
Abstract
Introduction
Nonsyndromic, multi-suture craniosynostosis is not common, especially those involving unilateral coronal and lambdoid sutures. Based on the experience on 6 cases, we analyzed the skull morphology of combined unilateral coronal-lambdoid suture synostosis and evaluated the surgical outcome of suturectomy.
Methods
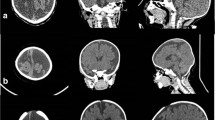
Patients who underwent an operation for craniosynostosis in Seoul National University Children’s Hospital from 2010 to 2018 were reviewed. For qualitative analysis of the surgical outcome, five typical morphologic characteristics (ipsilateral superior orbital rim deviation, deviation of the nasal ridge, ipsilateral frontal flattening, contralateral parietal bulging, ipsilateral occipitomastoid bulging) in unilateral coronal-lambdoid suture synostosis were evaluated based on medical photos, plain skull radiographs, and CT scans. For quantitative analysis, three parameters (nasal root deviation, orbital asymmetry, posterior skull base deviation) were measured.
Results
Among 316 patients with craniosynostosis, 41 patients had nonsyndromic, multi-suture synostosis. There were 6 unilateral coronal-lambdoid suture synostosis patients who were all treated with suturectomy. Qualitative evaluation of the postoperative outcome revealed that the nasal root and orbital rim deviations and the contralateral occipitomastoid bulging showed satisfactory improvements. However, ipsilateral frontal flattening and contralateral parietal bulging were improved but still present in most cases. Quantitative, craniometric analysis supported the qualitative outcomes. The nasal ridge deviation angle was corrected from 7.04 to 1.79 degrees. The posterior skull base deviation angle improved from 6.29 to 3.55 degrees.
Conclusion
Unilateral coronal-lambdoid suture synostosis suturectomy followed by helmet therapy resulted in favorable outcomes, although the correction of frontal flattening was less satisfactory than the other measures. Considering the minimal invasiveness of the treatment, suturectomy may be a viable option for these patients.





Similar content being viewed by others

References
Kolar JC (2011) An epidemiological study of nonsyndromal craniosynostoses. J Craniof Surg 22:47–49
Chumas PD, Cinalli G, Arnaud E, Marchac D, Renier D (1997) Classification of previously unclassified cases of craniosynostosis. J Neurosurg 86:177–181
Greene AK, Mulliken JB, Proctor MR, Meara JG, Rogers GF (2008) Phenotypically unusual combined craniosynostoses: presentation and management. Plast Reconstr Surg 122:853–862
Sloan GM, Wells KC, Raffel C, McComb JG (1997) Treatment of craniosynostosis: outcome analysis of 250 consecutive patients. Pediatrics 100:e2
Chong S, Wang KC, Phi JH, Lee JY, Kim SK (2016) Minimally invasive suturectomy and postoperative helmet therapy : advantages and limitations. J Korean Neurosurg Soc 59:227–232
Yan H, Abel TJ, Alotaibi NM, Anderson M, Niazi TN, Weil AG, Fallah A, Phillips JH, Forrest CR, Kulkarni AV, Drake JM, Ibrahim GM (2018) A systematic review of endoscopic versus open treatment of craniosynostosis. Part 2: the nonsagittal single sutures. J Neurosurg Pediatr 22:361–368
Rivero-Garvia M, Marquez-Rivas J, Rueda-Torres AB, Ollero-Ortiz A (2012) Early endoscopy-assisted treatment of multiple-suture craniosynostosis. Childs Nerv Syst 28:427–431
Wilkie AOM, Johnson D, Wall SA (2017) Clinical genetics of craniosynostosis. Curr Opin Pediatr 29:622–628
Whitaker LA, Bartlett SP, Schut L, Bruce D (1987) Craniosynostosis - an analysis of the timing, treatment, and complications in 164 consecutive patients. Plast Reconstr Surg 80:195–206
Wes AM, Mazzaferro D, Naran S, Bartlett SP, Taylor JA (2017) Nasal root deviation in unicoronal craniosynostosis: a craniometric analysis of early and late postoperative outcomes. J Craniofac Surg 28:1220–1223
Domeshek LF, Woo A, Skolnick GB, Naidoo S, Segar D, Smyth M, Proctor M, Patel KB (2019) Postoperative changes in orbital dysmorphology in patients with unicoronal synostosis. J Craniofac Surg 30:483–488
Ploplys EA, Hopper RA, Muzaffar AR, Starr JR, Avellino AM, Cunningham ML, Ellenbogen RG, Gruss JS (2009) Comparison of computed tomographic imaging measurements with clinical findings in children with unilateral lambdoid synostosis. Plast Reconstr Surg 123:300–309
Tamburrini G, Caldarelli M, Massimi L, Santini P, Di Rocco C (2005) Intracranial pressure monitoring in children with single suture and complex craniosynostosis: a review. Childs Nerv Syst 21:913–921
Di Rocco F, Arnaud E, Renier D (2009) Evolution in the frequency of nonsyndromic craniosynostosis clinical article. J Neurosurg Pediatr 4:21–25
Byun IH, Hong JW, Hussein MA, Kim YO (2018) Demographic characteristics of craniosynostosis patients in Asia. J Cranio-Maxillofac Surg 46:674–678
Delashaw JB, Persing JA, Broaddus WC, Jane JA (1989) Cranial vault growth in craniosynostosis. J Neurosurg 70:159–165
Dobbs TD, Salahuddin O, Jayamohan J, Richards P, Magdum S, Wall SA, Johnson D (2017) The management of trigonoscaphocephaly as a result of combined metopic and sagittal synostosis. Plast Reconstr Surg 139:1325E–1332E
Jimenez DF, Barone CM (2010) Multiple-suture nonsyndromic craniosynostosis: early and effective management using endoscopic techniques clinical article. J Neurosurg Pediatr 5:223–231
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hwang, J.H., Yang, J., Kim, K.H. et al. Combined unilateral coronal-lambdoid suture synostosis: surgical outcome of suturectomy and postoperative helmet therapy. Childs Nerv Syst 37, 277–286 (2021). https://doi.org/10.1007/s00381-020-04650-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-020-04650-2