
Abstract
Vulnerability markers for affective disorders have focused on stress hormone regulation and sleep. Among rapid eye movement (REM) sleep, increased REM pressure and elevated REM density are promising candidates for vulnerability markers. Regarding nonREM sleep, a deficit in amount of and latency until slow wave sleep during the first half of the night is a characteristic for depression. To further elucidate whether changes in the microstructure of sleep may serve as vulnerability markers we investigated the premorbid sleep composition in 21 healthy high-risk proband (HRPs) with a positive family history for affective disorders and compared HRPs with a control group of healthy subjects (HCs) without personal and family history for psychiatric disorders. The sleep electroencephalogram (EEG) was conventionally scored and submitted to a quantitative EEG analysis. The main difference in sleep characteristics between HRPs and HCs was an abnormally increased REM density. Differences in the spectral composition of sleep EEG were restricted to an increased power in the sigma frequency range. Since the HRP group comprised six unrelated and 15 related subjects we controlled for sibling effects. We could replicate the increased REM density in the group of HRPs whereas elevated power in the low sigma frequencies persisted only with approaching significance. The present study further supports elevated REM density as putative vulnerability marker for affective disorders. However, sleep EEG in our group of HRPs did not show slow wave sleep abnormalities. Ongoing follow up investigations of HRPs will clarify whether the observed increase in sigma EEG activity during nonREM sleep is of clinical relevance with respect to the likelihood to develop an affective disorder.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Vulnerability markers are supposed to represent proximately and specifically an underlying pathology linked to an increased liability to develop a complex disease. The validation of vulnerability markers requires the verification of distinct biological abnormalities in patients during symptomatic and asymptomatic states of a disease as well as in their healthy first-degree relatives who are at a high-risk to develop the disease (high risk probands, HRPs). The search for vulnerability marker for affective disorders has predominantly focused on stress hormone regulation, brain imaging, and sleep. As to sleep variables a deficit of slow wave sleep in the first sleep cycle, decreased sleep continuity, shortened latency to rapid eye movement (REM) sleep and increased amount of phasic components of REM sleep have been suggested as vulnerability markers [30, 37, 41, 47]. In particular, increased REM density may be a promising candidate since premorbidly elevated REM density in HRPs was associated with an increased likelihood to develop an affective disorder [34]. In addition, persistently increased REM density predicted poor treatment response in depressed patients [5, 8, 24, 44]. Unaffected HRPs also showed a stable reduction of slow wave sleep in their sleep EEG and on the other hand a slow wave sleep deficit in depressed patients was shown to be associated with less favorable outcome of the disease [24, 29, 33].
Most research on sleep related vulnerability markers, however, including our own published findings of the “Munich Vulnerability Study on Affective Disorders” [30, 33, 34] was based on visual analysis of the sleep according to the conventional criteria of Rechtschaffen and Kales [36]. This could have limited the outcome of the studies because findings on neuronal mechanism generating EEG oscillations during sleep emphasized the need for a quantitative analysis of in particular the amount and temporal dynamics of sigma and delta frequencies [13, 42]. It has already been demonstrated in patients with depression that a decreased delta power during nonREM sleep episodes is of clinical relevance [6, 35]. In addition, patients with depression showed signs of a general reduction in the temporal coherence of EEG oscillations indicating a loss of rhythmic organization of sleep [2]. Interestingly, a first study in HRPs also indicated a reduced coherence of sleep EEG frequencies in the beta/delta and theta range [20].
Therefore, we hypothesized that sleep EEG composition is altered also in HRPs for affective disorders. We compared the EEG power spectrum of HRPs with that of control subjects without personal and family history for psychiatric disorders, in particular with respect to the spectral power in the sigma and delta frequencies. We investigated the microstructure of sleep using a whole night spectral analysis. HRPs and controls were recruited from the “Munich Vulnerability Study on Affective Disorders”.
Methods
Subjects
During two recruitment periods of the “Munich Vulnerability Study on Affective Disorders” (1988–1992, 1994–1998) n = 740 psychiatric inpatients with a diagnosis of major depression, bipolar disorder, or “bipolar II” disorder were screened. We identified patients who had at least one first-degree relative with an affective disorder or schizophrenia and at least one first-degree relative with no current or lifetime diagnosis of a psychiatric disorder who was conceived as high risk proband (HRP). The psychiatric examinations to verify diagnoses or absence of diagnoses were done using the Structured Clinical Interview for DSM-III-R [48]. Further details of the selection procedure are described elsewhere [25].
