
Abstract
Objectives
To determine normal pericoronary adipose tissue mean attenuation (PCATMA) values for left the anterior descending (LAD), left circumflex (LCX), and right coronary artery (RCA) in patients without plaques on coronary CT angiography (cCTA), taking into account tube voltage influence.
Methods
This retrospective study included 192 patients (76 (39.6%) men; median age 49 years (range, 19–79)) who underwent cCTA with third-generation dual-source CT for the suspicion of CAD between 2015 and 2017. We selected patients without plaque on cCTA. PCATMA was measured semi-automatically on cCTA images in the proximal segment of the three main coronary arteries with 10 mm length. Paired t-testing was used to compare PCATMA between combinations of two coronary arteries within each patient, and one-way ANOVA testing was used to compare PCATMA in different kV groups.
Results
The overall mean ± standard deviation (SD) PCATMA was − 90.3 ± 11.1 HU. PCATMA in men was higher than that in women: − 88.5 ± 10.5 HU versus − 91.5 ± 11.3 HU (p = 0.001). PCATMA of LAD, LCX, and RCA was − 92.4 ± 11.6 HU, − 88.4 ± 9.9 HU, and − 90.2 ± 11.4 HU, respectively. Pairwise comparison of the arteries showed significant difference in PCATMA: LAD and LCX (p < 0.001), LAD and RCA (p = 0.009), LCX and RCA (p = 0.033). PCATMA of the 70 kV, 80 kV, 90 kV, 100 kV, and 120 kV groups was − 95.6 ± 9.6 HU, − 90.2 ± 11.5 HU, − 87.3 ± 9.9 HU, − 82.7 ± 6.2 HU, and − 79.3 ± 6.8 HU, respectively (p < 0.001).
Conclusions
In patients without plaque on cCTA, PCATMA varied by tube voltage, with minor differences in PCATMA between coronary arteries (LAD, LCX, RCA). PCATMA values need to be interpreted taking into account tube voltage setting.
Key Points
• In patients without plaque on cCTA, PCAT MA differs slightly by coronary artery (LAD, LCX, RCA).
• Tube voltage of cCTA affects PCAT MA measurement, with mean PCAT MA increasing linearly with increasing kV.
• For longitudinal cCTA analysis of PCAT MA , the use of equal kV setting is strongly recommended.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Coronary artery disease (CAD) is caused by atherosclerosis of the coronary arteries. Prior studies showed that coronary inflammation plays an essential role in the development and progression of atherosclerotic plaque [1,2,3]. An observational study demonstrated that invasively determined inflammatory changes of the coronary wall are present in early stages of CAD [4]. In the CANTOS trial, anti-inflammatory therapy reduced cardiovascular events, independent of lipid-lowering therapies [5, 6]. Efforts have been made to find a reliable non-invasive imaging parameter to detect coronary inflammation, focusing on adipose tissue [7,8,9,10]. The amount of epicardial adipose tissue (EAT) has been quantified [11,12,13], not only based on coronary computed tomography angiography (cCTA) but also based on coronary calcium scans or non-gated chest CTs [14, 15]. More recently, attention was focused on pericoronary adipose tissue (PCAT). Although PCAT is part of EAT, morphological and functional characteristics of PCAT are different from those of EAT. PCAT is directly affected by coronary inflammation, causing compositional changes of PCAT, while EAT is mainly affected by systemic conditions such as obesity [16]. A clinical pathology review suggested PCAT to be an independent risk factor for cardiovascular disease [17]. Antonopoulos et al indirectly evaluated coronary inflammation on cCTA around the RCA by measuring the fat attenuation index, equivalent to PCAT mean attenuation (PCATMA) [16]. They found a correlation between cCTA-derived PCATMA and adipocyte size or PCAT lipid volume in ex vivo PCAT histology. Additionally, PCAT and the coronary wall had a bidirectional communication, where inflammatory processes in the coronary vessel wall influenced PCAT composition via a paracrine pathway [16, 18]. In turn, PCAT influenced the coronary wall by secreted bioactive inflammation molecules [19]. In the presence of increased inflammation, higher CT attenuation of PCAT is expected [16].
