
Abstract
Background
Fast-track (FT) recovery protocols have demonstrated advantages over historical recovery routines after open colectomy; however, their impact in recovery after laparoscopic colectomy is not clearly defined. This study was designed to determine whether patients who recover on FT protocol after laparoscopic colectomy have a shorter length of stay (LOS) and fewer complications compared with patients who recover on standard (non-FT) protocol.
Methods
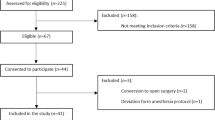
A cohort of consecutive patients with colon cancer who underwent completed laparoscopic-assisted right hemicolectomy from 2005–2007 was identified. Univariate and multivariate logistic analyses were performed to identify risk factors for increased LOS and postoperative complications with recovery protocol as the primary predictor.
Results
A total of 197 patients were included: 115 (58%) patients recovered on a non-FT protocol, and 82 (42%) patients on FT protocol. Univariate analysis showed no differences with respect to age, gender, body mass index, or American Society of Anesthesiologists (ASA) class between groups. The median (interquartile range) LOS was 4 (range, 3–6) days and 3 (range, 3–4) days for the non-FT and FT recovery patients, respectively (p < 0.001). On multivariate analysis, independent risk factors for increased LOS were complications (p < 0.001) and non-FT recovery (p = 0.007). Non-FT recovery also was associated with increased complications (56 vs. 29%, p = 0.0002); this remained significant on multivariate analysis (p < 0.001). Readmissions were similar (p = 1.0) between recovery groups. No mortalities were observed at 30 days.
Conclusions
Fast-track recovery is independently associated with a shorter LOS and decreased morbidity after laparoscopic right hemicolectomy.
Similar content being viewed by others


References
Kehlet H, Wilmore DW (2002) Multimodal strategies to improve surgical outcome. Am J Surg 183:630–641
Basse L, Thorbol JE, Lossl K, Kehlet H (2004) Colonic surgery with accelerated rehabilitation or conventional care. Dis Colon Rectum 47:271–277 (discussion 277-278)
Andersen HK, Lewis SJ, Thomas S (2008) Early enteral nutrition within 24 h of colorectal surgery versus later commencement of feeding for postoperative complications [review]. The Cochrane Library 2008, Issue 2:1–25
Wind J, Polle SW, Fung Kon Jin PH, Dejong CH, von Meyenfeldt MF, Ubbink DT, Gouma DJ, Bemelman WA (2006) Systematic review of enhanced recovery programmes in colonic surgery. Br J Surg 93:800–809
Weeks JC, Nelson H, Gelber S, Sargent D, Schroeder G (2002) Short-term quality-of-life outcomes following laparoscopic-assisted colectomy vs open colectomy for colon cancer: a randomized trial. JAMA 287:321–328
Noel JK, Fahrbach K, Estok R, Cella C, Frame D, Linz H, Cima RR, Dozois EJ, Senagore AJ (2007) Minimally invasive colorectal resection outcomes: short-term comparison with open procedures. J Am Coll Surg 204:291–307
Vermeulen H, Storm-Versloot MN, Busch OR, Ubbink DT (2006) Nasogastric intubation after abdominal surgery: a meta-analysis of recent literature. Arch Surg 141:307–314
Bucher P, Mermillod B, Gervaz P, Morel P (2004) Mechanical bowel preparation for elective colorectal surgery: a meta-analysis. Arch Surg 139:1359–1364 (discussion 1365)
Basse L, Hjort Jakobsen D, Billesbolle P, Werner M, Kehlet H (2000) A clinical pathway to accelerate recovery after colonic resection. Ann Surg 232:51–57
Basse L, Jakobsen DH, Bardram L, Billesbolle P, Lund C, Mogensen T, Rosenberg J, Kehlet H (2005) Functional recovery after open versus laparoscopic colonic resection: a randomized, blinded study. Ann Surg 241:416–423
Senagore AJ, Duepree HJ, Delaney CP, Brady KM, Fazio VW (2003) Results of a standardized technique and postoperative care plan for laparoscopic sigmoid colectomy: a 30-month experience. Dis Colon Rectum 46:503–509
Raue W, Haase O, Junghans T, Scharfenberg M, Muller JM, Schwenk W (2004) ‘Fast-track’ multimodal rehabilitation program improves outcome after laparoscopic sigmoidectomy: a controlled prospective evaluation. Surg Endosc 18:1463–1468
Disclosures
Drs. Tsikitis, Holubar, Dozois, Cima, Pemberton, and Larson have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tsikitis, V.L., Holubar, S.D., Dozois, E.J. et al. Advantages of fast-track recovery after laparoscopic right hemicolectomy for colon cancer. Surg Endosc 24, 1911–1916 (2010). https://doi.org/10.1007/s00464-009-0871-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-009-0871-y