
Abstract
Objectives
To determine whether single-phase dual-energy CT (DECT) differentiates vascular and nonvascular renal lesions in the portal venous phase (PVP). Optimal iodine threshold was determined and compared to Hounsfield unit (HU) measurements.
Methods
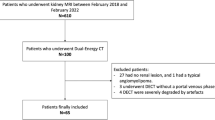
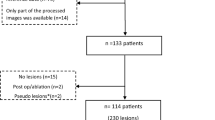
We retrospectively included 250 patients (266 renal lesions) who underwent a clinically indicated PVP abdominopelvic CT on a rapid-kilovoltage-switching single-source DECT (rsDECT) or a dual-source DECT (dsDECT) scanner. Iodine concentration and HU measurements were calculated by four experienced readers. Diagnostic accuracy was determined using biopsy results and follow-up imaging as reference standard. Area under the curve (AUC) was calculated for each DECT scanner to differentiate vascular from nonvascular lesions and vascular lesions from hemorrhagic/proteinaceous cysts. Univariable and multivariable logistic regression analyses evaluated the association between variables and the presence of vascular lesions.
Results
A normalized iodine concentration threshold of 0.25 mg/mL yielded high accuracy in differentiating vascular and nonvascular lesions (AUC 0.93, p < 0.001), with comparable performance to HU measurements (AUC 0.93). Both iodine concentration and HU measurements were independently associated with vascular lesions when adjusted for age, gender, body mass index, and lesion size (AUC 0.95 and 0.95, respectively). When combined, diagnostic performance was higher (AUC 0.96). Both absolute and normalized iodine concentrations performed better than HU measurements (AUC 0.92 vs. AUC 0.87) in differentiating vascular lesions from hemorrhagic/proteinaceous cysts.
Conclusion
A single-phase (PVP) DECT scan yields high accuracy to differentiate vascular from nonvascular renal lesions. Iodine concentration showed a slightly higher performance than HU measurements in differentiating vascular lesions from hemorrhagic/proteinaceous cysts.
Key Points
• A single-phase dual-energy CT scan in the portal venous phase differentiates vascular from nonvascular renal lesions with high accuracy (AUC 0.93).
• When combined, iodine concentration and HU measurements showed the highest diagnostic performance (AUC 0.96) to differentiate vascular from nonvascular renal lesions.
• Compared to HU measurements, iodine concentration showed a slightly higher performance in differentiating vascular lesions from hemorrhagic/proteinaceous cysts.




Similar content being viewed by others

Abbreviations
- BMI:
-
Body mass index
- CT:
-
Computed tomography
- DECT:
-
Dual-energy CT
- dsDECT:
-
Dual-source DECT scanner
- HU:
-
Hounsfield unit
- keV:
-
Kiloelectron volt
- kVp:
-
Kilovoltage peak
- PACS:
-
Picture archive and communication system
- PVP:
-
Portal venous phase
- ROC:
-
Receiver operating curves
- ROI:
-
Region of interest
- rsDECT:
-
Rapid-kilovoltage-switching single-source DECT
- VIF:
-
Variance inflation factor
- VUE:
-
Virtual unenhanced images
References
Patel BN, Alexander L, Allen B et al (2017) Dual-energy CT workflow: multi-institutional consensus on standardization of abdominopelvic MDCT protocols. Abdom Radiol (NY) 42:676–687
Marin D, Boll DT, Mileto A, Nelson RC (2014) State of the art: dual-energy CT of the abdomen. Radiology 271:327–342
McCollough CH, Leng S, Yu L, Fletcher JG (2015) Dual- and multi-energy CT: principles, technical approaches, and clinical applications. Radiology 276:637–653
Patel BN, Thomas JV, Lockhart ME, Berland LL, Morgan DE (2013) Single-source dual-energy spectral multidetector CT of pancreatic adenocarcinoma: optimization of energy level viewing significantly increases lesion contrast. Clin Radiol 68:148–154
Murray N, Darras KE, Walstra FE, Mohammed MF, McLaughlin PD, Nicolaou S (2019) Dual-energy ct in evaluation of the acute abdomen. Radiographics 39:264–286
