
Abstract
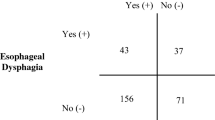
The purpose of this prospective, double-blinded, multirater, systematic replication study was to investigate agreement for aspiration risk, in the same individual, between videofluoroscopic swallow studies (VFSS) and the Yale Swallow Protocol. Participants were 25 consecutive adults referred for dysphagia testing who met the inclusion criteria of completion of a brief cognitive assessment, oral mechanism examination, and no tracheotomy tube. First, all participants were administered the Yale Swallow Protocol by two experienced speech-language pathologists trained in protocol administration. Failure criteria were inability to drink the entire amount, interrupted drinking, or coughing during or immediately after drinking. Second, all participants completed a VFSS within 5–10 min of protocol administration. A speech-language pathologist, blinded to protocol results, reviewed the VFSS to determine aspiration status in a binary (yes/no) manner. Inter-rater agreement between two speech-language pathologists was 100 % for identification of aspiration risk with the Yale Swallow Protocol. Inter-rater agreement between the speech-language pathologist and the radiologist for identification of aspiration status with VFSS was 100 %. Twenty percent of VFSS recordings were viewed again 3–6 months after initial data collection, and intrarater agreement for identification of thin liquid aspiration was 100 %. Sensitivity for the Yale Swallow Protocol = 100 %, specificity = 64 %, positive predictive value = 78 %, and negative predictive value = 100 %. Importantly, all participants who passed the protocol did not aspirate during VFSS. Multiple, double-blinded raters and VFSS as the reference standard agreed with previous research with a single, nonblinded rater and FEES as the reference standard for identification of aspiration risk. The clinical usefulness and validity of the Yale Swallow Protocol for determining aspiration risk in a small sample size of male participants has been confirmed. Future research is needed with a larger and more heterogeneous population sample.
Similar content being viewed by others

References
DePippo KL, Holas MA, Reding MJ. Validation of the 3-oz water swallow test for aspiration following stroke. Arch Neurol. 1992;49:1259–61.
Suiter DB, Leder SB. Clinical utility of the 3 ounce water swallow test. Dysphagia. 2008;23:244–50.
Leder SB, Suiter DM, Green BG. Silent aspiration risk is volume dependent. Dysphagia. 2011;26:304–9.
Warner HL, Suiter DM, Nystrom KV, Poskus, K, Leder SB. Comparing accuracy of the Yale Swallow Protocol when administered by registered nurses and speech-language pathologists. J Clin Nurs. doi:10.1111/jocn.12340.
Leder SB, Suiter DM, Lisitano HL. Answering orientation questions and following single step verbal commands: Effect on aspiration status. Dysphagia. 2009;24:290–5.
Leder SB, Suiter DM, Murray J, Rademaker AW. Can an oral mechanism examination contribute to the assessment of odds of aspiration? Dysphagia. 2013;28:370–4. doi:10.1007/s00455-012-9442-9.
Leder SB, Suiter DM, Warner HL, Kaplan LJ. Initiating safe oral feeding in critically ill intensive care and step-down unit patients based on passing a 3-ounce (90 milliliters) water swallow challenge. J Trauma. 2011;70:1203–7.
Leder SB, Suiter DM, Warner HL, Acton LM, Swainson BA. Success of recommending oral diets in acute stroke patients based on a 90-cc water swallow challenge protocol. Top Stroke Rehabil. 2012;19:40–4.
Leder SB, Suiter DM, Warner HL, Acton LM, Siegel MD. Safe initiation of oral diets in hospitalized patients based on passing a 3-ounce (90 cc) water swallow challenge protocol. QJM. 2012;105:257–63.
Leder SB, Judson JL, Sliwinski E, Madson L. Promoting safe swallowing when puree is swallowed without aspiration but thin liquid is aspirated: nectar is enough. Dysphagia. 2013;28(1):58–62.
Muma JR. The need for replication. J Speech Hear Res. 1993;36:927–30.
Logemann JA. Evaluation and treatment of swallowing disorders. 2nd ed. Austin: Pro-Ed; 1998.
Peterson SJ, Tsai AA, Scala CM. Adequacy of oral intake in critically ill patients 1 week after extubation. J Am Diet Assoc. 2010;110:427–33.
Ramsey DJC, Smithard DG, Kalra L. Early assessments of dysphagia and aspiration risk in acute stroke patients. Stroke. 2003;34:1252–7.
