hematopoietic stem cell transplantation (HSCT) commences. The rationale of oral-dental treatment is to prevent the future development and spread of infections in patients with compromised immune systems. This study aims to shed light on the challenges facing hospital dentists in the implementation of optimal oral-dental treatment prior to HSCT.
Patients and methods
Data regarding the medical status and dental treatment needs before HSCT were retrieved from the files of 86 consecutive patients post-HSCT. The timing of the oral-dental examination was also recorded.
Main results
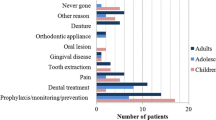
Dental treatments required before the HSCT were mainly combinations of scaling, plastic fillings, and extractions (47.8%, 39.1%, and 19.5% of the patients respectively). Patients presented at the clinic for oral-dental examination an average of 20.65±16.82 days before HSCT with a median of 15 (quarter interval range 10–15) days.
Conclusions
Our data indicate a dense distribution of dental needs preceding the ablative conditioning regimen for HSCT. These facts accentuate the vital need for cooperation between hospital dentists and treating physicians.
Similar content being viewed by others


References
Barker JG (1999) Current practices in the oral management of the patient undergoing chemotherapy or bone marrow transplantation. Supp Care Cancer 7:17–20
Gratwohl A (2002) The role of the EBMT activity survey in the management of hematopoietic stem cell transplantation. European Group for Blood Marrow. Int J Hematol 76(1):386–392
Greenberg MS (1990) Prechemotherapy dental treatment to prevent bacteremia. NCI Monogr 9:39–41
Hupp JR (2003) Wound Repair. In: Peterson LJ, Ellis E, Hupp JR, Tucker M (eds) Contemporary oral and maxillofacial surgery. Mosby, St. Louis, MO pp 49–59
Lazarchik DA, Filler SJ, Winkler MP (1995) Dental evaluation in bone marrow transplantation. Gen Dent 43(4):369–371
Little JW, Falace DA, Miller CS, Rhodus NL (1997) Dental Management of the medically compromised patient/blood dyscrasias. Mosby, St. Louis, MO
Miller CS, Epstein JB, Hall EH (2001) Changing oral care needs in the United States: The continuing need for oral medicine. Oral Surg Oral Med Oral Pathol 91(1):34–44
Peterson DE (1990) Pretreatment strategies for infection prevention in chemotherapy patients. NCI Monogr 9:61–71
Raut A, Huryn JM, Hwang FR (2001) Sequelae and complications related to dental extractions in patients with hematologic malignancies and the impact on medical outcome. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 92(1):49–55
Schubert MM (1999) Oral complications. In: Thomas ED, Blume KG, Forman SJ (eds) Hematopoietic cell transplantation. Blackwell Science, Malden, MA pp 751–763
Sonis ST, Woods PD, White BA (1990) Oral complications of cancer therapies. Pretreatment oral assessment. NCI Monogr 9:29–32
Stevenson-Moore P (1990) Oral complications of cancer therapies. Essential aspects of a pretreatment oral examination. NCI Monogr 9:33–36
Woo S and Matin K (1997) Off-site dental evaluation program for prospective bone marrow transplant recipients. JADA 128:189–193
Acknowledgment
We would like to thank Dr. Sharon D.M. Robinson for the editorial assistance.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Elad, S., Garfunkel, A.A., Or, R. et al. Time limitations and the challenge of providing infection-preventing dental care to hematopoietic stem-cell transplantation patients. Support Care Cancer 11, 674–677 (2003). https://doi.org/10.1007/s00520-003-0499-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-003-0499-8