The inclusion criteria mentioned were met by 136 patients, and 50 patients of this group agreed to participate in the study (index patients) providing 101 possible HRPs. Out of these HRPs, a quantitative analysis of sleep EEG was obtained in 21 subjects (mean age 27.1 ± 6.1 years, 12m:9f). The study group of 21 HRPs belonged to 12 families. Thus, our HRP group consisted of six unrelated (2m:4f) and 15 related subjects (10m:5f) with one family providing four, one family three, and four families two HRPs. The corresponding index patients suffered from recurrent major depression (n = 8) or bipolar I disorder (n = 4).
Polysomnography of these HRPs was compared with the sleep EEG 13 healthy control subjects (HCs, mean age 27.5 ± 6.0 years, 4m:9f), who were free of personal and family history of psychiatric disorders. HRPs and HCs did not differ in age (P = 0.865) or gender distribution (Fisher’s exact test P = 0.172).
The study protocol was approved by the local ethical committee. Every proband gave a written informed consent for participation in the study.
Procedure
Before entering the study, HRPs and HCs underwent extensive physical, psychiatric, and laboratory examinations including hematology, virology, clinical chemistry, endocrinology, electroencephalography (EEG), and electrocardiography (ECG) to exclude acute and chronic disease. Details of the procedure are described elsewhere [30]. In short, we excluded subjects with medical treatment for at least 3 months prior to the study, personal history of psychiatric disorders including alcohol and drug abuse, recent stressful life events, sleep disturbances, shift work or a recent transmeridian flight. In addition, thorough clinical exploration and visual inspection of the polysomnographic recordings confirmed that no subject with sleep disorders including insomnia, sleep apnea, periodic movements in sleep syndrome and restless legs syndrome was included. All subjects slept two consecutive nights in our sleep laboratories. Prior to the investigation intake of caffeine or alcohol was not allowed.
Sleep EEG recording
After adaptation to the laboratory setting (first night), sleep was recorded between 11PM and 7AM of the second night. The polysomnographic sleep recordings included two EEGs (C3-A2/C4-A1, time constant 0.3 s, notch filter at 50 Hz, low pass at 70 Hz), a vertical and horizontal electrooculogram (EOG), electromyogram (EMG) and electrocardiogram (ECG). The filtered EOG, EEG, EMG, and ECG signals were transmitted to a polygraph (Schwartzer, ED 24), digitalized via an eight-bit analog-to-digital converter (sampling rate 100 Hz), and stored on disk. Sleep stages were visually scored for consecutive 30 s epochs according to standard guidelines [36] by experienced raters who were blind to the subjects study group assignment. Mean REM density index of the total night or the first REM period was defined as the average ratio of 3-s miniepochs of REM sleep, including REMs, to the total amount of 3-s miniepochs of REM sleep during the total night or the first REM period, respectively. The sleep variables including sleep architecture and sleep continuity were computed as described elsewhere [30].
The quantitative EEG analysis was performed from the C3-A2/C4-A1 EEG derivation using a fast Fourier transformation in order to compute sleep state specific EEG power spectra. State-specific power were computed using 12 2.56 s epochs which had overlapping to match the 30 s epochs of visual sleep scoring as described previously [43]. The spectral power of 50 frequency bins at 0.39 Hz intervals were cumulated across the delta (0.8–3.9 Hz), theta (4.3–7.8 Hz), alpha (8.2–11.7 Hz), low sigma (LSF 12.1–13.7 Hz), high sigma (HSF 14.1–16.0 Hz), total sigma (12.1–14.8 Hz) and beta range (15.2–19.1 Hz)
Additionally, we compared the shape of the two local maxima observed within the theta/alpha (7.0–9.0 Hz) and sigma (12.1–14.8) frequency range between the two groups. We determined the maximal power (peak) of the individual local maximum, the area under the curve (AUC, approximated with the trapezoidal rule), and a second order polynomial indicating the curvature of the local maximum. A local maximum is described by a negative, a local minimum by a positive curvature coefficient.
