
Abstract
Purpose
Chemical sphincterotomy (CS) is routinely applied in order to avoid the irreversible anal incontinence associated with the surgical treatment of chronic anal fissure (CAF). However, CS has a lower cure rate than surgery. We developed a screening test (using anal manometry) to separate those patients that are unlikely to benefit from CS and should undergo a more aggressive treatment.
Methods
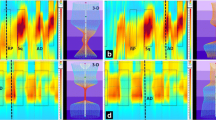
Changes in pressure both at rest and during voluntary contraction of the anal sphincter in 187 patients with chronic anal fissure and 25 healthy subjects (control group) of both sexes were measured. Patients were then sequentially treated (1:1:1) with botulin toxin injections (TOX) (n = 63) or ointments of either nitroglycerine (NTG) (n = 65) or diltiazem (DTZ) (n = 59) for 2 months. The cure rate (overall and for each treatment group) and its relationship with changes in anal pressure were determined.
Results
The overall cure rate was 53% (NTG = 54%, DTZ = 53% and TOX = 51%). Healing was not related to differences in resting or voluntary contraction pressure. However, the probability of healing was associated with an increase in the percentage change between resting and squeeze pressure (PI index) higher than 150% (190 ± 122), similar to that of the control subjects (200 ± 115). Failure of CS was observed in patients with a lower PI (114 ± 77).
Conclusions
The ratio resting/voluntary contraction pressure may be predictive of healing in CAF, thus allowing the selection of patients at high risk of failure of conservative treatment.



Similar content being viewed by others


References
Ortiz H, Marzo J, Armendáriz P et al (2005) Fisura de ano. Alteraciones de la continencia y de la calidad de vida durante la enfermedad y a los 6 meses de la esfinterotomía lateral interna subcutánea. Cir Esp 77:91–95
Klosterhalfen B, Vogel P, Rixen H, Mittermayer C (1989) Topography of the inferior rectal artery: a possible cause of chronic, primary anal fissure. Dis Colon Rectum 32(1):43–52
Utzig MJ, Kroesen AJ, Buhr HJ (2003) Concepts in pathogenesis and treatment of chronic anal fissure. A review of the literature. Am J Gastroenterol 98:968–974
Nelson R (2006) Non surgical therapy for anal fissure. Cochrane Database Syst Rev 18(4):CD003431, Review
Essani R, Sarkisyan G, Beart RW et al (2005) Cost-saving effect of treatment algorithm for chronic anal fissure: a prospective analysis. J Gastrointest Surg 9(9):1237–1243
Haq Z, Rahman M, Chowdhury RA et al (2005) Chemical sphincterotomy-first line of treatment for chronic anal fissure. Mymensingh Med J 14(1):88–90
Parellada C (2004) Randomized, prospective trial comparing 0.2 percent isosorbide dinitrate ointment with sphincterotomy in treatment of chronic anal fissure: a two-year follow-up. Dis Colon Rectum 47(4):437–443
Mishra R, Thomas S, Maan MS et al (2005) Topical nitroglycerin versus lateral internal sphincterotomy for chronic anal fissure: prospective, randomized trial. Anz J Surg 75(12):1032–1035
Romano G, Rotondano G, Santangelo M, Esercizio L (1994) A critical appraisal of pathogenesis and morbidity of surgical treatment of chronic anal fissure. J Am Coll Surg 178(6):600–604
Bove A, Balzano A, Perrotti P et al (2004) Different anal pressure profiles in patients with anal fissure. Tech Coloproctol 8(3):151–156, discussion 156-157
Pascual M et al (2005) Endosonographic and manometric assessment of the internal anal sphincter in patients with chronic anal fissure. Cir Esp 77(1):27–30
Mínguez M, Tomás-Ridocci M, Moreno-Osset E et al (2005) Características presivas del canal anal en los sujetos normales. Influencia de la edad y el sexo. Gastroenterología y Hepatología 10-17
Taylor BM, Beart RW Jr, Phillips S (1984) Longitudinal…radial variations of pressure in the human anal sphincter. Gastroenterology 86:693–697
Ho KS, Ho YH (2005) Randomized clinical trial comparing oral nifedipine with lateral anal sphincterotomy and tailored sphincterotomy in the treatment of chronic anal fissure. Br J Surg 92(4):403–408
Thornton J, Kennedy ML, King DW (2005) Prospective manometric assessment of botulinum toxin and its correlation with healing of chronic anal fissure. Dis Colon Rectum 48:1207–1212
Madalinski M, Chodorowski Z (2006) Why the most potent toxin may heal anal fissure. Adv Ther 23(4):627–634
Madalinski M, Kalinowski L (2009) Novel options for the pharmacological treatment of chronic anal fissure—role of botulin toxin. Curr Clin Pharmacol 4(1):47–52
Rosales RL, Arimura K, Takenaga S, Osame M (1996) Extrafusal and intrafusal muscle effects in experimental botulinum toxin-A injection. Muscle Nerve 19(4):488–496
Burgueño MJ, Garcia Bastos JL, Gonzalez-Buitrago JM (1995) Las curvas ROC en la evaluación de las pruebas diagnósticas. Med Clin (Barc) 104:661–670
Minguez M, Melo F, Espi A et al (1999) Therapeutic effects of different doses of botulinum toxin in chronic anal fissure. Dis Colon Rectum 42(8):1016–1021
Lindsey I, Jones OM, Cunningham C et al (2004) Chronic anal fissure. Br J Surg 91(3):270–279
Jones OM (2007) Towards safer treatments for benign anorectal disease: the pharmacological manipulation of the internal anal sphincter. Ann R Coll Surg Engl 89(6):574–579
Acknowledgements
We thank Professor Manuel Canteras for his kind assistance in performing statistical analysis; Professor Francisco J Fenoy and Dr. Graciela Valero and Ma Dolores Frutos for their kind assistance in the preparation of the manuscript.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gil, J., Luján, J., Hernández, Q. et al. Screening for the effectiveness of conservative treatment in chronic anal fissure patients using anorectal manometry. Int J Colorectal Dis 25, 649–654 (2010). https://doi.org/10.1007/s00384-010-0885-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-010-0885-x