Thus, PCAT could potentially be used as a non-invasive proxy to assess coronary inflammation based on routine cCTA imaging, and could offer valuable information for early diagnosis, treatment, and prevention of CAD. Several studies explored the diagnostic value of PCATMA in patients with plaques [20,21,22,23,24]. However, studies including patients without plaque so far mainly focused on the healthy RCA in small cohorts of patients. Further standardization and validation, as well as reference PCATMA values in all three main coronary arteries without plaque, are needed before generalized clinical implementation can be considered. Reference values of PCATMA for healthy patients are necessary for the application in diseased patients because based on the healthy reference values clinicians may in the future be able to classify the coronary arteries into healthy or vulnerable vessels, even before the presence of plaque. Additionally, clinical cCTA scans are acquired at different tube voltages depending on patient characteristics and CT systems. Differences in tube voltage affect Hounsfield Unit (HU) values measured in different tissues. However, so far, no study has actually studied the magnitude of the effect of the tube voltage on PCAT. Potential future cutoff values in PCAT need to be seen in perspective of difference by tube voltage, and may need adjustment by kV setting.
The objectives of this study were to explore PCATMA reference values of three main coronary arteries in patients without plaque on cCTA, and to determine the influence of cCTA tube voltages and vessel analyzed on PCATMA measurement.
Materials and methods
Study population
This retrospective, single-center observational study was performed at the University Medical Center Groningen, Groningen, The Netherlands. The study was compliant with the Declaration of Helsinki. The study protocol was approved by the institutional ethical review board, and informed consent was waived. Patients were eligible if they were suspected of coronary artery disease and underwent routine cCTA between January 2015 and November 2017. The cohort list was randomly screened for patients meeting the inclusion criteria until the required sample size was reached; see sample size calculations in the statistical paragraph. Inclusion criteria were (1) calcium score of 0 and (2) no coronary plaque on cCTA. Exclusion criteria were (1) objection to the use of data for scientific research; (2) poor cCTA image quality; and (3) patients with anomalous coronary artery origin from the aorta sinus that leads to inaccurate measurements. A radiologist with 10 years of experience re-evaluated all calcium scoring and cCTA scans. In case of doubt, a radiologist with 14 years of experience performed a second reading.
cCTA scan and post-processing protocol
Third-generation dual-source CT was used (Somatom Force; Siemens Healthineers). A non-enhanced electrocardiography (ECG)-triggered CT acquisition was performed to obtain the calcium score. cCTA was performed according to standard clinical protocol. Patients received sublingual nitroglycerin unless contra-indicated. In case of high heart rate (> 70–73 beats/min), patients received an intravenous beta-blocker. cCTA was acquired in high-pitch mode in case of regular heart rate < 70 beats/min, in sequential mode in diastolic phase if heart rate was > 70 beats/min, and in sequential mode with broad ECG interval in case of arrhythmias. Tube voltage ranged from 70 to 120 kV, depending on patient size, as suggested by CarekV (kV optimization assistance). Contrast bolus timing was determined after a test bolus. Iomeprol (Iomeron 350; Bracco Altana Pharma) was injected with dose and flow rate depending on patient characteristics and scan mode. A dual bolus technique was used followed by a saline flush. cCTA images were reconstructed with a slice thickness of 0.6 mm. Post-processing and analysis of cCTA images were performed using dedicated software (Aquarius iNtuition, TeraRecon, Version 4.4.13).
PCATMA measurement
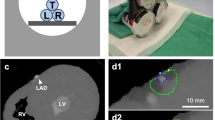
PCATMA was measured in the main coronary arteries (LAD, LCX, and RCA). PCATMA measurements were based on the conceptual framework as proposed by Antonopoulos et al [16]. The workstation automatically reconstructed three-dimensional volume-rendered and curved multi-planar reformat images, which were manually corrected by the radiologist in case of identification errors. The following steps were performed (Fig. 1): (a) Start and end points of the PCATMA measurement were selected. For LAD and RCA, the start point was 10 mm distally from the origin to avoid overlap with the LCX measurement and influence of the aortic wall, respectively. For LCX, the vessel origin was selected as the start point. Because of LCX anatomy, there is limited adipose tissue around the LCX after 10 mm. We adjusted the measurement length to 10 mm for all coronary arteries in order to minimize interference of side branch intersections, which costs less time than the 40 mm in the original study [16]. (b) A 1-mm gap was left around the artery lumen and the measurement circle in order to prevent blooming artifacts from high contrast concentration. (c) The mean HU value of adipose tissue was measured in a concentric circle from 1 to 2 mm around the coronary lumen (1 mm thickness). Compared with prior studies, we reduced measurement width from the average vessel diameter of about 3 to 1 mm in order to avoid interference from the myocardium and veins. (d) The software automatically calculates the mean CT attenuation and volume for voxels within the target threshold of − 190 to – 30 HU [16].

