
Abstract
Purpose
To determine the correlation of pre-procedural and imaging characteristics with lung shunt fraction (LSF) measured by technetium-99 m macroaggregated albumin (99mTc-MAA) scan in patients with hepatocellular carcinoma.
Methods
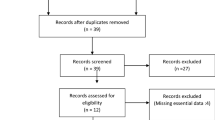
A retrospective study was conducted of 428 subjects with hepatocellular carcinoma from 2004 to 2011 assessed for lung shunting by 99mTc-MAA scan. Baseline characteristics included age, gender, ethnicity, tumor burden, maximum dimension, number of lesions, presence of extrahepatic metastases, macrovascular (hepatic and portal vein) invasion, ascites on imaging, laboratory values, and alpha-fetoprotein (AFP). Univariate and multivariate logistic regression analysis was performed. Receiver operating characteristic curves were used to obtain sensitivity (SN), specificity (SP), and positive likelihood ratios (LR+) of characteristics for low LSF (LSF <10%) and high LSF (LSF >20%).
Results
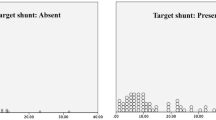
Statistically significant (p < 0.05) independent indicators of low LSF included bilirubin <1.45 mg/dL (SN = 49.5%, SP = 69.1%, LR+ = 1.60), maximum tumor size <7.15 cm (SN = 66.0%, SP = 75.9%, LR+ = 2.74), AFP ≤200 ng/mL (SN = 64.6%, SP = 65.0%, LR+ = 1.85), and absent macrovascular invasion (SN = 73.9%, SP = 64.9%, LR+ = 2.11). Independent indicators of high LSF included albumin <2.65 g/dL (SN = 64.3%, SP = 64.1%, LR+ = 1.79) and macrovascular invasion (SN = 74.4%, SP = 67.4%, LR+ = 2.28). A combined risk factor model was constructed. If there is no macrovascular invasion: \({\text{LSF }} = {\text{ e}}^{ - 3.846} \times ({\text{Bilirubin}})^{0.303} \times {\text{AFP}}^{0.056} \times ({\text{Maximum dimension}})^{0.364}\). With macrovascular invasion, \({\text{LSF }} = {\text{ e}}^{ - 3.629} \times ({\text{Bilirubin}})^{0.303} \times {\text{AFP}}^{0.056} \times ({\text{Maximum dimension}})^{0.364}\) (R 2 = 0.257). Since these factors all have LR+ between 2 and 5, they only reflect slight increase in LSF predictivity.
Conclusion
Serum AFP, albumin, bilirubin, and portal/hepatic vein invasion on cross-sectional imaging are statistically significant but weak clinical indicators of LSF, as shown by low SN, SP, and LR+ for clinically relevant cutoff LSF values. Thus, these factors cannot be relied upon in clinical practice.


Similar content being viewed by others
Abbreviations
- 99mTc:
-
Technetium-99 m
- 99mTc-MAA:
-
Technetium-99m macroaggregated albumin
- 90Y:
-
Yttrium-90
- AFP:
-
Alpha-fetoprotein
- BCLC:
-
Barcelona Clinic Liver Cancer
- ECOG:
-
Eastern Cooperative Oncology Group
- HBV:
-
Hepatitis B virus
- HCC:
-
Hepatocellular carcinoma
- HCV:
-
Hepatitis C virus
- LR+ :
-
Positive likelihood ratio
- LSF:
-
Lung shunt fraction
- MAA:
-
Macroaggregated albumin
- NASH:
-
Nonalcoholic steatohepatitis
- PVT:
-
Portal vein thrombosis
- ROC:
-
Receiver operating characteristic
- SN:
-
Sensitivity
- SP:
-
Specificity
References
Salem R, Lewandowski RJ, Sato KT, Atassi B, Ryu RK, Ibrahim S, et al. Technical aspects of radioembolization with 90Y microspheres. Tech Vasc Interv Radiol. 2007;10(1):12–29.
Salem R, Parikh P, Atassi B, Lewandowski RJ, Ryu RK, Sato KT, et al. Incidence of radiation pneumonitis after hepatic intra-arterial radiotherapy with yttrium-90 microspheres assuming uniform lung distribution. Am J Clin Oncol. 2008;31(5):431–8.
Gaba RC, Zivin SP, Dikopf MS, Parvinian A, Casadaban LC, Lu Y, et al. Characteristics of primary and secondary hepatic malignancies associated with hepatopulmonary shunting. Radiology. 2014;271(2):602–12.
SIRS-Spheres Yttrium-90 microspheres package insert. Singapore Science Park SSM.
