
Abstract
Purpose
Nulliparity and operative vaginal delivery are established risk factor for obstetric anal sphincter injury (OASI). However, risk factors for OASIS occurrence among parous women delivering vaginally are not well-established. We aimed to study the risk factors for OASI occurrence among parous women.
Methods
A retrospective study including all parous women who delivered vaginally at term during 2011–2019 at a university hospital. Deliveries of parous women with OASI were compared to deliveries without OASI. The risk factors associated with OASI were investigated.
Results
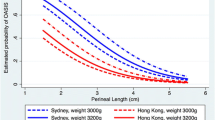
Overall, 35,397 women were included in the study with an OASI rate of 0.4% (n = 144). A higher rate of only one previous vaginal delivery was noted in the OASI group (78.5% vs. 46.4%, OR [95% CI] 4.20, 2.82–6.25, p < 0.001). The rate of vacuum-assisted deliveries was comparable between the study groups. The median birth weight was higher among the OASI group (3566 vs. 3300 g, p < 0.001), as was the rate of macrosomic neonates (19.4% vs. 5.5%, OR [95% CI] 4.15, 2.74–6.29, p < 0.001). On multivariate logistic regression analysis, only two factors were independently positively associated with the occurrence of OASI: a history of only one previous vaginal delivery (adjusted OR [95% CI] 4.34, 2.90–6.49, p = 0.001), and neonatal birth-weight (for each 500 g increment) (adjusted OR [95% CI] 2.51, 1.84–3.44, p < 0.001).
Conclusions
Among parous women, the only factors found to be independently positively associated with OASI were the order of parity and neonatal birth-weight. Vacuum-assisted delivery was not associated with an increased risk of OASI among parous women.


Similar content being viewed by others


Abbreviations
- OASI:
-
Obstetric anal sphincter injury
References
Baghestan E, Irgens LM, Børdahl PE, Rasmussen S (2010) Trends in risk factors for obstetric anal sphincter injuries in Norway. Obstet Gynecol 116:25–34
Kamm MA (1994) Obstetric damage and faecal incontinence. Lancet 344:730–733
de Leeuw JW, Struijk PC, Vierhout ME, Wallenburg HC (2001) Risk factors for third degree perineal ruptures during delivery. BJOG 108:383–387
Haadem K, Gudmundsson S (1997) Can women with intrapartum rupture of anal sphincter still suffer after-effects two decades later? Acta Obstet Gynecol Scand 76:601–603
Sultan AH, Kamm MA, Hudson CN, Bartram CI (1994) Third degree obstetric anal sphincter tears: risk factors and outcome of primary repair. BMJ 308:887–891
Tetzschner T, Sørensen M, Lose G, Christiansen J (1996) Anal and urinary incontinence in women with obstetric anal sphincter rupture. Br J Obstet Gynaecol 103:1034–1040
Bulletins—Obstetrics ACoOaGCoP (2016) Practice bulletin no. 165: prevention and management of obstetric lacerations at vaginal delivery. Obstet Gynecol 128:e1–e15
Pergialiotis V, Vlachos D, Protopapas A, Pappa K, Vlachos G (2014) Risk factors for severe perineal lacerations during childbirth. Int J Gynaecol Obstet 125:6–14
Kudish B, Sokol RJ, Kruger M (2008) Trends in major modifiable risk factors for severe perineal trauma, 1996–2006. Int J Gynaecol Obstet 102:165–170
Elvander C, Ahlberg M, Thies-Lagergren L, Cnattingius S, Stephansson O (2015) Birth position and obstetric anal sphincter injury: a population-based study of 113 000 spontaneous births. BMC Pregnancy Childbirth 15:252
Waldenström U, Ekéus C (2017) Risk of obstetric anal sphincter injury increases with maternal age irrespective of parity: a population-based register study. BMC Pregnancy Childbirth 17:306
Angioli R, Gómez-Marín O, Cantuaria G, O’sullivan MJ (2000) Severe perineal lacerations during vaginal delivery: the University of Miami experience. Am J Obstet Gynecol 182:1083–1085
Thiagamoorthy G, Johnson A, Thakar R, Sultan AH (2014) National survey of perineal trauma and its subsequent management in the United Kingdom. Int Urogynecol J 25:1621–1627
Muraca GM, Skoll A, Lisonkova S et al (2018) Perinatal and maternal morbidity and mortality among term singletons following midcavity operative vaginal delivery versus caesarean delivery. BJOG 125:693–702
Muraca GM, Liu S, Sabr Y et al (2019) Episiotomy use among vaginal deliveries and the association with anal sphincter injury: a population-based retrospective cohort study. CMAJ 191:E1149–E1158
Waldman R (2019) ACOG practice bulletin no. 198: prevention and management of obstetric lacerations at vaginal delivery. Obstet Gynecol 133:185
Bulletins-Obstetrics ACoOaGCoP (2003) Practice bulletin number 49, december: dystocia and augmentation of labor. Obstet Gynecol 102:1445–1454
