
Abstract
Background and study aims
Conventional endoscopic resection (CER) includes polypectomy and endoscopic mucosal resection. The most common complications related to these techniques are post procedure bleeding and perforation. The aim of this study was to evaluate the outcomes of CER for colorectal neoplasms ≧20 mm and to clarify predictive factors for complications.
Patients and methods
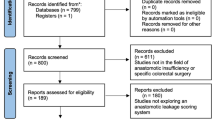
We conducted a multicenter prospective study at 18 specialized institutes. From October 2007 to December 2010, 1,029 CERs were performed at participating institutes. We collected the data prospectively and analyzed gender, age, tumor size, gross appearance, mode of resection, etc.
Results
The mean size of polyps resected was 26.4 ± 8.6 mm (range 20–120 mm). The final pathology was Vienna classification category 1 or 2 in 24, category 3 in 502, and category 4 or 5 in 503 lesions. Post procedure bleeding and intra procedure perforation occurred, respectively, in 16 (1.6 %) and 8 cases (0.78 %). The overall complication rate was 2.3 %. Risk factors for bleeding in multivariate analysis were only patients under 60 years of age. Risk factors for perforation in multivariate analysis were en bloc resection and Vienna classification category 4–5. The difference of complication rate was not statistically significant regarding gender, size, tumor location, gross appearance, treatment method, and kind of insufflation.
Conclusion
CER is a safe, efficient, and effective minimally invasive therapy for large colorectal lesions. However, care should be taken for post procedure bleeding in patients under 60 years of age and for perforation in cases of Vienna classification category 4–5 or when an en bloc resection is tried.

Similar content being viewed by others


References
Fukami N, Lee JH (2006) Endoscopic treatment of large sessile and flat colorectal lesions. Curr Opin Gastroenterol 22:54–59
Repici A, Pellicano R, Strangio G, Danese S, Fagoonee S, Malesci A (2009) Endoscopic mucosal resection for early colorectal neoplasia: pathologic basis, procedures, and outcomes. Dis Colon Rectum 52:1502–1515
Deyhle P, Largiader F, Fumagalli S (1973) A method for endoscopic electroresection of sessile colonic polyps. Endoscopy 5:38–40
Kudo SE (1993) Endoscopic mucosal resection of flat and depressed types of early colorectal cancer. Endoscopy 25:455–461
Kitajima K, Fujimori T, Fujii S et al (2004) Correlations between lymph node metastasis and depth of submucosal invasion in submucosal invasive colorectal carcinoma: a Japanese collaborative study. J Gastroenterol 39:534–543
Ono H, Kondo H, Gotoda T et al (2001) Endoscopic mucosal resection for treatment of early gastric cancer. Gut 48:225–229
Oka S, Tanaka S, Kaneko I et al (2006) Advantage of endoscopic submucosal dissection compared with EMR for early gastric cancer. Gastrointest Endosc 64:877–883
Tanaka S, Oka S, Chayama K (2008) Colorectal endoscopic submucosal dissection: present status and future perspective, including its differentiation from endoscopic mucosal resection. J Gastroenterol 43:641–651
Uraoka T, Kawahara Y, Kato J et al (2009) Endoscopic submucosal dissection in the colorectum: present status and future prospects. Dig Endosc 21(Suppl 1):S13–16
Sorbi D, Norton I, Conio M et al (2000) Postpolypectomy lower GI bleeding: descriptive analysis. Gastrointest Endosc 51:690–696
Church JM (2003) Experience in the endoscopic management of large colonic polyps. ANZ J Surg 73(12):988–995
Participants in the Paris Workshop (2003) The Paris endoscopic classification of superficial neoplastic lesions: esophagus, stomach, and colon—November 30 to December 1, 2002. Gastrointest Endosc 58(Suppl):3–43
Kudo SE, Lambert R, Allen J et al (2008) Nonpolypoid neoplastic lesions of the colorectal mucosa. Gastrointest Endosc 68(Suppl):3–29
Japanese society for cancer of the colon and rectum (2009) Japanese classification of colorectal carcinoma. Second English Edition. Kanehara & Co. Ltd., Tokyo
Schlemper RJ, Riddell RH, Kato Y et al (2000) The Vienna classification of gastrointestinal epithelial neoplasia. Gut 47:251–255
Rubio CA, Nesi G, Messerini L et al (2006) The Vienna classification applied to colorectal adenomas. J Gastroenterol Hepatol 21(11):1697–1703
Van Gossum A, Cozzoli A, Adler M et al (1992) Colonoscopic snare polypectomy: analysis of 1485 resections comparing two types of current. Gastrointest Endosc 38(4):472–475
Bedogni G, Bertoni G, Ricci E et al (1986) Colonic excision of large and giant colorectal polyps. Technical implications and results over eight years. Dis Colon Rectum 29(12):831–835
Metz AJ, Bourke ML, Moss A et al (2011) Factors that predict bleeding following endoscopic mucosal resection of large colonic lesions. Endoscopy 43(6):506–511