Lewandowski RJ, Salem R. Yttrium-90 radioembolization of hepatocellular carcinoma and metastatic disease to the liver. In: Seminars in interventional radiology. 2006;23(1):64–72.
Sandow T, DeVun D, Gulotta P, Bohorquez H, Kirsch D. Elevated lung shunt fraction as a prognostic indicator for disease progression and metastasis in hepatocellular carcinoma. JVIR J Vasc Interv Radiol. 2016;S1051–0443(16):00135.
Ludwig JM, Ambinder EM, Ghodadra A, Xing M, Prajapati HJ, Kim HS. Lung shunt fraction prior to yttrium-90 radioembolization predicts survival in patients with neuroendocrine liver metastases: single-center prospective analysis. Cardiovasc Intervent Radiol. 2016;39(7):1007–14.
Xing M, Lahti S, Kokabi N, Schuster DM, Camacho JC, Kim HS. 90Y radioembolization lung shunt fraction in primary and metastatic liver cancer as a biomarker for survival. Clin Nucl Med. 2016;41(1):21–7.
Gates VL, Marshall KG, Salzig K, Williams M, Lewandowski RJ, Salem R. Outpatient single-session yttrium-90 glass microsphere radioembolization. JVIR J Vasc Interv Radiol. 2014;25(2):266–70.
Gabr A, Kallini JR, Gates V, Hickey R, Kulik L, Desai K, et al. Same-day Y90 radioembolization: implementing a new treatment paradigm. Eur J Nucl Med Mol Imaging. 2016;43(13):2353–9.
Ward TJ, Tamrazi A, Lam MG, Louie JD, Kao PN, Shah RP, et al. Management of high hepatopulmonary shunting in patients undergoing hepatic radioembolization. JVIR J Vasc Interv Radiol. 2015;26(12):1751–60.
Theysohn JM, Schlaak JF, Muller S, Ertle J, Schlosser TW, Bockisch A, et al. Selective internal radiation therapy of hepatocellular carcinoma: potential hepatopulmonary shunt reduction after sorafenib administration. JVIR J Vasc Interv Radiol. 2012;23(7):949–52.
Rose SC, Hoh CK. Hepatopulmonary shunt reduction using chemoembolization to permit yttrium-90 radioembolization. JVIR J Vasc Interv Radiol. 2009;20(6):849–51.
Kwok N, Irani Z, Sheth R, Arellano RS. Hepatopulmonary shunt reduction with bland embolization for yttrium-90 radioembolization. Diagn Interv Imaging. 2016;97(3):369–70.
Gaba RC, Vanmiddlesworth KA. Chemoembolic hepatopulmonary shunt reduction to allow safe yttrium-90 radioembolization lobectomy of hepatocellular carcinoma. Cardiovasc Intervent Radiol. 2012;35(6):1505–11.
Kallini JR, Gabr A, Kulik L, Salem R, Lewandowski RJ. The utility of unilobar technetium-99m macroaggregated albumin to predict pulmonary toxicity in bilobar HCC prior to yttrium-90 radioembolization. JVIR J Vasc Interv Radiol. 2016;27(9):1453.
Olorunsola OG, Kohi MP, Behr SC, Kolli PK, Taylor AG, Tong RT, et al. Imaging predictors of elevated lung shunt fraction in patients being considered for yttrium-90 radioembolization. JVIR J Vasc Interv Radiol. 2015;26(10):1472–8.
Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS, Rubinstein L, et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst. 2000;92(3):205–16.
Yerubandi V, Ronald J, Howard BA, Suhocki PV, James OG, Wong TZ, et al. Patient and tumor characteristics predictive of an elevated hepatopulmonary shunt fraction before radioembolization of hepatic tumors. Nucl Med Commun. 2016;37(9):939–46.
McGee S. Simplifying likelihood ratios. J Gen Intern Med. 2002;17(8):646–9.
Ahmadzadehfar H, Duan H, Haug AR, Walrand S, Hoffmann M. The role of SPECT/CT in radioembolization of liver tumours. Eur J Nucl Med Mol Imaging. 2014;41(Suppl 1):S115–24.
Acknowledgements
We would like to acknowledge the efforts of Karen Marshall, Krystina Salzig, and Melissa J. Williams in data collection.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
RJL, RS, and LK are advisors to BTG. LK is an advisor to Bayer/Onyx.
Rights and permissions
About this article

Cite this article
Kallini, J.R., Gabr, A., Hickey, R. et al. Indicators of Lung Shunt Fraction Determined by Technetium-99 m Macroaggregated Albumin in Patients with Hepatocellular Carcinoma. Cardiovasc Intervent Radiol 40, 1213–1222 (2017). https://doi.org/10.1007/s00270-017-1619-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-017-1619-z