
Abstract
Background
The diagnosis and management of neonatal pneumoperitoneum revolves around necrotizing enterocolitis (NEC) in most of the published literature. Although NEC remains the major cause of pneumoperitoneum in a neonate, there are several other causes leading to free air in the peritoneal cavity. A number of case reports have appeared describing pneumoperitoneum in a newborn due to rupture of one particular organ, but there have been only few collective reviews on the subject. The present study shares the experience with neonates admitted with a diagnosis of pneumoperitoneum in a pediatric surgical center of a developing country. The various causes of pneumoperitoneum in a newborn, their management and subsequent outcome are described.
Materials and methods
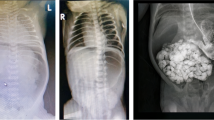
The study was conducted in the Department of Pediatric Surgery, CSMMU (upgraded King Georges Medical College), Lucknow, India. All the neonates admitted with a diagnosis of pneumoperitoneum during the period of last 3 years (2005–2008) were retrospectively analyzed. Other neonatal admissions were also retrieved for the same period. Free air was confirmed by erect abdominal X-ray or lateral decubitus films in certain cases. The data sheets were analyzed regarding age of presentation, cause of bowel perforation, management offered and subsequent outcome achieved. All patients of NEC without evidence of perforation were not included in the study (n = 21).
Results
Out of total 537 neonatal admissions, 89 (16.5%) neonates were admitted with a diagnosis of pneumoperitoneum. There were 79 (88.7%) males and only 10 (11.6%) female neonates admitted during the study period. All of them had evidence of pneumoperitoneum at the time of admission. The age at presentation ranged from 4 to 32 days. NEC remained the single major cause of pneumoperitoneum in the newborn; however, in 44 (49.4%) patients the cause was not related to NEC. Perforated pouch colon, isolated colonic perforations, caecal perforations, gastric and duodenal perforations were the main causes of pneumoperitoneum not related to NEC. There were seven patients in whom no cause of pneumoperitoneum could be ascertained. The treatment was individualized according to the presentation. Most of the NEC-related perforations were managed by peritoneal drains. Laparotomy was done in rest of the patients. Three patients were managed conservatively. Overall, 19 (21.6%) patients expired. Most of those expired were of low birth weight with NEC and congenital pouch colon with perforation.
Conclusion
Neonatal pneumoperitoneum remains a surgical emergency and outcome can be lethal if the problem is not addressed early. NEC remains the major cause; however, there are several other important causes of isolated gastrointestinal perforations leading to neonatal pneumoperitoneum. The management should be individualized in these patients and the outcome largely depends on the early recognition of the condition.

Similar content being viewed by others


References:
Grosfeld JL et al (1996) Gastrointestinal perforation and peritonitis in infants and children: experience with 179 cases over ten years. Surgery 120:650–656
Calisti A, Perfrelli L et al (2004) Surgical approach to neonatal intestinal perforations. Minerva Pediatr 56:335–339
Kim SS, Albanese CT (2006) Necrotizing enterocolitis. In: Grosfeld JL, O’Neil JA, Fonkalsrud EW, Coran AG (eds) Pediatric surgery, chap 92, 6th edn. Mosby Inc., pp 1437
Sharma SB et al (2004) Gastrointestinal perforations in neonates with anorectal malformations. Indian J Gastroenterol 23:107–108
Chirdan LB, Ameh EA (2001) Neonatal intestinal perforation in a developing country. Ann Trop Paediatr 21(1):26–28
Cruze S, Snyder WH (1961) Acute perforation of the alimentary tract in infancy and childhood. Ann Surg 154:93–99
Mestel AL, Trusler GA et al (1996) Pneumoperitoneum in the newborn. Can Med Assoc J 95:201–204
de Feiter PW et al (2006) Rectal perforations after barium enema: a review. Dis Colon Rectum 49(2):261–271
Swenson O, Sherman JO, Fisher JH (1973) Diagnosis of congenital megacolon: an analysis of 501 patients. J Pediatr Surg 8:587–594
Newman B, Nussbaum A, Kirkpatrick JA Jr (1987) Bowel perforation in Hirschsprung’s disease. AJR Am J Roentgenol 148:1195–1197
Chiba T, Ohi R et al (1991) Ileal atresia with perforation in siblings. Eur J Pediatr Surg 1(1):51–53
Benjamin PK, Thompson JE et al (1990) Complications of mechanical ventilation in a children’s hospital multidisciplinary intensive care unit. Respir Care 35:873–878
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Khan, T.R., Rawat, J.D., Ahmed, I. et al. Neonatal pneumoperitoneum: a critical appraisal of its causes and subsequent management from a developing country. Pediatr Surg Int 25, 1093–1097 (2009). https://doi.org/10.1007/s00383-009-2488-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00383-009-2488-6