Measurement steps of PCATMA (cCTA at 70 kV in a 56-year-old male patient). (a) Measurement ranges (red rectangles) are marked on the VR image, the 10-mm reference line is the blue line. (b) A gap of 1 mm is determined around the border of the coronary lumen. (c) CT density is measured for a concentric ring from 1 to 2 mm around the coronary lumen (1 mm thickness). (d) The software automatically calculates the mean CT attenuation and volume for voxels within the target threshold of − 190 to – 30 HU. PCATMA is pericoronary adipose tissue mean attenuation; LAD is left anterior descending coronary artery; LCX is left circumflex coronary artery; RCA is right coronary artery; VR is volume rendering; cCTA is coronary computed tomography angiography
EAT measurements
The heart was manually segmented. Within this segmentation, an HU range from − 190 to − 30 was set to select relevant tissue. The volume value of the EAT was automatically obtained by the software.
PCAT measurement methodology variation
In order to evaluate whether measurement length influences PCATMA measurements, PCATMA was measured with 40 mm and 10 mm lengths in 60 randomly selected cCTA scans. In twenty randomly selected cCTAs, intra- and inter-observer agreements were determined. For intra-observer agreement, PCATMA was measured again by the same reader after at least 4 weeks to avoid image recognition. For inter-observer agreement, a second independent reader measured PCATMA after sufficient training.
Statistical methods
The sample size was calculated using paired sample t-testing with GPOWER software (Faul, Erdfelder, Lang, & Buchner, version 3.1.9.2). For sample size calculation, we used results from two prior PCATMA studies [16, 25], with the following parameters: mean and SD of PCATMA (− 75.1 ± 8.6 HU and − 77.0 ± 8.5 HU); correlation between groups 0.5. The effect size was calculated to be 0.2222108. With α = 0.05, power = 0.8, and two-tailed analysis, the needed sample size was 161. We added 20%, yielding a total sample size of 192, to decrease type I and type II error ratios.
Normality testing for continuous variables was performed with the Shapiro-Wilk test. Continuous variables were represented as mean ± SD. Categorical variables were recorded as numbers (n) and frequencies (%). Associations of age, sex, and BMI with PCATMA were tested using multivariable regression analysis. PCATMA values by sex were compared using unpaired sample t-testing. PCATMA comparisons between combinations of two coronary arteries were made using paired sample t-testing; values between three coronary arteries were compared using repeated ANOVA testing. In order to determine the effects of tube voltage on PCATMA, patients were grouped according to tube voltage as follows: 70, 80, 90, 100, 120 kV. For PCATMA and EAT volume comparison of multiple kV groups, one-way ANOVA testing was used. Post hoc pairwise comparisons of PCATMA were performed between each two kV groups. p values < 0.05 were considered statistically significant. For multi-paired t-testing a Bonferroni correction was applied, adjusting the p value accordingly. SPSS (SPSS, version 25; IBM) was used for statistical analysis.
Results
Study population characteristics
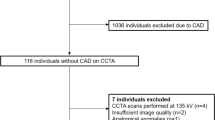
In total, 206 patients without CAD on cCTA images were selected for analysis. Fourteen patients were excluded for various reasons: anomalous origin of coronary artery (n = 6), insufficient image quality (n = 5), incomplete coronary image coverage (n = 1), pacemaker artifact (n = 1), and streak artifact (n = 1) (Fig. 2). The final study population consisted of 192 patients (76 [39.6%] men; mean age 50.5 years [range, 19–79 years]) and 576 coronary arteries. Overall, 72 patients (37.5%) underwent cCTA at 70 kV, 53 (27.6%) at 80 kV, 39 (20.3%) at 90 kV, and 28 (14.6%) at 100 to 120 kV (Table 1).

