
Summary
Background
Viral or bacterial upper respiratory infections are the most common cause of acute exacerbation of chronic obstructive pulmonary disease (AECOPD). Based on available data, no reliable parameter has been presented to distinguish between bacterial and nonbacterial exacerbations. Therefore, we compared the diagnostic value of procalcitonin (PCT) level, which is a newer marker for predicting bacterial infections in patients with AECOPD, to routine parameters such as C-reactive protein (CRP) levels and the neutrophil/lymphocyte (N/L) ratio.
Methods
This study included all consecutive patients who were admitted for a diagnosis of AECOPD between January 1 and March 31, 2014. PCT, CRP, and the N/L ratio were assessed in addition to cultures from tracheal aspirates or sputum on the first day of admission. Patients with a pneumonic infiltration on chest radiographs, or an extrapulmonary infection focus, or whose blood samples were not obtained for PCT and/or CRP at the same time as sputum culture were excluded from the study.
Results
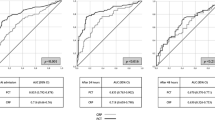
A total of 77 patients were included with a mean age of 71.7 ± 9.5 years. Bacteria were isolated in 37.4 % of the patients. Mean PCT levels were significantly higher in patients with positive sputum cultures than in patients with negative sputum cultures. The cut-off values for PCT, CRP, and the N/L ratio for predicting a bacterial infection were 0.40 ng/mL, 91.50 mg/L, and 11.5, respectively; sensitivity was 61, 54, and 61 % respectively; specificity was 67, 52, and 58 %, respectively; and the area under the curve (AUC) values were 0.64, 0.52, and 0.58, respectively. The AUC value of PCT was significantly better for predicting bacterial infection compared with the CRP level or the N/L ratio (p = 0.042).
Conclusion
PCT was better than CRP and the N/L ratio for predicting a bacterial infection in hospitalized patients with AECOPD. However, we find PCT not so reliable in predicting bacterial infection in AECOPD due to sensitivity and specificity of less than 80 % and a low AUC value.
Zusammenfassung
Hintergrund
Virale oder bakterielle Infektionen des oberen Respirationstraktes sind die häufigste Ursache einer akuten Exazerbation einer chronisch obstruktiven Lungenerkrankung (COPD). Bis jetzt ist kein verlässlicher Parameter bekannt, der in der Lage ist, zwischen bakteriellen und nicht-bakteriellen Exazerbationen zu unterscheiden. Wir haben daher den diagnostischen Wert der Konzentrationen von Procalcitonin (PCT), einem neueren Marker zur Vorhersage bakterieller Infektionen bei Patienten mit COPD, mit dem der herkömmlichen Routineparameter, wie dem C-reaktivem Protein (CRP) und dem Neutrophilen/Lymphozyten (N/L) Quotienten, verglichen.
Methoden
Diese Studie schloss alle konsekutiven Patienten ein, die mit der Diagnose einer COPD zwischen 1. Jänner und 31. März 2014 aufgenommen waren. PCT, CRP und die N/L Quotienten wurden zusätzlich zu Kulturen von Aspiraten aus der Trachea oder von Sputa am Aufnahmetag erhoben. Patienten mit einem Lungeninfiltrat oder einem extrapulmonalen Infektionsherd und/oder deren Blutproben nicht am selben Tag wie die Sputum Kulturen abgenommen waren, wurden aus der Studie ausgeschlossen.
Ergebnisse
Siebenundsiebzig Patienten mit einem mittlerem Alter von 71,7 ± 9,5 Jahren wurden in die Studie aufgenommen. Bei 37,4 % der Patienten konnten Bakterien isoliert werden. Die mittleren PCT Werte waren bei den Patienten mit positiven Sputum Kulturen signifikant höher als bei denen mit negativen Kulturen. Die Grenzwerte für die PCT, CRP und N/L Quotienten Werte zur Vorhersage eines bakteriellen Infektes lagen bei 0,40 ng/mL, 91,50 mg/L, und 11,5. Die Sensitivität war bei 61, 54, und 61 % – die Spezifität bei 67, 52, und 58 %, die Flächen unter der Kurve (AUC) 0,64, 0,52, and 0,58. Die AUC der PCT Werte war bei der Vorhersage von bakteriellen Infekten im Vergleich zu den CRP Werten und den N/L Quotienten signifikant besser (p = 0,042).
Schlussfolgerung
Bei Patienten mit COPD war das PCT bei der Vorhersage von bakteriellen Infekten besser als das CRP beziehungsweise die N/L Quotienten. Wir sind allerdings der Meinung, dass PCT kein sehr verlässlicher Parameter in der Vorhersage von bakteriellen Infekten ist, da sowohl die Spezifität als auch die Sensitivität unter 80 % liegen, und da auch die AUC niedrig ist.


Similar content being viewed by others


References
Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: updated 2014. http://www.goldcopd.org/uploads/users/files/GOLD_Report2014_Feb07.pdf. Accessed 30 April 2014.
