
Abstract
Introduction
Since receiving Food and Drug Administration approval in 2000, surgery utilizing a robot has been successfully performed in numerous procedures including gastric bypass. However, despite the proven safety profile, reported lower complication rates, and technical benefits of robotic surgery, only a few centers in the USA have consistently applied this technology to bariatric surgery. In addition, there are limited studies with relatively small sample sizes comparing robotic-assisted Roux-en-Y gastric bypass (RRYGB) with laparoscopic Roux-en-Y gastric bypass (LRYGB).
Methods
Through a retrospective analysis of our database, we compared outcomes of RRYGB versus LRYGB in the treatment of morbid obesity. All patients who underwent RRYGB and LRYGB through the Comprehensive Weight Management Program of the Queen’s Medical Center (Honolulu, HI) from January 2007 to December 2009 were included. Outcomes data included weight loss, operative times, and hospital length of stay. All complications were reported.
Results
105 patients who underwent RRYGB were compared with 195 patients who received LRYGB. Excess weight loss, estimated blood loss, and length of hospital stay were similar in both groups. There were no mortalities in either group. The RRYGB group experienced a 9.5% complication rate versus 9.7% in LRYGB patients. Operative time was the only statistically significant difference, being approximately 17 min in favor of LRYGB. However, there was a steady decrease in RRYGB operative time with increasing experience.
Conclusion
Our study demonstrates a favorable safety profile with nearly equivalent outcomes and some previously unidentified qualitative benefits of the RRYGB approach to bariatric surgery in a community setting. These results are despite our early experience with the robotic surgery platform and confirm noninferiority of RRYGB versus LRYGB. While the RRYGB operative time was longer than LRYGB, the demonstrated decrease in operative time commensurate with increase in operative experience holds tremendous promise for the future.
Similar content being viewed by others


Obesity rates have increased dramatically in the USA over the last 25 years. As of 2008, overall prevalence of obesity as defined by body mass index (BMI) greater than 30 kg/m2 was 33.8% [1]. Obesity adversely affects the lives of millions of Americans by increasing the risk for comorbid conditions such as diabetes mellitus, obstructive sleep apnea, hypertension, and even certain cancers [2, 3]. Laparoscopic Roux-en-Y gastric bypass (LRYGB) is a safe, effective, and durable treatment option for refractory morbid obesity and its related health consequences [4]. Moreover, this minimally invasive approach offers obvious advantages such as decreased recovery time, less postoperative pain, and favorable complication rates as compared with open approaches [4–6].
The advent of robotic-assisted techniques using the da Vinci™ surgical system now offers the possibility of improved accuracy and enhanced precision with its three-dimensional visualization, wristed instrumentation, tremor control, and improved ergonomics. Since receiving Food and Drug Administration approval in 2000, robot-assisted surgery has been utilized in a variety of general surgical procedures, urologic surgery, and gynecologic procedures [7–10]. Over 200 medical centers in the USA currently own and use a da Vinci™ surgical system robot [10]. Only a few, however, have applied this technology to bariatric surgery [11–16]. Although robotic-assisted Roux-en-Y gastric bypass (RRYGB) has been shown to be safe, few studies have clearly demonstrated significant benefit over the laparoscopic approach [11–16]. Moreover, the high initial capital investment, along with the additional costs of required maintenance, and the technologically complex nature of robotic surgery have been formidable barriers to widespread acceptance of this new technology [11, 12, 15].
Since February 2007, three surgeons at the Queen’s Medical Center (Honolulu, HI) Comprehensive Weight Management Program have performed over 105 RRYGB surgeries. The Queen’s Medical Center is a 560-bed, community hospital. We present our data regarding patient outcomes, comparing the robotic-assisted approach with LRYGB. Perioperative complications, operative times, surgical blood loss, and associated hospital costs were specifically examined. This study represents consistent use of the da Vinci™ surgical system for bariatric surgery in a community hospital setting.
Methods
We retrospectively reviewed our database, including all patients undergoing bariatric surgery at our center between January 2007 and December 2009. All patients undergoing LRYGB and RRYGB surgery for morbid obesity were included. Preoperative data included baseline BMI, American Society of Anesthesiology (ASA) score, age, gender, ethnicity, and presence of obesity-related comorbid diseases. Each patient record was evaluated for operative time, intraoperative blood loss, and surgical complications. Postoperative data studied included total hospital length of stay, percentage excess body weight loss (% EWL) at 1 year, and surgery-related complications.