Flowchart of patient inclusion. CAD is coronary artery disease; cCTA is coronary computed tomography angiography
PCATMA of healthy coronary arteries on cCTA
Overall mean PCATMA value was − 90.3 ± 11.1 HU. Mean PCATMA of men and women was − 88.5 ± 10.5 HU and − 91.5 ± 11.3 HU (p = 0.001), respectively. In multivariable linear regression analysis, kV, age, and gender were significantly associated with PCATMA (p < 0.05) while BMI was not (p = 0.235). Mean PCATMA of LAD, LCX, and RCA was − 92.4 ± 11.6 HU, − 88.4 ± 9.9 HU, and − 90.2 ± 11.4 HU, respectively (p < 0.001). There were significant differences between all combinations of coronary arteries: PCATMA-LAD and PCATMA-LCX (p < 0.001), PCATMA-LAD and PCATMA-RCA (p = 0.009), PCATMA-LCX and PCATMA-RCA (p = 0.033) (Fig. 3).

PCATMA values for the main coronary arteries. PCATMA is pericoronary adipose tissue mean attenuation; LAD is left anterior descending coronary artery; LCX is left circumflex coronary artery; RCA is right coronary artery
Influence of tube voltage on PCATMA
Mean PCATMA showed a positive linear association with tube voltage (Fig. 4). Mean (SD) PCATMA of the 70 kV, 80 kV, 90 kV, 100 kV, and 120 kV groups was − 95.6 ± 9.6 HU, − 90.2 ± 11.5 HU, − 87.3 ± 9.9 HU, − 82.7 ± 6.2 HU, and − 79.3 ± 6.8 HU, respectively (p < 0.001). Post hoc pairwise comparisons of the kV groups demonstrated significant differences between each two groups except for the 80 kV and 90 kV (p = 0.222), and 100 kV and 120 kV groups (p = 0.267).

PCATMA values in patient groups based on cCTA tube voltage setting. PCATMA is pericoronary adipose tissue mean attenuation; kV is kilovoltage; HU is Hounsfield Units; cCTA is coronary computed tomography angiography
Tube voltage and EAT volume
Mean EAT volume showed a positive linear association with tube voltage (Fig. 5). Mean (SD) EAT volume of the 70 kV, 80 kV, 90 kV, 100 kV, and 120 kV groups was 107.6 ± 49.7 cm3, 145.5 ± 60.1 cm3, 172.8 ± 63.6 cm3, 183.7 ± 63.2 cm3, and 199.5 ± 78.1 cm3, respectively (p < 0.001).

EAT volume in patient groups based on cCTA tube voltage setting. EAT is epicardial adipose tissue; kV is kilovoltage; CM is centimeter; cCTA is coronary computed tomography angiography
PCAT measurement methodology variation
PCATMA of LAD, LCX, and RCA for 40-mm measurement length was − 95.6 ± 9.7 HU, − 88.7 ± 10.0 HU, and − 92.9 ± 8.3 HU, respectively, compared with − 94.5 ± 11.0 HU, − 90.0 ± 8.7 HU, and − 91.6 ± 9.7 HU for 10-mm measurement length (p = 0.124, 0.118, 0.116, respectively) (Supplementary Material Table S1 and Fig. S1). There was excellent correlation within and between readers for repeated PCATMA measurements (0.974–0.982), with minimal bias but with some variability between readings (upper and lower limits of agreement 3.9 HU and − 3.3 HU within-reader, 4.6 HU, and − 4.1 HU between-readers) (Supplementary Material Table S2 and Fig. S2).
Discussion
In this study, we investigated the PCATMA values of healthy coronary arteries and the influence of tube voltage. Our main results showed that the tube voltage of cCTA significantly influenced PCATMA values in patients without CAD, and that PCATMA differed slightly between the LAD, LCX, and RCA.
Although the presence of obstructive disease on cCTA is associated with worse outcomes, many myocardial infarctions originate from coronary segments without prior obstructive disease. Thus, the focus has shifted to the identification of segments at future risk of developing potentially vulnerable plaque [26]. Studies on PCATMA in diseased populations showed significant differences between diseased and non-diseased coronary arteries, and between flow-limiting and non-flow limiting stenosis [24]. Although results were statistically significant, these studies show, similar to the current study, limited absolute differences in PCAT values (± 5 HU). However, these studies show an increased accuracy for the prediction of hemodynamic significance of a lesion, especially in combination with other factors such as stenosis diameter. Further understanding of the PCAT parameter and the influence of scan protocol settings on this biomarker and its variability can help to determine limits of reliability around PCATMA values when comparing patients.