Salomon LJ, Alfirevic Z, Da Silva CF et al (2019) ISUOG practice guidelines: ultrasound assessment of fetal biometry and growth. Ultrasound Obstet Gynecol 53:715–723
Deane RP (2019) Operative vaginal delivery and pelvic floor complications. Best Pract Res Clin Obstet Gynaecol 56:81–92
Meyer R, Rottenstreich A, Shapira M et al (2020) The role of fetal head circumference in the formation of obstetric anal sphincter injuries following vacuum deliveries among primiparous women. Arch Gynecol Obstet 301:1423
Meyer R, Rottenstreich A, Zamir M et al (2020) Sonographic fetal head circumference and the risk of obstetric anal sphincter injury following vaginal delivery. Int Urogynecol J. https://doi.org/10.1007/s00192-020-04296-3
Laine KSF, Sandvik L et al (2012) Incidence of obstetric anal sphincter injuries after training to protect the perineum: cohort study. BMJ Open 2:e001649. https://doi.org/10.1136/bmjopen-2012001649
Laine K, Gissler M, Pirhonen J (2009) Changing incidence of anal sphincter tears in four Nordic countries through the last decades. Eur J Obstet GynecolReprod Biol 146:71–75
Ginath S, Mizrachi Y, Bar J, Condrea A, Kovo M (2017) Obstetric anal sphincter injuries (OASIs) in Israel: a review of the incidence and risk factors. Rambam Maimonides Med J 8:e0018
DrusanyStarič K, Bukovec P, Jakopič K, Zdravevski E, Trajkovik V, Lukanović A (2017) Can we predict obstetric anal sphincter injury? Eur J Obstet GynecolReprod Biol 210:196–200
Lund NS, Persson LK, Jangö H, Gommesen D, Westergaard HB (2016) Episiotomy in vacuum-assisted delivery affects the risk of obstetric anal sphincter injury: a systematic review and meta-analysis. Eur J Obstet GynecolReprod Biol 207:193–199
Simic M, Cnattingius S, Petersson G, Sandström A, Stephansson O (2017) Duration of second stage of labor and instrumental delivery as risk factors for severe perineal lacerations: population-based study. BMC Pregnancy Childbirth 17:72
Levin G, Rottenstreich A, Cahan T et al (2020) Does birthweight have a role in the effect of episiotomy on anal sphincter injury? Arch Gynecol Obstet 301:171–177
Hsieh WC, Liang CC, Wu D, Chang SD, Chueh HY, Chao AS (2014) Prevalence and contributing factors of severe perineal damage following episiotomy-assisted vaginal delivery. Taiwan J Obstet Gynecol 53:481–485
Kalis V, Laine K, de Leeuw JW, Ismail KM, Tincello DG (2012) Classification of episiotomy: towards a standardisation of terminology. BJOG 119:522–526
Shiono P, Klebanoff MA, Carey JC (1990) Midline episiotomies: more harm than good? Obstet Gynecol 75:765–770
Jangö H, Langhoff-Roos J, Rosthøj S, Sakse A (2014) Modifiable risk factors of obstetric anal sphincter injury in primiparous women: a population-based cohort study. Am J Obstet Gynecol 210(59):e1–6
Lipschuetz M, Cohen SM, Ein-Mor E et al (2015) A large head circumference is more strongly associated with unplanned cesarean or instrumental delivery and neonatal complications than high birthweight. Am J Obstet Gynecol 213:833.e1–33.e12
Lipschuetz M, Cohen SM, Israel A et al (2018) Sonographic large fetal head circumference and risk of cesarean delivery. Am J Obstet Gynecol 218:339.e1–39.e7
Laufe LEBM (1992) Assisted vaginal delivery: obstetric forceps and vacuum extraction techniques. McGraw-Hill, New York
Barbara G, Pifarotti P, Facchin F et al (2016) Impact of mode of delivery on female postpartum sexual functioning: spontaneous vaginal delivery and operative vaginal delivery vs. Cesarean Section. J Sex Med 13:393–401
Kahramanoglu I, Baktiroglu M, Hamzaoglu K, Kahramanoglu O, Verit FF, Yucel O (2017) The impact of mode of delivery on the sexual function of primiparous women: a prospective study. Arch Gynecol Obstet 295:907–916
Funding
No external funding was used in this conduct of this study.
Author information
Authors and Affiliations
Contributions
All authors contributed to the manuscript. GL, RM and AR reviewed the literature and wrote the paper. DS, RYU, AT performed the procedures and collected the data. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
Authors declare that they have no conflict of interest.
Human and animal participants
For this type of study formal consent is not required and was waived by the institutional review board approval. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Levin, G., Rottenstreich, A., Tsur, A. et al. Risk factors for obstetric anal sphincter injury among parous women. Arch Gynecol Obstet 303, 709–714 (2021). https://doi.org/10.1007/s00404-020-05806-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00404-020-05806-w