Dev D, Wallace E, Sankaran R, et al. Value of C-reactive protein measurements in exacerbations of chronic obstructive pulmonary disease. Respir Med. 1998;92:664–7.
Torres A. COPD guidelines in relation to infections: a critical analysis. Breathe. 2009;5(4):317–32. doi:10.1183/18106838.0504.317.
Lacoma A, Prat C, Andreo F, et al. Value of procalcitonin, C-reactive protein, and neopterin in exacerbations of chronic obstructive pulmonary disease. Int J COPD. 2011;6:157–69.
Daniels JMA, Schoorl M, Snijders D, et al. Procalcitonin vs C-reactive protein as predictive markers of response to antibiotic therapy in acute exacerbations of COPD. Chest. 2010;138(5):1108–15.
Nuutilia J, Lilius EM. Distinction between bacterial and viral infections. Curr Opin Pulm Med. 2007;20:304–10.
Wedzicha JA. Exacerbations: etiology and pathophysiologic mechanisms. Chest. 2002;121:136–41.
Polzin A, Pletz M, Erbes R. Procalcitonin as a diagnostic tool in lower respiratory tract infections and tuberculosis. Eur Respir J. 2003;21:939–43. doi:10.1183/09031936.03.00055103
Antonescu-Turcu AL, Tomic R. C-reactive protein and copeptin: prognostic predictors in chronic obstructive pulmonary disease exacerbations. Curr Opin Pulm Med. 2009;15:120–5.
Günay E, Sarınç UlaşlıS, Akar O, et al. Neutrophil-to-lymphocyte ratio in chronic obstructive pulmonary disease: a retrospective study. Inflammation. 2014;37:2. doi:10.1007/s10753-013-9749-1.
Mohamed KH, Abderabo MM, Ramadan ES, et al. Procalcitonin as a diagnostic marker in acute exacerbation of COPD. Egypt J Chest Dis Tuberculosis. 2012;61:301–5.
Delèvaux I, André M, Colombier M, et al. Can procalcitonin measurement help in differentiating between bacterial infection and other kinds of inflammatory processes? Ann Rheum Dis. 2003;62:337–40.
Simon L, Gauvin F, Amre DK, et al. Serum procalcitonin and c-reactive protein levels as markers of bacterial infection: a systematic review and meta-analysis. Clin Infect Dis. 2004;39:206–17.
Daubin C, Parienti JJ, Vabret A, et al. Procalcitonin levels in acute exacerbation of COPD admitted in ICU: a prospective cohort study. BMC Infect Dis. 2008;8:145. doi:10.1186/1471-2334-8-145.
Ko FWS, Ng TKC, Li TST, et al. Sputum bacteriology in patients with acute exacerbations of COPD in Hong Kong. Respir Med. 2005;99:454–60.
Bafadhel M, Clark TW, Reid C, et al. Procalcitonin and C-reactive protein in hospitalized adult patients with community-acquired pneumonia or exacerbation of asthma or COPD. Chest. 2011;139(6):1410–8.
Kherad O, Bridevaux PO, Kaiser L, et al. Is acute exacerbation of COPD (AECOPD) related to viral infection associated with subsequent mortality or exacerbation rate? Open Respir Medi J. 2014;8:18–21.
Domenech A, Puig C, Martí S, et al. Infectious etiology of acute exacerbations in severe COPD patients. J Infect. 2013;67:516–23.
Lieberman D, Lieberman D, Ben-Yaakov M, et al. Infectious etiologies in acute exacerbation of COPD. Diagn Microbiol Infect Dis. 2001;40(3):95–102.
Peng C, Tian C, Zhang Y, et al. C-reactive protein levels predict bacterial exacerbation in patients with chronic obstructive pulmonary disease. Am J Med Sci. 2013;345(3):190–4.
Gaïni S, Koldkjaer OG, Pedersen C, Pedersen SS,. Procalcitonin, lipopolysaccharide-binding protein, interleukin-6 and C-reactive protein in community-acquired infections and sepsis: a prospective study. Crit Care. 2006;10(2):R53.
De Jager CPC, van Wijk PTL, Mathoera RB, et al. Lymphocytopenia and neutrophil-lymphocyte count ratio predict bacteremia better than conventional infection markers in an emergency care unit. Crit Care. 2010;14:R192.
Bartlett JG, Senthi S. Management of infection in exacerbations of chronic obstructive pulmonary disease. In Sexton JD, editor. UpToDate. Waltham. http://www.uptodate.com. Accessed 6 June 2014.
Syrjala H, Broas M, Suramo I, Ojala A, Lahde S. High-resolution computed tomography for the diagnosis of community-acquired pneumonia. Clin Infect Dis. 1998;27:358–63.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Tanrıverdi, H., Örnek, T., Erboy, F. et al. Comparison of diagnostic values of procalcitonin, C-reactive protein and blood neutrophil/lymphocyte ratio levels in predicting bacterial infection in hospitalized patients with acute exacerbations of COPD. Wien Klin Wochenschr 127, 756–763 (2015). https://doi.org/10.1007/s00508-014-0690-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00508-014-0690-6