One of the main results of this study is that the use of different kV levels has considerable impact on PCATMA values. In clinical practice, cCTA acquisitions are acquired with varying kV levels. Higher kV voltages will inherently lead to higher PCATMA and EAT attenuation, unrelated to a pathophysiological process. Prior studies investigating the use of PCATMA used cCTA images obtained at 100 kV and/or 120 kV [16, 20, 21, 25]. However, lower kV acquisitions are becoming increasingly popular in order to reduce radiation and contrast medium volume. Recent results from the PROTECTION VI Study showed that low kV settings for cCTA (< 100 kV) are already applied in 14% of patients and this is only expected to increase [27, 28]. Our results showed significant differences between all kV levels except between 80 and 90 kV, and between 100 and 120 kV. The lack of difference in PCATMA between 100 and 120 kV is also reflected by the similar PCATMA results from previous studies investigating only those two levels. The differences in PCATMA between the other kV levels indicate that a kV-specific PCATMA cutoff should be used to discriminate healthy from diseased patients and perform accurate risk assessment. Determination of this cutoff fell outside the scope of this research. The current study provides reference values of PCATMA by kV setting in normal coronary arteries; future studies should investigate the PCATMA by kV in coronary arteries with plaque and/or stenosis, and evaluate the optimal cutoff values. To construct a kV correction factor, ideally the same patients would have to undergo repeated cCTA at different kV levels. The results also showed a positive relation between kV and EAT volume. This is likely mostly due to the fact that patients with higher BMI (and more intrathoracic fat) were usually scanned with higher kV to get better image quality. In view of the influence of kV on PCATMA analysis, it is recommended that for the longitudinal follow-up and comparison of cCTA-based PCATMA values, the cCTA is performed at equal tube voltage setting.
The majority of PCATMA studies about relationship with CAD focused on analysis of the RCA alone, while the LAD and LCX could provide additional information and increase the accuracy of outcome prediction [16, 21]. Our study focused on PCATMA measurements in all three coronary arteries, showing that PCATMA was slightly but significantly different between the LAD, LCX, and RCA. This difference could be caused by differences in anatomy and surrounding tissues, indicating that PCATMA values and corresponding cutoff values based on RCA measurements cannot be directly transferred to the other coronary arteries. Our study results showed that LAD had slightly but significantly lower PCATMA compared with the RCA and LCX. As is known in literature, atherosclerosis development also differs between the coronary arteries. The LAD is subject to atherosclerosis more often and at an earlier stage in comparison with RCA and LCX [29,30,31]. The fact that LAD had a lower PCATMA is an important hypothesis-generating finding. This finding suggests that PCATMA could be related to vessel vulnerability for atherosclerosis. This hypothesis should be further investigated in pathophysiological and prospective clinical studies.
To analyze all three coronary arteries, an adjusted measurement method was used in our study. Previously, a measurement length of 40 mm was used [16, 21, 25] which was feasible for the RCA because it has fewer side branches and proximal variations than the LAD and LCX. To avoid influence of side branches, measurement length was reduced from 40 to 10 mm in this study. Results from our sub-study demonstrated no differences in PCATMA between our 10-mm methods and 40-mm method. PCATMA measurement width around the coronary could potentially affect measurement accuracy. Prior studies measured PCATMA using approximately 3 mm thickness (or equal to vessel diameter) around the coronary vessels [16, 20, 21, 25]. However, contrast enhancement of the lumen has been found to influence the HU values in the voxels adjacent to the luminal border [32]. To take this into account, we applied a 1-mm gap around the vessel wall. Thus, our study measured PCATMA using a more constrictive measurement width, making it more suitable for LAD and LCX measurements, and potentially more sensitive to inflammatory changes. Manual PCAT measurements using the method described here can be performed in a similar time span compared with manual EAT measurements. Fully automated software, as mentioned by some researchers [21], allows for PCATMA evaluation within 30 s, increasing the time efficiency of PCATMA analysis and enabling use in clinical practice.
