
Abstract
Background
For a small subset of patients, laparoscopic fundoplication fails, typically resulting in recurrent reflux or severe dysphagia. Although redo fundoplications can be performed laparoscopically, few studies have examined their long-term efficacy.
Methods
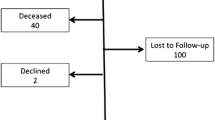
Using a prospectively maintained database, the authors identified and contacted 41 patients who had undergone redo laparoscopic fundoplications at the University of Washington between 1996 and 2001. The median follow-up period was 50 months (range, 20–95 months). Current symptoms were compared with those acquired and entered into the authors’ database preoperatively. Patients also were asked to return for esophageal manometry and pH testing.
Results
All redo fundoplications were performed laparoscopically. There were no conversions. The most common indication for redo fundoplication was recurrent reflux. The most common anatomic abnormality was a herniated wrap. Heartburn improved in 61%, regurgitation in 69%, and dysphagia in 74% of the patients. Complete resolution of these symptoms was achieved, respectively, in 45%, 41% and 38% of these same patients. Overall, 68% of the patients rated the success of the procedure as either “excellent” or “good,” and 78% said they were happy they chose to have it. For those who underwent reoperation for gastroesophageal reflux disease, distal esophageal acid exposure according to 24-h pH monitoring decreased after redo fundoplication from 15.7% ± 18.1% to 3.4% ± 3.6% (p = 0.041).
Conclusion
Although not as successful as primary fundoplication, a majority of patients can expect durable improvement in their symptoms with a laparoscopic redo fundoplication.




Similar content being viewed by others

References
Ackroyd R, Watson DI, Majeed AW, Troy G, Treacy PJ, Stoddard CJ (2004) Randomized clinical trial of laparoscopic versus open fundoplication for gastro-oesophageal reflux disease. Br J Surg 91: 975–982
Chrysos E, Tsiaoussis J, Athanasakis E, Zoras O, Vassilakis JS, Xynos E (2002) Laparoscopic vs open approach for Nissen fundoplication: a comparative study. Surg Endosc 16: 1679–1684
Coelho JC, Goncalves CG, Claus CM, Andrigueto PC, Ribeiro MN (2004) Late laparoscopic reoperation of failed antireflux procedures. Surg Laparosc Endosc Percutan Tech 14: 113–117
Dallemagne B, Weerts JM, Jehaes C, Markiewicz S, Lombard R (1991) Laparoscopic Nissen fundoplication: preliminary report. Surg Laparosc Endosc 1: 138–143
Dassinger MS, Torquati A, Houston HL, Holzman MD, Sharp KW, Richards WO (2004) Laparoscopic fundoplication: 5-year follow-up. Am Surg 70: 691–694; discussion 694–695
Deschamps C, Trastek VF, Allen MS, Pairolero PC, Johnson JO, Larson DR (1997) Long-term results after reoperation for failed antireflux procedures. J Thorac Cardiovasc Surg 113: 545–550; discussion 550–541
Dutta S, Bamehriz F, Boghossian T, Pottruff CG, Anvari M (2004) Outcome of laparoscopic redo fundoplication. Surg Endosc 18: 440–443
Eubanks TR, Omelanczuk P, Richards C, Pohl D, Pellegrini CA (2000) Outcomes of laparoscopic antireflux procedures. Am J Surg 179: 391–395
Granderath FA, Kamolz T, Schweiger UM, Pointner R (2002) Long-term follow-up after laparoscopic refundoplication for failed antireflux surgery: quality of life, symptomatic outcome, and patient satisfaction. J Gastrointest Surg 6: 812–818