Statistical analysis
Since the HRP group contained a considerable number of related subjects (15 out of 21, pairs, triplets or quadruplets of siblings) while the subjects of the HCs were all unrelated, we had to control for the effects of an artificial reduction of the within group variance among HRPs due to an increased similarity of related subjects. In order to account for this effect, we compared the mean correlation of n = 13 related pairs of HRP siblings (=four pairs of doublet siblings, three pairs out of one triplet of siblings, six pairs out of one quadruplet of siblings, see Fig. 1) across EEG frequency bands with the mean correlation of all unrelated pairs among the subgroup of HRP siblings (n = 92, total number of all possible pairs among HRP siblings \( {\left( {{\left( {\matrix{ {{15}} \cr {2} \cr } } \right)} = 105} \right)} - n = 13 \) related pairs of HRP siblings; mean intraclass correlation, mean calculation after Fisher-z transformation). Differences between correlation coefficients were evaluated with z tests (after Fisher-z transformation).

Siblings within the HRPs. The group of HRPs comprised a subgroup of related HRPs (n = 15). Therefore, the number of the HRPs was reduced from 21 to 12 with individual results of 15 related HRP substituted by the mean values of the four pairs, one triplet and one quadruplet of siblings (six unrelated HRPs + six means of siblings)
In order to account for the effects of HRP siblings on the group variance we repeated all analyses after substituting the individual results of related HRPs by the mean score of the siblings. Thus, the number of the HRPs was reduced from 21 to 12 with individual results of 15 related HRP substituted by the mean values of the four pairs, one triplet and one quadruplet of siblings (six unrelated HRPs + six means of siblings, see Fig. 1).
Differences in sleep variables and spectral activity between both groups, HRPs and HCs, were evaluated by t tests for independent samples. Associations between conventional sleep variables and spectral activity were evaluated with non-parametric Spearman rank correlation coefficients. Group differences in the local maximum of the theta/alpha and sigma frequency range were calculated non-parametrically by Mann–Whitney U tests due to heterogeneous variances between both groups.
Finally, we examined the spectral change over four consecutive 2-h periods of nonREM sleep with respect to the study groups by multivariate ANOVA for repeated measures
The level of significance was set to P = 0.05 (two-tailed). Differences with a significance level of P < 0.10 are reported as trend. Due to the high intercorrelation between sleep variables and the exploratory nature of the analysis, we refrained from correcting for multiple testing. If not otherwise stated, means and standard deviations are reported.
Results
Similarity of quantitative sleep EEG between HRP siblings
As expected, the subgroup of related pairs of HRP siblings (n = 13 pairs) showed overall higher intra-class correlation coefficients for both nonREM and REM sleep EEG compared to all unrelated pairs of the same subgroup of HRP siblings (n = 92 pairs). These differences were significant for nonREM sleep total spectrum as well as for the combined delta–sigma and sigma–beta frequency range (P < 0.05). In the REM sleep spectrum significant differences could be detected for the theta and the combined sigma–beta frequencies (see Table 1).
All subsequent group comparisons were performed with the individual HRP data and after mean substitution of HRP siblings.
Sleep EEG variables
The variables representing sleep architecture and continuity were similar between the two groups with the exception of a significant increased REM density during the whole night in the HRPs (P < 0.05). There was also a trend towards higher REM density (P = 0.074) and shorter REM sleep period (P = 0.051) during the first sleep cycle in the total group of HRPs (see Table 2). When correcting for the siblings effect by mean substitution we failed to replicate the finding of an increase REM density during the total night (P = 0.113). However, we still found a shorter REM period (P = 0.043) and the trend suggesting higher REM density (P = 0.089) in the first sleep cycle.
Quantitative analysis of sleep EEG
NonREM sleep
There were no significant differences in the spectral composition of nonREM sleep of the whole night between the groups except of a tendency towards a higher power in LSF (12.1–13.7 Hz; P = 0.076) and the total sigma band (12.1–14.8 Hz; P = 0.081). After correcting for the sibling effects in HRPs by mean substitution, we could not find significant differences between controls and HRPs.
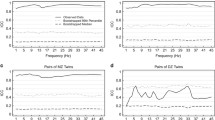
In a subsequent analysis we compared the shape of the two local maxima observed within the theta/alpha (7.0–9.0 Hz) and sigma (12.1–14.8 Hz) frequency range between the two groups. No group differences were found for individual maximum power or for the AUC of the two maxima. However, we found a significantly more pronounced curvature in HRPs in the sigma frequency range which is indicated by a more negative second order polynomial compared with HCs [mean(SD); HRP −0.50 (0.98) vs. HC 0.02 (0.26); Mann–Whitney U test, P = 0.035]. After correction for siblings we could confirm the more pronounced local maximum of the sigma EEG activity among HRPs (Mann–Whitney U test, P = 0.034, see Fig. 2).