Marcon J, Graser A, Horst D et al (2020) Papillary vs clear cell renal cell carcinoma. Differentiation and grading by iodine concentration using DECT-correlation with microvascular density. Eur Radiol 30:1–10
Pourvaziri A, Parakh A, Mojtahed A, Kambadakone A, Sahani DV (2019) Diagnostic performance of dual-energy CT and subtraction CT for renal lesion detection and characterization. Eur Radiol 29:6559–6570
Patel BN, Vernuccio F, Meyer M et al (2019) Dual-energy CT material density iodine quantification for distinguishing vascular from nonvascular renal lesions: normalization reduces intermanufacturer threshold variability. AJR Am J Roentgenol 212:366–376
Meyer M, Nelson RC, Vernuccio F et al (2019) Comparison of iodine quantification and conventional attenuation measurements for differentiating small, truly enhancing renal masses from high-attenuation nonenhancing renal lesions with dual-energy CT. AJR Am J Roentgenol. https://doi.org/10.2214/AJR.18.20547:W1-W11
Zarzour JG, Milner D, Valentin R et al (2017) Quantitative iodine content threshold for discrimination of renal cell carcinomas using rapid kV-switching dual-energy CT. Abdom Radiol (NY) 42:727–734
Marin D, Davis D, Roy Choudhury K et al (2017) Characterization of small focal renal lesions: diagnostic accuracy with single-phase contrast-enhanced dual-energy ct with material attenuation analysis compared with conventional attenuation measurements. Radiology 284:737–747
Mileto A, Marin D, Ramirez-Giraldo JC et al (2014) Accuracy of contrast-enhanced dual-energy MDCT for the assessment of iodine uptake in renal lesions. AJR Am J Roentgenol 202:W466–W474
Ascenti G, Mileto A, Krauss B et al (2013) Distinguishing enhancing from nonenhancing renal masses with dual-source dual-energy CT: iodine quantification versus standard enhancement measurements. Eur Radiol 23:2288–2295
Kaza RK, Caoili EM, Cohan RH, Platt JF (2011) Distinguishing enhancing from nonenhancing renal lesions with fast kilovoltage-switching dual-energy CT. AJR Am J Roentgenol 197:1375–1381
Graser A, Becker CR, Staehler M et al (2010) Single-phase dual-energy CT allows for characterization of renal masses as benign or malignant. Investig Radiol 45:399–405
Graser A, Johnson TR, Hecht EM et al (2009) Dual-energy CT in patients suspected of having renal masses: can virtual nonenhanced images replace true nonenhanced images? Radiology 252:433–440
Patel BN, Boltyenkov AT, Martinez MG et al (2020) Cost-effectiveness of dual-energy CT versus multiphasic single-energy CT and MRI for characterization of incidental indeterminate renal lesions. Abdom Radiol (NY) 45:1896–1906
Salameh JP, McInnes MDF, McGrath TA, Salameh G, Schieda N (2019) Diagnostic accuracy of dual-energy CT for evaluation of renal masses: systematic review and meta-analysis. AJR Am J Roentgenol 212:W100–W105
Bellini D, Panvini N, Laghi A et al (2019) Systematic review and meta-analysis investigating the diagnostic yield of dual-energy CT for renal mass assessment. AJR Am J Roentgenol. https://doi.org/10.2214/AJR.18.20625:1-10
Obmann MM, Cosentino A, Cyriac J et al (2020) Quantitative enhancement thresholds and machine learning algorithms for the evaluation of renal lesions using single-phase split-filter dual-energy CT. Abdom Radiol (NY) 45:1922–1928
Sica GT (2006) Bias in research studies. Radiology 238:780–789
Patel BN, Farjat A, Schabel C et al (2018) Energy-specific optimization of attenuation thresholds for low-energy virtual monoenergetic images in renal lesion evaluation. AJR Am J Roentgenol 210:W205–W217
Krauss B, Grant KL, Schmidt BT, Flohr TG (2015) The importance of spectral separation: an assessment of dual-energy spectral separation for quantitative ability and dose efficiency. Investig Radiol 50:114–118
Li X, Meng X, Ye Z (2016) Iodine quantification to characterize primary lesions, metastatic and non-metastatic lymph nodes in lung cancers by dual energy computed tomography: An initial experience. Eur J Radiol 85:1219–1223
