
Abstract
Background
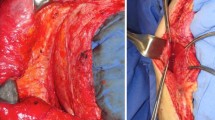
Proper defect closure during abdominal wall reconstruction (AWR) is a key to improving cosmetic and functional results, and reducing morbidity. We have completed the initial prospective evaluation of a technique we previously described and published: endoscopic subcutaneous anterior component separation (ACS) as an adjunct to mainly laparoscopic AWR. We now present the long-term clinical and imaging follow-up results.
Study design
Data were prospectively collected over a 3-year period (2012–2015) on patients who underwent AWR with endoscopic ACS. Inclusion criteria included the following: defects of 6–15 cm that are longer than wider; no skin dystrophy; no loss of domain; no active infection; no previous multiple, complex repairs; no previous multiple mesh repairs; and no high probability of severe adhesions. All patients were followed up clinically at 3, 6, and 12 months postoperatively and then annually. All patients underwent CT scanning of the abdominal wall (sagittal, axial, coronal, and 3D reconstruction) at 3 months and 1 year postoperatively and then annually.
Results
Twenty consecutive patients underwent adjunctive endoscopic ACS: 17 laparoscopic AWRs, 2 open repairs, and 1 hybrid repair. Up to 38 months (mean 21 months) of follow-up, there were no ventral hernia recurrences or de novo hernias at the ACS site. One patient experienced partial primary closure failure. Morbidity consisted in one case each of hematoma, seroma, and transient neuralgia. Cosmetic results and patient satisfaction were excellent.
Conclusion
We confirmed that endoscopic subcutaneous ACS is a safe, effective, reliable, reproducible technique that facilitates primary closure of defects during AWR in selected patients.



Similar content being viewed by others


References
Nguyen DH, Nguyen MT, Ashkenazy EP et al (2014) Primary fascial closure with laparoscopic ventral hernia repair: systematic review. World J Surg 38:3097–3104
Ramirez OM, Ruas E, Dellon AL (1990) “Components separation” method for closure of abdominal-wall defects: an anatomic and clinical study. Plast Reconstr Surg 86:519–526
Rosen MJ, Jin J, McGee MF et al (2007) Laparoscopic component separation in the single stage treatment of infected abdominal wall prosthetic removal. Hernia 11:435–440
Harth KC, Rosen MJ (2010) Endoscopic versus open component separation in complex abdominal wall reconstruction. Am J Surg 199:342–347
Daes J (2014) Endoscopic subcutaneous approach to component separation. J Am Col Surg. 218:e1–e4
Ferretis M, Orchard P (2015) Minimally invasive component separation techniques in complex ventral abdominal hernia repair: a systematic review of the literature. Surg Laparosc Endosc Percutan Tech 25:100–105
Daes J (2015) Standardization of hernia surgery (Letter to the Editor). Hernia 19:1039–1040
Clapp ML, Hicks SC, Awad SS, Liang MK (2013) Trans-cutaneous closure of central defects (TCCD) in laparoscopic ventral hernia repairs (LVHR). World J Surg 37:42–51
Banerjee A, Beck C, Narula VK et al (2012) Laparoscopic ventral hernia repair: does primary repair in addition to placement of mesh decrease recurrence? Surg Endosc 26:1264–1268
den Hartog D, Eker HH, Tuinebreijer WE et al (2010) Isokinetic strength of the trunk flexor muscles after surgical repair for incisional hernia. Hernia 14:243–247
Gunnarsson U, Johansson M, Strigard K (2011) Assessment of abdominal muscle function using the Biodex System-4. Validity and reliability in healthy volunteers and patients with giant ventral hernia. Hernia 15:417–421
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Authors Jorge Daes and Rodolfo J. Dennis have no conflicts of interest or financial ties to disclose pertaining to this publication.
Rights and permissions
About this article

Cite this article
Daes, J., Dennis, R.J. Endoscopic subcutaneous component separation as an adjunct to abdominal wall reconstruction. Surg Endosc 31, 872–876 (2017). https://doi.org/10.1007/s00464-016-5045-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-016-5045-0