Spectral composition of nonREM sleep. The spectral power (±SEM) of nonREM sleep in the group of HRPs (black line) showed a significantly pronounced local maximum in the sigma frequency range (Mann–Whitney U test, P = 0.034) when compared to the group of control subjects (grey line)
Finally, we examined the spectral change over the four consecutive 2-h periods with respect to the study groups by multivariate ANOVA for repeated measures. We found significant changes at the multivariate level (P < 0.001) as well as for all wave bands at the univariate level (P < .05, Greenhouse–Geisser corrected) except for sigma (P = 0.289) and high beta frequency range (P = 0.253). However, no main effects of study group or interactions between change and study group were found. Significant changes during the 2-h periods were also found for the sigma range maximum (P = 0.005), but no interactions with the study groups (P = 0.540). The main effect of a more pronounced curvature of the local maximum in the sigma frequency range among HRPs was confirmed with approaching significance (P = 0.095).
REM sleep
We did not find significant differences in the spectral composition of REM sleep between HRPs and HCs, neither before nor after correction for the sibling effects.
Discussion
We investigated the microstructure of sleep in subjects who are at a high risk for developing affective disorder (HRPs) and compared the sleep characteristics between HRPs and a healthy control group without personal and family history for psychiatric disorders (HCs). Besides conventional scoring of parameters an all-night spectral analysis was conducted to obtain an EEG power spectrum. The subgroup of HRPs in the present study showed a significant increase of their REM density which is in accordance with the results of complete sample of HRPs from the “Munich Vulnerability Study on Affective Disorders” [33, 34]. As to the first sleep cycle a trend towards an elevated REM density was still present after correcting for sibling effects within HRPs. Since increased REM density is a typical abnormality of sleep in depression [30, 33, 41, 47] this parameter is a promising candidate for vulnerability marker [33, 34]. Other studies suggested a shortened REM sleep latency as possible vulnerability marker [22, 23], which could not be confirmed with the sample of HRPs from the present study. However, we observed in another subgroup of HRPs that a cholinergic stimulation test demasked REM sleep dysregulation that were not overt during baseline conditions. In addition, the shortening in REM sleep latency induced by RS 86 appeared to predict the later onset of major depressive and bipolar disorders in those HRPs with a strong family history for affective disorders [31].
The analysis of quantitative EEG data showed a marginal-significant increase in sigma power during nonREM sleep in particular with respect to LSF. When comparing the curvature of the local maxima in the EEG power spectrum this result turned out to be significant. After correction for siblings within the HRPs there was still a significantly more pronounced shape of the local maximum in sigma EEG activity when compared to healthy controls. We could not observe significant differences in all other frequency bands between the groups, in particular there was no reduction in slow wave activity during nonREM sleep in our group of HRPs when compared to the control group. Also the spectral pattern of REM sleep did not differ between HRPs and control subjects.
Dynamics of the spectral power in the sigma frequency range reliably indicate sleep spindle activity [12]. There is good evidence that there are two types of sleep spindles: (1) low frequency sleep spindles predominate in the frontotemporal regions and underlie a strong ontogenetic variation. Low frequency sleep spindles are established in the first months of life, show a second maximum during puberty and usually decrease thereafter. In up to 40% of the general population low frequency sleep spindles persist after puberty [21, 32, 39, 40, 46]. (2) High frequency sleep spindles (14 Hz) with low amplitude are strongly related to the occurrence of slow oscillations and typically occur in centroparietal brain areas [27, 38, 46, 49]. The function of sleep spindles in general and the existence of two types of sleep spindles are still unclear. Different regulatory mechanisms for low and high frequency spindles have been suggested [18, 19, 27, 28]. Interestingly, low and high sleep spindles differ in their occurrence within sleep cycles and throughout the night [1, 14, 43]. The increase in LSF across sleep episodes is thought to maintain sleep in the second part of the night when delta power is already at a low level [14]. Therefore, it may be speculated that the observed increase in particular of LSF in HRPs may indicate an early sign of nonREM sleep dysregulation where the generation of delta sleep is still intact. In addition, in view of the mentioned differences in developmental characteristics of the two kinds of sleep spindles the increased power in LFS may reflect abnormalities in thalamo-cortical pathway maturation in our group of HRPs.