While PCATMA and EAT both are measures of adipose tissue, they represent different processes [16]. PCATMA quantifies fat at the per-vessel level or per-lesion level as an indicator of coronary inflammation, while EAT provides a measure of the volume of the entire epicardial fat system as a marker for paracrine effects of fat. Thus, PCATMA may provide a more specific, focal assessment of coronary risk and vulnerability. PCATMA was shown to have additional diagnostic value with more precision and specificity compared with EAT measurements [33]. Studies found that PCATMA and FFR were related at the per-vessel level [20] and that PCATMA of RCA was able to assist in risk stratification of cardiovascular mortality [25]. The combined use of PCATMA, total plaque volume, and diameter stenosis has shown high diagnostic accuracy for prediction of hemodynamically significant coronary stenosis [24]. Interestingly, Goeller et al [21] found that changes in attenuation of adipose tissue in the pericoronary space were related to changes in plaque burden. These results suggest that these effects are associated with changes in PCAT specifically rather than adipose tissue in general.
Besides differences between kV levels and coronary arteries, our results show a slight but important difference in PCATMA between men and women that could not be explained by differences in kV distribution. Men are known to get CAD more frequently than women and at an earlier age [31]. The PCATMA difference between men and women follows the same trend. This finding deserves further exploration in a study with comprehensive cardiovascular risk factor assessment and more diverse range of coronary atherosclerosis. Sex-related differences in PCATMA could be caused by several factors. Men have a higher amount of EAT than women [34, 35], related to cardiovascular risk. There are sex-related differences in the regulation mechanism of pericardial adipokines [36] and in the physiological mechanism of adipose tissue [37]. Additionally, it could be that differences in sex-related hormones, higher low-density lipoprotein in male patients, and differences in risk factors impact PCATMA in men and women [38].
Limitations
This was a single-center retrospective study of patients with a clinical indication for cCTA. There was no follow-up, since a normal cCTA result led to discharge from the cardiology outpatient clinic. Some of the patients might have been at higher risk to develop CAD, reflected in already altered PCATMA values while there was no plaque development yet. There could be factors other than tube voltage affecting PCATMA measurements such as obesity or diabetes, inflammatory processes, or specific medication. Further work is needed to explore all potentially influencing factors. With regard to the measurement itself, the anatomical variation of LCX compared with LAD and RCA was relatively large and could have affected the PCATMA measurement. However, with our adjusted measurement protocol, we found excellent correlation between repeated measurements within and between readers with limited bias, indicating the validity of the PCATMA measurement.
Conclusion
In conclusion, our results showed that PCATMA varied considerably by tube voltage in patients without plaque on cCTA, with minor differences in PCATMA between coronary arteries (LAD, LCX, RCA). cCTA kV setting needs to be taken into account when interpreting PCATMA values.
Abbreviations
- BMI:
-
Body mass index
- CAD:
-
Coronary artery disease
- cCTA:
-
Coronary computed tomography angiography
- EAT:
-
Epicardial adipose tissue
- ECG:
-
Electrocardiography
- kV:
-
Kilovoltage
- LAD:
-
Left anterior descending coronary artery
- LCX:
-
Left circumflex coronary artery
- PCATMA :
-
Pericoronary adipose tissue mean attenuation
- RCA:
-
Right coronary artery
- SD:
-
Standard deviation
References
Stoll G, Bendszus M (2006) Inflammation and atherosclerosis: novel insights into plaque formation and destabilization. Stroke 37:1923–1932
Hansson GK (2005) Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med 352:1685–1695
Libby P, Tabas I, Fredman G, Fisher EA (2014) Inflammation and its resolution as determinants of acute coronary syndromes. Circ Res 114:1867–1879