Kim HH, Cho EJ, Park SJ et al (2012) Risk factors for incomplete resection and complications in endoscopic mucosal resection for lateral spreading tumors. Dig Endosc 24(4):259–266
Lim TR, Mahesh V, Singh S et al (2010) Endoscopic mucosal resection of colorectal polyps in typical UK hospitals. World J Gastroenterol 16(42):5323–5328
Ferrara F, Luigiano C, Ghersi S et al (2010) Efficacy, safety and outcomes of “Inject and Cut” endoscopic mucosal resection for large sessile and flat colorectal polyps. Digestion 82:313–320
Araghizadef FY, Timmcke AE, Opelka FG et al (2001) Colonoscopic perforations. Dis Colon Rectum 44(5):713–716
Bergmann U, Beger HG (2003) Endoscopic mucosal resection for advanced non-polypoid colorectal adenoma and early stage carcinoma. Surg Endosc 17:475–479
Zlantanic J, Way JD, Kim PS et al (1999) Large sessile colonic adenomas: use of argon plasma coagulator to supplement piecemeal snare polypectomy. Gastrointest Endosc 49:731–735
Doniec JM, Lohnert MS, Schniewind B et al (2003) Endoscopic removal of large colorectal polyps: prevention of unnecessary surgery? Dis Colon Rectum 2003(46):340–348
Kunihiro M, Tanaka S, Haruma K et al (2000) Electrocautery snare resection stimulates cellular proliferation of residual colorectal tumor: an increasing gene expression related to tumor growth. Dis Colon Rectum 43:1107–1115
Hotta K, Fujii T, Saito Y et al (2009) Local recurrence after endoscopic resection of colorectal tumors. Int J Colorectal Dis 24:225–230
Nakajima T, Saito Y, Tanaka S et al (2013) Current status of endoscopic resection strategy for large, early colorectal neoplasia in Japan. Surg Endosc 27(9):3262–3270
Kudo SE, Rubio CA, Teixeira CR et al (2001) Pit pattern in colorectal neoplasia: endoscopic magnifying view. Endoscopy 33(4):367–373
Acknowledgments
This study was carried out within the framework of a project undertaken by the Colorectal Endoscopic Resection Standardization Implementation Working Group supported by JSCCR Grants.
Facilities that participated the study
The patients were enrolled at the 18 institutions affiliated with the Colorectal Endoscopic Resection Standardization Implementation Working Group of JSCCR as follows, 1) Digestive Disease Center, Showa University Northern Yokohama Hospital, Kanagawa, Japan (Yoshiki Wada, Shin-ei Kudo, Hiroshi Kashida), 2) Department of Endoscopy, Hiroshima University Hospital, Hiroshima, Japan (Shinji Tanaka), 3) Endoscopy Division, National Cancer Center Hospital, Tokyo, Japan (Yutaka Saito), 4) Department of Gastrointestinal Oncology, Osaka Medical Center for Cancer and Cardiovascular Diseases, Osaka, Japan (Hiroyasu Iishi), 5) Department of Gastroenterology & Gastrointestinal Oncology, National Cancer Center Hospital East, Chiba, Japan (Hiroaki Ikematsu), 6) Department of Endoscopy, Cancer Institute Ariake Hospital, Tokyo, Japan (Masahiro Igarashi), 7) Digestive disease center, Asahikawa City Hospital, Hokkaido, Japan (Yuusuke Saitoh), 8) Institute of Gastroenterology, Tokyo Women’s Medical University, Tokyo, Japan (Yuji Inoue), 9) Department of Gastroenterology, Kitasato University East Hospital, Kanagawa, Japan (Kiyonori Kobayashi), 10) Department of Gastroenterology, Fukuoka University Chikushi Hospital, Fukuoka, Japan (Takashi Hisasbe), 11) Division of Gastroenterology, Department of Medicine, Kurume University School of Medicine, Fukuoka, Japan (Osamu Tsuruta), 12) Gastrointestinal Center, Sano Hospital, Hyogo, Japan (Yasushi Sano), 13) Department of Gastroenterology, Akita Red Cross Hospital, Akita, Japan (Hiro-o Yamano), 14) Department of Gastroenterology, JR West Osaka Railway Hospital, Osaka, Japan (Seiji Shimizu), 15) Department of Gastroenterology, Toranomon Hospital, Tokyo, Japan (Naohisa Yahagi), 16) Department of Surgery, Teikyo University Hospital, Tokyo, Japan (Toshiaki Watanabe), 17) Department of Gastroenterology, Chofu Surgical Clinic, Tokyo, Japan (Hisashi Nakamura),18) Gastroenterology, Takahiro Fujii Clinic, Tokyo, Japan (Takahiro Fujii)
Disclosures
Yoshiki Wada, Shin-ei Kudo, Shinji Tanaka, Yutaka Saito, Hiroyasu Iishii, Hiroaki Ikematsu, Masahiro Igarashi, Yusuke Saitoh, Yuji Inoue, Kiyonori Kobayashi, Takashi Hisabe, Osamu Tsuruta, Hiroshi Kashida, Hideki Ishikawa and, Kenichi Sugihara have no conflicts of interests or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Wada, Y., Kudo, Se., Tanaka, S. et al. Predictive factors for complications in endoscopic resection of large colorectal lesions: a multicenter prospective study. Surg Endosc 29, 1216–1222 (2015). https://doi.org/10.1007/s00464-014-3799-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-014-3799-9