It has been repeatedly demonstrated that individual sleep spindle characteristics are established very early in life and stable thereafter [32, 39, 40]. The trait-like character of spindle characteristics promoted hypothesis on a strong genetic influence on this sleep EEG pattern [10]. In addition, recent studies using elaborate EEG analysis and study designs demonstrated also the strong trait-like character of delta waves [4, 45]. By means of cluster analysis the largest between-subject differences in spectral power were identified in frequencies below 15 Hz and in particular with respect to the delta activity [4]. We observed a significantly higher correlation of delta–sigma frequencies during nonREM sleep in pairs of related HRPs when compared to pairs of HRP siblings who were not related with each other. Therefore, our data further support a genetic influence on the spectral composition of nonREM sleep in particular with respect to the combined occurrence of slow waves and spindles. This is of interest, since more recent studies point to a relation of sleep spindles to memory processes [9, 16] and to general mental abilities, respectively [3].
Various other factors, however, are known to affect spectral composition of nonREM sleep and have to be considered when interpreting the observed differences between HRPs and control subjects. Though sex distribution between the groups did not differ there were three times more men in the HRP than in the control group. Studies on gender effects point to an increase in sleep spindles in women [7, 26]. Therefore, it is unlikely that gender proportion has influenced the observed findings. In addition, the phase of menstrual cycle was shown to affect nonREM sleep that is characterized by an increased EEG activity in the 14–15-Hz range in the luteal phase accompanying an increase in core body temperature [15]. Since our recordings in female participants were not controlled for the phase of the menstrual cycle it cannot be ruled out that this effect may have biased our findings.
It has to be mentioned, however, that changes in sleep spindle characteristics are not typically associated with depression. Up to now, there was only one study demonstrating a significant abnormality of sleep spindles in patients with depression where the authors observed a reduced number and density of sleep spindles when compared with healthy controls [11]. Interestingly, a recent study using a 256-electrode high-density EEG during sleep also observed a spindle deficit in patients with schizophrenia when compared to patients with depression and healthy control subjects [17]. However, it is difficult to rule out subtle drug-induced effects on EEG composition in patients under ongoing psychotropic medication. Therefore, future studies using elaborate techniques to assess EEG composition during sleep have to clarify whether the finding of the present study is of clinical relevance with respect to the likelihood to develop affective disorders.
In summary, the present study confirmed an increased REM density among HRPs, which has been suggested as a possible vulnerability marker for affective disorders. The spectral composition of the sleep in HRPs was characterized by a pronounced local maximum in the low sigma frequency range which may indicate a subtle dysregulation of nonREM sleep.
References
Aeschbach D, Dijk DJ, Borbely AA (1997) Dynamics of EEG spindle frequency activity during extended sleep in humans: relationship to slow-wave activity and time of day. Brain Res 748:131–136
Armitage R, Hoffmann RF, Rush AJ (1999) Biological rhythm disturbance in depression: temporal coherence of ultradian sleep EEG rhythms. Psychol Med 29:1435–1448
Bodizs R, Kis T, Lazar AS, Havran L, Rigo P, Clemens Z, Halasz P (2005) Prediction of general mental ability based on neural oscillation measures of sleep. J Sleep Res 14:285–292
Buckelmüller J, Landolt H-P, Stassen HH, Achermann P (2006) Trait-like individual differences in the human sleep electroencephalogram. Neuroscience 138:351–356