Choi BJ, Matsuo Y, Aoki T et al (2014) Coronary endothelial dysfunction is associated with inflammation and vasa vasorum proliferation in patients with early atherosclerosis. Arterioscler Thromb Vasc Biol 34:2473–2477
Ridker PM, Libby P, MacFadyen JG et al (2018) Modulation of the interleukin-6 signalling pathway and incidence rates of atherosclerotic events and all-cause mortality: analyses from the Canakinumab Anti-Inflammatory Thrombosis Outcomes Study (CANTOS). Eur Heart J 39:3499–3507
Ridker PM, Everett BM, Thuren T et al (2017) Antiinflammatory therapy with canakinumab for atherosclerotic disease. N Engl J Med 377:1119–1131
Nosalski R, Guzik TJ (2017) Perivascular adipose tissue inflammation in vascular disease. Br J Pharmacol 174:3496–3513
Mancio J, Oikonomou EK, Antoniades C (2018) Perivascular adipose tissue and coronary atherosclerosis. Heart 104:1654–1662
Tanaka K, Sata M (2018) Roles of perivascular adipose tissue in the pathogenesis of atherosclerosis. Front Physiol 9:3
Ohyama K, Matsumoto Y, Takanami K et al (2018) Coronary adventitial and perivascular adipose tissue inflammation in patients with vasospastic angina. J Am Coll Cardiol 71:414–425
Mazurek T, Zhang L, Zalewski A et al (2003) Human epicardial adipose tissue is a source of inflammatory mediators. Circulation 108:2460–2466
Goeller M, Achenbach S, Marwan M et al (2018) Epicardial adipose tissue density and volume are related to subclinical atherosclerosis, inflammation and major adverse cardiac events in asymptomatic subjects. J Cardiovasc Comput Tomogr 12:67–73
Lu MT, Park J, Ghemigian K et al (2016) Epicardial and paracardial adipose tissue volume and attenuation - association with high-risk coronary plaque on computed tomographic angiography in the ROMICAT II trial. Atherosclerosis 251:47–54
Nagayama Y, Nakamura N, Itatani R et al (2019) Epicardial fat volume measured on nongated chest CT is a predictor of coronary artery disease. Eur Radiol 29:3638–3646
Bos D, Leening MJG (2018) Leveraging the coronary calcium scan beyond the coronary calcium score. Eur Radiol 28:3082–3087
Antonopoulos AS, Sanna F, Sabharwal N et al (2017) Detecting human coronary inflammation by imaging perivascular fat. Sci Transl Med 9:eaal2658
Lian X, Gollasch M (2016) A clinical perspective: contribution of dysfunctional perivascular adipose tissue (PVAT) to cardiovascular risk. Curr Hypertens Rep 18:82
Margaritis M, Antonopoulos AS, Digby J et al (2013) Interactions between vascular wall and perivascular adipose tissue reveal novel roles for adiponectin in the regulation of endothelial nitric oxide synthase function in human vessels. Circulation 127:2209–2221
Antoniades C, Antonopoulos AS, Tousoulis D, Stefanadis C (2009) Adiponectin: from obesity to cardiovascular disease. Obes Rev 10:269–279
Goeller M, Achenbach S, Cadet S et al (2018) Pericoronary adipose tissue computed tomography attenuation and high-risk plaque characteristics in acute coronary syndrome compared with stable coronary artery disease. JAMA Cardiol 3:858–863
Goeller M, Tamarappoo BK, Kwan AC et al (2019) Relationship between changes in pericoronary adipose tissue attenuation and coronary plaque burden quantified from coronary computed tomography angiography. Eur Heart J Cardiovasc Imaging 20:636–643
Kwiecinski J, Dey D, Cadet S et al (2019) Peri-coronary adipose tissue density is associated with (18)F-sodium fluoride coronary uptake in stable patients with high-risk plaques. JACC Cardiovasc Imaging 12:2000–2010
Gaibazzi N, Martini C, Botti A, Pinazzi A, Bottazzi B, Palumbo AA (2019) Coronary inflammation by computed tomography pericoronary fat attenuation in MINOCA and Tako-Tsubo syndrome. J Am Heart Assoc 8:e013235
Yu M, Dai X, Deng J, Lu Z, Shen C, Zhang J (2020) Diagnostic performance of perivascular fat attenuation index to predict hemodynamic significance of coronary stenosis: a preliminary coronary computed tomography angiography study. Eur Radiol 30:673–681
Oikonomou EK, Marwan M, Desai MY et al (2018) Non-invasive detection of coronary inflammation using computed tomography and prediction of residual cardiovascular risk (the CRISP CT study): a post-hoc analysis of prospective outcome data. Lancet 392:929–939