Liang P, Ren XC, Gao JB, Chen KS, Xu X (2017) Iodine concentration in spectral CT: assessment of prognostic determinants in patients with gastric adenocarcinoma. AJR Am J Roentgenol 209:1033–1038
Silverman SG, Israel GM, Trinh QD (2015) Incompletely characterized incidental renal masses: emerging data support conservative management. Radiology 275:28–42
Silverman SG, Pedrosa I, Ellis JH et al (2019) Bosniak Classification of cystic renal masses, Version 2019: an update proposal and needs assessment. Radiology 292:475–488
Corwin MT, Altinmakas E, Asch D et al (2020) Clinical importance of incidental homogeneous renal masses 10-40 mm and 21-39 Hounsfield Units at portal venous-phase CT: A 12-institution retrospective cohort study. AJR Am J Roentgenol. https://doi.org/10.2214/AJR.20.24245
Hu EM, Ellis JH, Silverman SG, Cohan RH, Caoili EM, Davenport MS (2018) Expanding the definition of a benign renal cyst on contrast-enhanced CT: can incidental homogeneous renal masses measuring 21-39 HU be safely ignored? Acad Radiol 25:209–212
Silverman SG, Israel GM, Herts BR, Richie JP (2008) Management of the incidental renal mass. Radiology 249:16–31
Corwin MT, Hansra SS, Loehfelm TW, Lamba R, Fananapazir G (2018) Prevalence of solid tumors in incidentally detected homogeneous renal masses measuring > 20 HU on portal venous phase CT. AJR Am J Roentgenol 211:W173–W177
Silverman SG, Gan YU, Mortele KJ, Tuncali K, Cibas ES (2006) Renal masses in the adult patient: the role of percutaneous biopsy. Radiology 240:6–22
Lin YM, Chiou YY, Wu MH, Huang SS, Shen SH (2018) Attenuation values of renal parenchyma in virtual noncontrast images acquired from multiphase renal dual-energy CT: Comparison with standard noncontrast CT. Eur J Radiol 101:103–110
Funding
The authors state that this work has not received any funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Guarantor
The scientific guarantor of this publication is Bhavik Patel, MD, MBA.
Conflict of interest
The authors of this manuscript declare relationships with the following companies:
DoMa activities related to the present article: none. Activities not related to the present article: research grant from the National Institute of Biomedical Imaging and Bioengineering (5T32EB009035). Shareholder of Segmed, Inc. Consultant for Segmed, Inc. Other relationships: no relevant relationships.
MW activities related to the present article: none. Activities not related to the present article: research grants from American Heart Association (18POST34030192), Philips Healthcare, and Stanford University, consulting for Arterys, Inc, and co-founder/shareholder of Segmed, Inc. Other relationships: no relevant relationships.
BP has research support from General Electric through an institutional grant outside of the submitted work.
The other authors have no conflict of interest to disclose.
Statistics and biometry
One of the authors has significant statistical expertise.
Informed consent
Written informed consent was waived by the Institutional Review Board.
Ethical approval
Institutional Review Board approval was obtained.
Methodology
• Retrospective
• Experimental
• Performed at one institution
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Table 6
– Univariable and multivariable logistic regression models evaluating the associations between variables and the presence of vascular lesions compared to non-vascular lesions. Table 7 – Univariable and multivariable logistic regression models evaluating the associations between variables and the presence of vascular lesions compared to hemorrhagic/proteinaceous cysts. (DOCX 29 kb)
Rights and permissions
About this article

Cite this article
Mastrodicasa, D., Willemink, M.J., Madhuripan, N. et al. Diagnostic performance of single-phase dual-energy CT to differentiate vascular and nonvascular incidental renal lesions on portal venous phase: comparison with CT. Eur Radiol 31, 9600–9611 (2021). https://doi.org/10.1007/s00330-021-08097-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-021-08097-0