We used SPSS® (version 16.0) statistical data analysis software to compare LRYGB versus RRYGB for significant differences. A p-value of <0.05 was deemed statistically significant for our study. Continuous variables were analyzed by independent T-test, and noncontinuous data were evaluated by chi-square analysis. Outcomes data comparisons included excess body weight loss at 1 year, evaluation of surgery-related complications, and an analysis of total hospital cost between the two groups.
Results
In total, 301 patients underwent bariatric surgery during the study period (195 LRYGB, 106 RRYGB). Two patients in the LRYGB group underwent additional procedures (resection of ovarian cysts) during the same anesthetic event, and three LRYGB patients were converted to open laparotomy (twice for positive intraoperative leak test and inability to control via laparoscopic methods; once due to extensive adhesions and inability to create a tension-free gastrojejunostomy via standard laparoscopic approach). There was one conversion from RRYGB to LRYGB, but no conversions to open laparotomy were necessary. These patients were all included in outcomes data analysis, but excluded from operative time analysis. One patient in the RRYGB group requested exclusion from the study, resulting in final study groups of 195 LRYGB and 105 RRYGB patients.
In the RRYGB group, there were 83 females (79.1%), and mean age was 42.2 years [standard deviation (SD) 10.95 years, range 21–64 years), preoperative BMI was 46.77 kg/m2 (SD 8.35 kg/m2, range 33.5–75.5 kg/m2), and nearly half (49.2%) were ethnically identified as Pacific Islander. In the LRGYB group, there were 141 females (72.3%), and mean age was 43.9 years (SD 10.86 years, range 20–64 years), preoperative BMI was 47.67 kg/m2 (SD 9.42 kg/m2, range 34.8–87.2 kg/m2), and over a third (34.4%) were of Pacific Islander descent. Comorbid disease profiles were similar in both groups. Of the LRYGB patients, 34.9% had diabetes, 64.1% had hypertension, 64.6% had obstructive sleep apnea, 38.5% had gastroesophageal reflux disease, 51.8% had dyslipidemia, and 32.3% had asthma. Of the RRYGB patients, 36.2% had diabetes, 57.1% had hypertension, 54.3% had obstructive sleep apnea, 41.9% had gastroesophageal reflux disease, 52.4% had dyslipidemia, and 35.2% had asthma. There were no statistically significant differences across LRYGB and RRYGB groups for preoperative data (Table 1).
Mean operative time was the only statistically significant difference (p = 0.003) between LRYGB and RRYGB. Operative times were 169 min (SD 38 min, range 94–298 min) in the RRYGB group versus 152 min (SD 50 min, range 56–319 min) in the LRYGB group. Mean intraoperative blood loss was 58.98 ml (SD 43.8 ml) for RRYGB patients and 57.2 ml (SD 45.9 ml) for LRYGB patients. Hospital length of stay was similar: 3.41 days (SD 7.03 days, range 1–74 days) for RRYGB and 2.95 days (SD 2.75 days, range 1–36 days) for LRYGB patients. Complication rates were nearly identical (9.74% for LRYGB, 9.52% for RRYGB), and ranged in severity from wound infections, postoperative trocar-site bleeding, marginal ulcers, delayed gastrojejunal anastomotic strictures, and anastomotic leaks. Of the LRYGB patients, 66.2% had available follow-up data at 1 year versus 61.9% in the RRYGB group. There were no statistically significant differences in % EWL (61.3% LRYGB versus 61.9% RRYGB), surgery-related complication rates, or total hospital costs between the LRYGB and RRYGB groups (Tables 2, 3).
Discussion
Reports on RRYGB performed in a community hospital setting are sparse. Previously reported studies have been published from large, academic institutions, and the applicability of robotic technology in a community bariatric setting has not been previously established.
Efficacy
The American Society for Metabolic and Bariatric Surgery estimated that over 220,000 bariatric procedures were performed in the USA in 2008, and LRYGB is the most commonly performed bariatric surgical procedure today [5, 17]. Our center’s experience mirrors this national trend, as a majority of our patients undergo LRYGB. With the addition of robotic surgery capabilities at our center in 2007, we have utilized the robot to assist with the most technically challenging portions of the Roux-en-Y gastric bypass, namely creation of gastrojejunostomy. Our outcomes data reflecting % EWL, hospital length of stay, and complication rates all demonstrate equivalent efficacy in surgical weight loss for both methods.