Maddox TM, Stanislawski MA, Grunwald GK et al (2014) Nonobstructive coronary artery disease and risk of myocardial infarction. JAMA 312:1754–1763
Stocker TJ, Deseive S, Leipsic J et al (2018) Reduction in radiation exposure in cardiovascular computed tomography imaging: results from the PROspective multicenter registry on radiaTion dose Estimates of cardiac CT angIOgraphy iN daily practice in 2017 (PROTECTION VI). Eur Heart J 39:3715–3723
Stocker TJ, Leipsic J, Hadamitzky M et al (2020) Application of low tube potentials in CCTA: results from the PROTECTION VI study. JACC Cardiovasc Imaging 13:425–434
Alluri K, McEvoy JW, Dardari ZA et al (2015) Distribution and burden of newly detected coronary artery calcium: results from the multi-ethnic study of atherosclerosis. J Cardiovasc Comput Tomogr 9:337–344 e331
Wykrzykowska JJ, Mintz GS, Garcia-Garcia HM et al (2012) Longitudinal distribution of plaque burden and necrotic core-rich plaques in noncuprit lesions of patients presenting with acute coronary syndromes. JACC Cardiovasc Imaging 5:S10–S18
Schulman-Marcus J, Hartaigh B, Gransar H et al (2016) Sex-specific associations between coronary artery plaque extent and risk of major adverse cardiovascular events: the CONFIRM long-term registry. JACC Cardiovasc Imaging 9:364–372
Kristanto W, Tuncay V, Vliegenthart R, van Ooijen PM, Oudkerk M (2015) Correction of lumen contrast-enhancement influence on non-calcified coronary atherosclerotic plaque quantification on CT. Int J Cardiovasc Imaging 31:429–436
Maurovich-Horvat P, Kallianos K, Engel LC et al (2015) Relationship of thoracic fat depots with coronary atherosclerosis and circulating inflammatory biomarkers. Obesity (Silver Spring) 23:1178–1184
Gill CM, Azevedo DC, Oliveira AL, Martinez-Salazar EL, Torriani M, Bredella MA (2018) Sex differences in pericardial adipose tissue assessed by PET/CT and association with cardiometabolic risk. Acta Radiol 59:1203–1209
Mancio J, Pinheiro M, Ferreira W et al (2017) Gender differences in the association of epicardial adipose tissue and coronary artery calcification: EPICHEART study: EAT and coronary calcification by gender. Int J Cardiol 249:419–425
Fei J, Cook C, Blough E, Santanam N (2010) Age and sex mediated changes in epicardial fat adipokines. Atherosclerosis 212:488–494
Chang E, Varghese M, Singer K (2018) Gender and sex differences in adipose tissue. Curr Diab Rep 18:69
Arnold AP, Cassis LA, Eghbali M, Reue K, Sandberg K (2017) Sex hormones and sex chromosomes cause sex differences in the development of cardiovascular diseases. Arterioscler Thromb Vasc Biol 37:746–756
Acknowledgements
We thank Dr. Estelle Noach for critical reading of the manuscript and Mrs. Amanda Boone for technical support of the Aquarius software. The UMCG is supported by an institutional research grant from Siemens Healthineers. We are grateful to Dr. Mieneke Rook for the scientific advice at the beginning of this study.
Funding
Financial support provided by the China Scholarship Council (CSC) for the PhD project of the first author is gratefully acknowledged.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Guarantor
The scientific guarantor of this publication is Rozemarijn Vliegenthart.
Conflict of interest
The UMCG is supported by an institutional research grant from Siemens Healthineers. The authors of this manuscript declare no other relationships with any companies whose products or services may be related to the subject matter of the article.
Statistics and biometry
One of the authors has significant statistical expertise.
Informed consent
Written informed consent was waived by the Institutional Review Board.
Ethical approval
Institutional Review Board approval was obtained.
Methodology
• retrospective
• cross-sectional study
• performed at one institution
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 374 kb)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ma, R., Ties, D., van Assen, M. et al. Towards reference values of pericoronary adipose tissue attenuation: impact of coronary artery and tube voltage in coronary computed tomography angiography. Eur Radiol 30, 6838–6846 (2020). https://doi.org/10.1007/s00330-020-07069-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-020-07069-0