Heffner JE. Swallowing complications after endotracheal extubation. Chest. 2010;137:509–10.
Leder SB, Lerner MZ. Nil per os except medications order in the dysphagic patient. QJM. 2013;106:71–5.
Leder SB. Serial fiberoptic endoscopic swallowing examinations in the management of patients with dysphagia. Arch Phys Med Rehabil. 1998;79:1264–9.
Leder SB, Ross DA. Investigation of the causal relationship between tracheotomy and aspiration in the acute care setting. Laryngoscope. 2000;110:641–4.
Leder SB, Ross DA. Confirmation of no causal relationship between tracheotomy and aspiration status: a direct replication study. Dysphagia. 2010;5:35–9.
Leder SB. Incidence and type of aspiration in acute care patients requiring mechanical ventilation via a new tracheotomy. Chest. 2002;122:1721–6.
Link DT, Willging JP, Miller CK. Pediatric laryngopharyngeal sensory testing during flexible endoscopic evaluation of swallowing: feasible and correlative. Ann Otol Rhinol Laryngol. 2000;109:899–905.
Donzelli J, Brady S, Wesling M. Predictive value of accumulated oropharyngeal secretions for aspiration during video nasal endoscopic evaluation of swallowing. Ann Otol Rhinol Laryngol. 2003;112:469–75.
Conflict of interest
None of the authors have a conflict of interest to declare.
Author information
Authors and Affiliations
Corresponding author
Appendices
Appendix 1: Yale Swallow Protocol
Step 1: Exclusion Criteria
__ Yale Swallow Protocol Deferred due to NO concern for aspiration risk.
Any YES answer to the following risk factors will also defer administration of protocol:
Yes No
__ __ Unable to remain alert for testing
__ __ Eating a modified diet (thickened liquids) due to pre-existing dysphagia
__ __ Existing enteral tube feeding via stomach or nose
__ __ Head-of-bed restrictions < 30 °
__ __ Tracheotomy tube present
__ __ Nil per os by physician order
If the patient’s clinical status changes resulting in a new risk for aspiration, the protocol must be readministered before oral alimentation or medications are ordered.
Appendix 2: Yale Swallow Protocol
Step 2: Administration Instructions
If patient is deemed an aspiration risk and all exclusion criteria in Step 1 are checked “NO,” proceed with protocol:
-
Brief Cognitive Screen:
What is your name?
Where are you right now?
What year is it?
-
Oral-Mechanism Examination:
Labial closure
Lingual range of motion
Facial symmetry (smile/pucker)
-
Perform the 3-ounce water swallow challenge:
Sit patient upright at 80–90 ° (or as high as tolerated > 30 °).
Ask patient to drink the entire 3 ounces (90 cc) of water from a cup or with a straw, in sequential swallows, and slow and steady but without stopping. (Note: Cup or straw can be held by clinician or patient.) Assess patient for interrupted drinking and coughing or choking during or immediately after completion of drinking.
Note: Information from the brief cognitive screen [5] and oral mechanism examination [6] provide information on odds of aspiration risk with the 3-ounce water swallow challenge and should not be used as exclusionary criteria for screening.
Appendix 3: Yale Swallow Protocol
Step 3: Pass/Fail Criteria
Results and Recommendations
__ PASS: Complete and uninterrupted drinking of all 3 ounces of water without overt signs of aspiration, i.e., coughing or choking, either during or immediately after completion.
-
If patient passes, collaborate with MD/PA/LIP to order appropriate oral diet. If dentate, order a soft solid consistency or regular consistency diet. If edentulous, order a liquid and puree diet.
__ FAIL: Inability to drink the entire 3 ounces in sequential swallows due to stopping/starting or patient exhibits overt signs of aspiration, i.e., coughing or choking, either during or immediately after completion.
-
If patient fails, keep nil per os (including medications) and discuss with the MD/PA/LIP the need for an objective swallowing evaluation by speech-language pathologist.
-
Readminister the protocol in 24 h if patient shows clinical improvement.
Rights and permissions
About this article
Cite this article
Suiter, D.M., Sloggy, J. & Leder, S.B. Validation of the Yale Swallow Protocol: A Prospective Double-Blinded Videofluoroscopic Study. Dysphagia 29, 199–203 (2014). https://doi.org/10.1007/s00455-013-9488-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00455-013-9488-3