Complications
Detailed information on complications for both RRYGB and LRYGB is presented in Tables 4 and 5 respectively. As evidenced by the nearly identical overall complication rates, our data confirm the safety profile of RRYGB when compared with LRYGB. Complications were varied and ranged in severity from episodes of dehydration and wound infections managed on an outpatient basis, to trocar-site bleeding requiring blood transfusions and anastomotic strictures managed with endoscopic dilation(s), to more severe complications such as bowel obstructions, anastomotic leaks, and postoperative hemorrhage requiring reoperation and intensive care (Table 6).
While most complications did not result in significant morbidity, there were isolated cases of patients requiring reoperation and an extended hospital stay. The longest length of stay (74 days) was recorded in the RRYGB group, in a patient who developed a postoperative gastrojejunal anastomotic leak, requiring open reoperation and repeated abdominal washouts. Likewise, in the LRGYB group, an anastomotic leak resulted in readmission and prolonged length of stay (70 days).
Although statistically not significant, RRYGB patients experienced fewer gastrojejunal anastomotic leaks, but more gastrojejunal anastomotic strictures than LRYGB patients. The benefits of robotic assistance such as enhanced stereoscopic image viewing and better surgical precision and instrument mobility may be contributing factors, but our study was likely underpowered to validate such differences.
In a preliminary review, we did identify this increased stricture rate among RRYGB patients, and modifications in our robotic surgical techniques were made during the study period in the hope of improving our surgical outcomes. We identified several factors that may have contributed to this early observation. Prior to August 2008, robotic-assisted construction of the gastrojejunal anastomosis was completed in a two-layered fashion with a running absorbable suture for full-thickness mucosal apposition and an outer, running seromuscular layer using a continuous Ethibond® suture. This continuous suture technique may have contributed to tissue ischemia and resulting stricture formation due to a purse-string effect at the anastomosis.
Additionally, the lack of haptic feedback with use of the robot may have also contributed to inadvertent rough handling of tissues and aggressive pull on suture material when creating an anastomosis with a running length of suture. Finally, the advantages of robotic surgery may have actually had a detrimental effect. Although the stereoscopic visualization is overall a tremendous benefit, the magnified view may have led to unnecessary placement of suture throws in closer proximity to each other, and this may have contributed to greater tissue ischemia and stricture formation.
After August 1, 2008, procedural modifications were made with the aim of decreasing tissue trauma, ischemia, and the possible end result of increased stricture formation. To address the issue of the purse-string effect, conversion was made to an interrupted, full-thickness, single-layered gastrojejunal anastomosis using absorbable Vicryl® suture with attention paid to achieving mucosal apposition. Additionally, after completion of the posterior half of the anastomosis, we now position a gastroscope with outer diameter of 8.8 mm beyond the newly created posterior aspect of the anastomosis and hold it in this position while the anterior half of the anastomosis is completed. This allows for appropriate sizing of the anastomotic diameter to be 10–12 mm when completed and ensures luminal patency of the completed gastrojejunal anastomosis. Following these modifications, no further events of anastomotic stricture after RRYGB were noted.
Conversions
No conversions from RRYGB to open surgery were required. However, one RRYGB conversion to LRYGB was required due to inability to dock the robot properly in a super-morbidly obese patient. This patient had a particularly large abdominal girth that prevented mobility of the robotic arms and proper reach with the camera arm. We were able to successfully complete the RYGB laparoscopically after conversion to standard laparoscopic methods. In contrast, three LRYGB cases were converted to open RYGB. In two instances, gastrojejunal anastomotic leaks were identified intraoperatively using insufflation via transoral placement of a gastroscope and air pressure testing of the newly created gastrojejunal anastomosis submerged under irrigation fluid. In both instances, leaks were evident at sites of bubbling at the anastomotic suture line, but were not able to be controlled laparoscopically. Thus, open conversion was required. In the third case of conversion from LRYGB to an open approach, the patient’s extensive intra-abdominal adhesions and foreshortened mesentery prevented mobilization of an adequate length of jejunum to complete a tension-free anastomosis with the newly created gastric pouch. Open conversion was necessary to safely perform the extensive adhesiolysis, mobilize the distal esophagus at the diaphragmatic hiatus to bring the gastric pouch to a more caudal position, and create windows in the jejunal Roux limb’s mesentery. Only after all of these maneuvers were we able to achieve creation of a tension-free anastomosis.