Buysse DJ, Frank E, Lowe KK, Cherry CR, Kupfer DJ (1997) Electroencephalographic sleep correlates of episode and vulnerability to recurrence in depression. Biol Psychiatry 41:406–418
Buysse DJ, Hall M, Begley A, Cherry CR, Houck PR, Land S, Ombao H, Kupfer DJ, Frank E (2001) Sleep and treatment response in depression: new findings using power spectral analysis. Psychiatry Res 103:51–67
Carrier J, Land S, Buysse DJ, Kupfer DJ, Monk TH (2001) The effects of age and gender on sleep EEG power spectral density in the middle years of life (ages 20–60 years old). Psychophysiology 38:232–242
Clark C, Dupont R, Golshan S, Gillin JC, Rapaport MH, Kelsoe JR (2000) Preliminary evidence of an association between increased REM density and poor antidepressant response to partial sleep deprivation. J Affect Disord 59:77–83
Clemens Z, Fabo D, Halasz P (2006) Twenty-four hours retention of visuospatial memory correlates with the number of parietal sleep spindles. Neurosci Lett 403:52–56
De Gennaro L, Ferrara M, Vecchio F, Curcio G, Bertini M (2005) An electroencephalographic fingerprint of human sleep. Neuro-Image 26:114–122
DeMaertelaer V, Hoffman G, Lemaire M, Mendlewicz J (1987) Sleep spindle activity changes in patients with affective disorders. Sleep 10:443–451
Dijk DJ, Hayes B, Czeisler CA (1993) Dynamics of electroencephalographic sleep spindles and slow-wave activity in men: effect of sleep deprivation. Brain Res 626:190–199
Dijk DJ (1995) EEG slow waves and sleep spindles: windows on the sleeping brain. Behav Brain Res 69:109–116
Dijk DJ, Czeisler CA (1995) Contribution of the circadian pacemaker and the sleep homeostat to sleep propensity, sleep structure, electroencephalographic slow waves, and sleep spindle activity in humans. J Neurosci 15:3526–3538
Driver HS, Dijk DJ, Werth E, Biedermann K, Borbély AA (1996) Sleep and the sleep electroencephalogram across the menstrual cycle in young healthy women. J Clin Endocrinol Metab 81:728–735
Gais S, Molle M, Helms K, Born J (2002) Learning-dependent increases in sleep spindle density. J Neurosci 22:6830–6834
Ferrarelli F, Huber R, Peterson MJ, Massimini M, Murphy M, Riedner BA, Watson A, Bria P, Tononi G (2007) Reduced sleep spinale activity in schizophrenia patients. Am J Psychiatry 164:483–492
Friess E, Tagaya H, Trachsel L, Holsboer F, Rupprecht R (1997) Progesterone-induced changes in sleep in male subjects. Am J Physiol 272:E885–891
Friess E, Tagaya H, Grethe C, Trachsel L, Holsboer F (2004) Acute cortisol administration promotes sleep intensity in man. Neuropsychopharmacology 29:598–604
Fulton MK, Armitage R, Rush AJ (2000) Sleep electroencephalographic coherence abnormalities in individuals at high risk for depression: a pilot study. Biol Psychiatry 47:618–625
Gibbs FA, Gibbs EL (1950) Atlas of electroencephalography. Addison-Wesley, Cambridge
Giles DE, Jarrett RB, Roffwarg HP, Rush AJ (1997) Reduced rapid eye movement latency: a predictor of recurrence in depression. J Neuropsychopharmacol 1:33–39
Giles DE, Kupfer DJ, Rush AJ, Roffwarg HP (1998) Controlled comparison of electrophysiological sleep in families of probands with unipolar depression. Am J Psychiatry 155:192–199
Hatzinger M, Hemmeter UM, Brand S, Ising M, Holsboer-Trachsler E (2004) Electroencephalographic sleep profiles in treatment course and long-term outcome of major depression: association with DEX/CRH-test response. J Psychiatr Res 38:453–465
Holsboer F, Lauer CJ, Schreiber W, Krieg JC (1995) Altered hypothalamic-pituitary-adrenocortical regulation in healthy subjects at high familial risk for affective disorders. Neuroendocrinology 62:340–347
Huupponen E, Himanen SL, Varri A, Hasan J, Lehtokangas M, Saarinen J (2002) A study on gender and age differences in sleep spindles. Neuropsychobiology 45:99–105
Jankel WR, Niedermayer E (1985) Sleep spindles. J Clin Neurophysiol 2:1–35
Jobert M, Poiseau E, Jahnig P, Schulz H, Kubicki S (1992) Topographical analysis of sleep spindle activity. Neuropsychobiology 26:210–217
Kupfer DJ, Ehlers CL, Frank E, Grochocinski VJ, McEachran AB, Buhari A (1993) Electroencephalographic sleep studies in depressed patients during long-term recovery. Psychiatry Res 49:121–138
