
Abstract
Introduction
Malunion is a well-recognized complication of long-bone fractures which accounts for more than 25% of injuries in conflict zones. The aim of this study was to investigate the rate of malunion sustained by casualties with penetrating gunshot wounds in an International Committee of the Red Cross (ICRC) surgical substitution project in the Democratic Republic of Congo (DRC) and compare these results with current literature.
Methods
A retrospective cohort study was performed. All patients admitted to the ICRC facility between the periods of 01.10.2014 and 31.12.2015 with long-bone fractures caused by gunshot wound were included, and data were collected retrospectively from the patient’s hospital notes.
Results
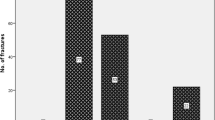
A total of 191 fractures caused by gunshot were treated in the DRC at the ICRC surgical substitution project during the study period. On average, the fractures were 3 days old on admission and were all open, with 62% also being comminuted. The ICRC management protocol, which emphasizes debridement, antibiotic prophylaxis and conservative fracture stabilization, was followed in all cases. Forty-eight percentage of the fractures were finally classified as ‘union without complication’; however, 17% were classified as ‘malunion’.
Conclusions
This study indicates that open long-bone fractures that are managed by the ICRC surgical substitution project in DRC may have an increased likelihood of malunion as compared to long-bone fractures treated in developed countries. Patient delay and mechanism of injury may have caused increased rates of infection which are likely behind these increased rates of malunion, alongside the lack of definitive fracture treatment options made available to the surgical team.





Similar content being viewed by others


References
Giannou C, Baldan M (2009) War surgery: working with limited resources in armed conflict and other situations of violence, vol 1. International Committee of the Red Cross, Geneva
Champion HR, Bellamy RF, Roberts P et al (2003) A profile of combat injury. J Trauma 54(5 suppl):S13–S19
Versier G, Le Marec C, Le Rou J (1998) Quatre ans de chirurgie de guerre au GMC de Sarajevo (juillet 1992 à août 1996). Médecine et armées 26:213–218
Tziopis C, Giannoudis PV (2007) Prevalence of long-bone non-unions. Injury 38:3–9
Nandra R, Grover L, Porter K (2016) Fracture non-union epidemiology and treatment. Trauma 18(1):3–11
Persad IJ, Reddy RS, Saunders MA et al (2005) Gunshot injuries to the extremities: experience of a UK trauma centre. Injury 36(3):407–411
Nicholas RM, McCoy GF (1995) Immediate intramedullary nailing of femoral shaft fractures due to gunshots. Injury 26(4):257–259
Perkins C, Scannell B, Brighton B et al (2016) Orthopaedic firearm injuries in children and adolescents: an eight-year experience at a major urban trauma center. Injury 47(1):173–177
Arslan H, Subasi M, Kesemenli C et al (2002) Problem fractures associated with gunshot wounds in children. Injury 33(9):743–749
Ali MA, Hussain SA, Khan MS (2008) Evaluation of results of interlocking nails in femur fractures due to high velocity gunshot injuries. J Ayub Med Coll Abbottabad 20(1):16–19
Hoencamp R, Idenburg FJ, Hamming JF et al (2014) Incidence and epidemiology of casualties treated from August 2006 to August 2010 at the Dutch role 2E at multi national base Tarin Kowt Afghanistan. World J Surg 39(10):2413–2421. doi:10.1007/s00268-014-2462-x
Hoencamp R, Tan ECTH, Idenburg FJ et al (2014) Challenges in training of military surgeons: experiences from Dutch combat operations in Southern Afghanistan. Eur J Trauma Emerg Surg 40(4):421–428
International Committee of the Red Cross (2016). www.icrc.org. Accessed 07 Dec 2016
Giannou C, Baldan M, Molde A (2013) War surgery: working with limited resources in armed conflict and other situations of violence, vol 2. International Committee of the Red Cross, Geneva
U.S. Food and Drug Administration (1986). http://www.fda.gov. Accessed 07 Dec 2016
Mills LA, Simpson AH (2013) The relative incidence of fracture non-union in the Scottish population (5.7 million): a 5-year study. BMJ Open 3(2):1–8
Calori GM, ALbisetti W, Agus A et al (2007) Risk factors contributing to fracture non-union. Injury Int J Care Injured 38:11–18
Mody R, Sapor M, Hartzell JD et al (2009) Infectious complications of damage control orthopaedics in war trauma. J Trauma 67:758–761
Moughrabieh A, Weinert C (2016) Rapid deployment of international Tele-Intensive Care Unit Services in war-torn Syria. Ann Am Thorac Soc 13(2):165–172
Zheng X, Rodríguez-Monroy C (2015) The development of intelligent healthcare in China. Telemed J E Health 21(5):443–448
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Bauhahn, G., Veen, H., Hoencamp, R. et al. Malunion of Long-Bone Fractures in a Conflict Zone in the Democratic Republic of Congo. World J Surg 41, 2200–2206 (2017). https://doi.org/10.1007/s00268-017-4008-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-017-4008-5