Operative time
Although the technical benefits of robotic surgery such as three-dimensional image viewing with improved optics, enhanced surgical dexterity, and better ergonomics have impressed many surgeons, these advancements have not translated into widespread adoption of this new technology for bariatric surgical procedures. One of the criticisms against robotic surgery is an increase in operative time. However, studies have shown that RRYGB may actually be easier to teach and learn. Centers reporting regular utilization of robotic-assisted procedures, including its use in bariatric surgery, have noted that ascendency of the robotic learning curve is quite favorable when compared with that of standard laparoscopic surgery [16, 18]. As a result, achievement of shorter operative times may be possible much sooner when using the robot [10–12].
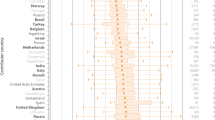
Our operative times did demonstrate a steady decrease over time (Fig. 1). The only statistically significant difference in our data, however, was this difference in operative times between RRYGB and LRYGB, with a trend toward increased operative times required for RRYGB. We attribute this additional time of approximately 17 min to the following: time required to properly dock the operating unit and adjust the surgeon’s console, time needed to create the anastomosis (versus stapled in LRYGB), and time required for endoscope placement during creation of anastomosis.

Operative times (min)
Cost
Another factor limiting widespread adoption of robot-assisted procedures in general and bariatric surgery is the associated cost. While the substantial initial investment for robotic equipment can be prohibitive, a case-by-case difference in cost was not identified in our study. Due to proprietary reasons, we are unable to publish data on specific dollar amount differences between RRYGB versus LRYGB procedures. However, an internal analysis of total hospital charges between RRYGB versus LRYGB billed for the surgical admission demonstrated that both groups had similar total hospital charges. Likewise, hospital length of stay between RRYGB and LRYGB was similar.
Surgical education
A significant advantage with utilization of robotic-assisted bariatric procedures in our center is the increased exposure that assisting surgical residents have to this emerging technology. No other study has previously reported on this finding. Our center is affiliated with the University of Hawaii, John A. Burns School of Medicine, a community-based surgical residency program. Use of the robot in general surgery remains limited, and prior to the initiation of the RRYGB operation, no surgical resident exposure was available. Since 2007, we have trained chief surgical residents to be qualified assistants in robotic surgery (curriculum available through da Vinci™ surgical systems).
The certification process begins with an online training module and an online knowledge assessment test. This is followed by a 2–3-h hands-on training session performed in a dry-lab setting where the resident is trained to set up the robot, install and replace various surgical instruments, and troubleshoot common problems and equipment errors. The next level of training provides the resident with ample opportunity for direct hands-on experience utilizing the robot in manual dexterity drills, suturing, and other robotic operating tasks, again in a dry-lab setting. Throughout this training program, the resident’s progress is tracked by a supervising robotic surgeon and the surgical residency program director.
After satisfactory completion of each of these levels of training, the resident is allowed to assist in a RRYGB procedure along with the supervising robotic surgeon. The qualification to assist independently is granted only after the resident has been proctored by an experienced robotic surgeon over several cases. Finally, after demonstration of familiarity with all previous levels of training, the surgical resident is then able to progress onto operating at the surgical robotic console with close supervision.
Conclusions
Our study demonstrates a favorable safety profile with nearly equivalent outcomes and some previously unidentified qualitative benefits of the RRYGB approach to bariatric surgery in a community setting. These results are despite our early inexperience and confirm noninferiority of RRYGB to LRYGB. The demonstrated decrease in operative time commensurate with increase in operative experience holds tremendous promise for the future. As such, our center is currently in preparation for a prospective randomized trial to further evaluate these outcomes.