Lauer CJ, Schreiber W, Holsboer F, Krieg JC (1995) In quest of identifying vulnerability markers for psychiatric disorders by all-night polysomnography. Arch Gen Psychiatry 52:145–153
Lauer CJ, Modell S, Schreiber W, Krieg JC, Holsboer F (2004) Prediction of the development of a first major depressive episode with a rapid eye movement sleep induction test using the cholinergic agonist RS 86. J Clin Psychopharmacol 24:356–357
Louis J, Zhang JX, Revol M, Debilly G, Challamel MJ (1992) Ontogenesis of nocturnal organization of sleep spindles: a longitudinal study during the first 6 months of life. Electroencephalogr Clin Neurophysiol 83:289–296
Modell S, Ising M, Holsboer F, Lauer CJ (2002) The munich vulnerability study on affective disorders: stability of polysomnographic findings over time. Biol Psychiatry 52:430–437
Modell S, Ising M, Holsboer F, Lauer CJ (2005) The munich vulnerability study on affective disorders: premorbid polysomnographic profile of affected high-risk probands. Biol Psychiatry 58:694–699
Nissen C, Feige B, Konig A, Voderholzer U, Berger M, Riemann D (2001) Delta sleep ratio as a predictor of sleep deprivation response in major depression. J Psychiatr Res 35:155–163
Rechtschaffen A, Kales A (1968) A manual of standardized terminology, techniques and scoring system for sleep stages of human subjects. National Institute of Neurological Diseases and Blindness, Bethesda
Reynolds CF, Kupfer DJ (1987) Sleep research in affective illness: state of the art circa 1987. Sleep 10:199–215
Scheuler W, Kubicki S, Scholz G, Marquardt J (1990) Two different activities in the sleep spindle frequency band discrimination based on the topographical distribution of spectral power and coherence. In: Horne J (ed) Sleep ‘90. Pontenagel, Bochum, pp 13–16
Shibagaki M, Kiyono S, Watanabe K, Hakamada S (1982) Concurrent occurrence of rapid eye movement with spindle burst during nocturnal sleep in mentally retarded children. Electroencephalogr Clin Neurophysiol 53:27–35
Shinomiya S, Nagata K, Takahashi K, Masumura T (1999) Development of sleep spindles in young children and adolescents. Clin Electroencephalogr 30:39–43
Steiger A, von Bardeleben U, Herth T, Holsboer F (1989) Sleep EEG and nocturnal secretion of cortisol and growth hormone in male patients with endogenous depression before treatment and after recovery. J Affect Disord 16:189–195
Steriade M, McCormick DA, Sejnowski TJ (1993) Thalamocortical oscillations in the sleeping and aroused brain. Science 262:679–685
Tagaya H, Trachsel L, Murck H, Antonijevic I, Steiger A, Holsboer F, Friess E (2000) Temporal dynamics of non-REM sleep episodes in humans. Brain Res 861:233–240
Thase ME, Fasiczka AL, Berman SR, Simons AD, Reynolds CF III (1998) Electroencephalographic sleep profiles before and after cognitive behavior therapy of depression. Arch Gen Psychiatry 55:138–144
Tucker AM, Dinges DF, von Dongen HP (2007) Trait interindividual differences in the sleep physiology of healthy young adults. J Sleep Res 16:170–180
Werth E, Achermann P, Dijk DJ, Borbely AA (1997) Spindle frequency activity in the sleep EEG: individual differences and topographic distribution. Electroencephalogr Clin Neurophysiol 103:535–542
Wichniak A, Riemann D, Kiemen A, Voderholzer U, Jernajczyk W (2000) Comparison between eye movement latency and REM sleep parameters in major depression. Eur Arch Psychiatry Clin Neurosci 250:48–52
Wittchen HU, Zaudig M, Schramm E et al (1990) SKID Strukturiertes Klinisches Interview für DSM-III-R. Beltz-Verlag Weinheim, Germany
Zygierewicz J, Blinowska KJ, Durka PJ, Szelenberger W, Niemcewicz S, Androsiuk W (1999) High resolution study of sleep spindles. Clin Neurophysiol 110:2136–2147
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License ( https://creativecommons.org/licenses/by-nc/2.0 ), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Friess, E., Modell, S., Brunner, H. et al. The Munich vulnerability study on affective disorders: microstructure of sleep in high-risk subjects. Eur Arch Psychiatry Clin Neurosc 258, 285–291 (2008). https://doi.org/10.1007/s00406-007-0795-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00406-007-0795-2