Hashemi M, Peters JH, DeMeester TR, Huprich JE, Quek M, Hagen JA, Crookes PE, Theisen J, DeMeester SR, Sillin LF, Bremner CG (2000) Laparoscopic repair of large type III hiatal hernia: objective follow-up reveals high recurrence rate. J Am Coll Surg 190: 553–560; discussion 560–551
Heudebert GR, Marks R, Wilcox CM, Centor RM (1997) Choice of long-term strategy for the management of patients with severe esophagitis: a cost-utility analysis. Gastroenterology 112: 1078–1086
Hinder RA, Filipi CJ, Wetscher G, Neary P, DeMeester TR, Perdikis G (1994) Laparoscopic Nissen fundoplication is an effective treatment for gastroesophageal reflux disease. Ann Surg 220: 472–481; discussion 481–473
Horgan S, Pohl D, Bogetti D, Eubanks T, Pellegrini C (1999) Failed antireflux surgery: what have we learned from reoperations? Arch Surg 134: 809–815; discussion 815–807
Hunter JG, Smith CD, Branum GD, Waring JP, Trus TL, Cornwell M, Galloway K (1999) Laparoscopic fundoplication failures: patterns of failure and response to fundoplication revision. Ann Surg 230: 595–604; discussion 604–596
Jenkinson AD, Kadirkamanathan SS, Scott SM, Yazaki E, Evans DF (2004) Relationship between symptom response and oesophageal acid exposure after medical and surgical treatment for gastro-oesophageal reflux disease. Br J Surg 91: 1460–1465
Khajanchee YS, O’Rourke RW, Lockhart B, Patterson EJ, Hansen PD, Swanstrom LL (2002) Postoperative symptoms and failure after antireflux surgery. Arch Surg 137: 1008–1013; discussion 1013–1004
Locke GR III, Talley NJ, Fett SL, Zinsmeister AR, Melton LJ III (1997) Prevalence and clinical spectrum of gastroesophageal reflux: a population-based study in Olmsted County, Minnesota. Gastroenterology 112: 1448–1456
Lord RV, Kaminski A, Oberg S, Bowery DJ, Hagen JA, DeMeester SR, Sillin LE, Peters JH, Crookes PF, DeMeester TR (2002) Absence of gastroesophageal reflux disease in a majority of patients taking acid suppression medications after Nissen fundoplication. J Gastrointest Surg 6: 3–9; discussion 10
Lundell L, Miettinen P, Myrvold HE, Pedersen SA, Liedman B, Hatlebakk JG, Julkonen R, Levander K, Carlsson J, Lamm M, Wiklund I (2001) Continued (5-year) follow-up of a randomized clinical study comparing antireflux surgery and omeprazole in gastroesophageal reflux disease. J Am Coll Surg 192: 172–179; discussion 179–181
Nebel OT, Fornes MF, Castell DO (1976) Symptomatic gastroesophageal reflux: incidence and precipitating factors. Am J Dig Dis 21: 953–956
Nessen SC, Holcomb J, Tonkinson B, Hetz SP, Schreiber MA (1999) Early laparoscopic Nissen fundoplication for recurrent reflux esophagitis: a cost-effective alternative to omeprazole. JSLS 3: 103–106
Neuhauser B, Hinder RA (2001) Laparoscopic reoperation after failed antireflux surgery. Semin Laparosc Surg 8: 281–286
Nilsson G, Larsson S, Johnsson F (2000) Randomized clinical trial of laparoscopic versus open fundoplication: blind evaluation of recovery and discharge period. Br J Surg 87: 873–878
Oelschlager BK, Pellegrini CA (2001) Minimally invasive surgery for gastroesophageal reflux disease. J Laparoendosc Adv Surg Tech A 11: 341–349
Romagnuolo J, Meier MA, Sadowski DC (2002) Medical or surgical therapy for erosive reflux esophagitis: cost-utility analysis using a Markov model. Ann Surg 236: 191–202
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Oelschlager, B.K., Lal, D.R., Jensen, E. et al. Medium- and long-term outcome of laparoscopic redo fundoplication. Surg Endosc 20, 1817–1823 (2006). https://doi.org/10.1007/s00464-005-0262-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-005-0262-y