References
Flegal KM, Carroll MD, Ogden CL, Curtin LR (2010) Prevalence and trends in obesity among US adults, 1999–2008. J Am Med Assoc 303(3):235–241
Buchwald H, Avidor Y, Braunwald E, Jensen MD, Pories W, Fahrbach K, Schoelles K (2004) Bariatric surgery: a systematic review and meta-analysis. JAMA 292:1724–1737
Sjöström L, Narbro K, Sjöström CD, Karason K, Larsson B, Wedel H, Lystig T, Sullivan M, Bouchard C, Carlsson B, Bengtsson C, Dahlgren S, Gummesson A, Jacobson P, Karlsson J, Lindroos AK, Lonroth H, Naslund I, Olbers T, Stenlof K, Torgerson J, Agren G, Carlsson LM (2007) The effects of obesity on mortality in Swedish obese subjects. N Engl J Med 357(8):741–752
Pories WJ (2008) Bariatric surgery: risks and rewards. J Clin Endocrinol Metab 93(11):S89–S96
The Longitudinal Assessment of Bariatric Surgery (LABS) Consortium (2009) Perioperative safety in the longitudinal assessment of bariatric surgery. N Engl J Med 361:445–454
Weller WE, Rosati C (2008) Comparing outcomes of laparoscopic versus open bariatric surgery. Ann Surg 248(1):10–15
Talamini MA, Chapman S, Horgan S, Melvin WS (2003) A prospective analysis of 211 robotic-assisted surgical procedures. Surg Endosc 17:1521–1524
Badani KK, Kaul S, Menon M (2007) Evolution of robotic radical prostatectomy: assessment after 2766 procedures. Cancer 110(9):1951–1958
Payne TN, Dauterive FR (2008) A comparison of total laparoscopic hysterectomy to robotically assisted hysterectomy: surgical outcomes in a community practice. J Minim Invasive Gynecol 15(3):286–291
da Vinci Surgery. Overview of surgical procedures, including gastric bypass surgery. Available at: http://www.davincisurgery.com/procedures/index.aspx. Accessed 14 April 2010
Ali MR, Bhasker-Rao B, Wolfe BM (2005) Robot-assisted laparoscopic roux-en-y gastric bypass. Surg Endosc 19:468–472
Parini U, Fabozzi M, Contul RB, Millo P, Loffredo A, Allieta R, Nardi M Jr, Lale-Murix E (2006) Laparoscopic gastric bypass performed with the da vinci intuitive robotic system: preliminary experience. Surg Endosc 20:1851–1857
Mohr CJ, Nadzam GS, Curet M (2005) Totally robotic roux-en-y gastric bypass. Arch Surg 140:779–786
Mohr CJ, Nadzam GS, Alami RS, Sanchez BR, Curet MJ (2006) Totally robotic laparoscopic roux-en-y gastric bypass: Results from 75 patients. Obes Surg 16:690–696
Hubens G, Balliu L, Ruppert M, Gypen B, Van Tu T, Vaneerdeweg W (2008) Roux-en-y gastric bypass procedure performed with the da vinci robot system: is it worth it? Surg Endosc 22:1690–1696
Yu SC, Clapp BL, Lee MJ, Albrecht WC, Scarborough TK, Wilson EB (2006) Robotic assistance provides excellent outcomes during the learning curve for laparoscopic roux-en-y gastric bypass: results from 100 robotic assisted gastric bypasses. Am J Surg 192:746–749
American Society for Metabolic and Bariatric Surgery. Fact Sheet on Metabolic and Bariatric Surgery. Available at: http://www.asbs.org/Newsite07/media/asmbs_fs_surgery.pdf. Accessed 14 April 2010
Ali MR, Rasmussen J, Bhasker-Rao B (2007) Teaching robotic surgery: a stepwise approach. Surg Endosc 21:912–915
Disclosures
Authors Chan W. Park, Edward CF Lam, Teresa M. Walsh, Maxine Karimoto, MD, Adrienne T. Ma, Matt Koo, Chet Hammill, Cedric S. F. Lorenzo, and Racquel Bueno have no conflicts of interest or financial ties to disclose. Author Kenric Murayama is a speaker/proctor for Covidien and has received honoraria from them.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Park, C.W., Lam, E.C.F., Walsh, T.M. et al. Robotic-assisted Roux-en-Y gastric bypass performed in a community hospital setting: the future of bariatric surgery?. Surg Endosc 25, 3312–3321 (2011). https://doi.org/10.1007/s00464-011-1714-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-011-1714-1