
Abstract
Background
For patients with acute cholecystitis managed with percutaneous cholecystostomy (PC), the optimal duration of post-procedural antibiotic therapy is unknown. Our objective was to compare short versus long courses of antibiotics with the hypothesis that patients with persistent signs of systemic inflammation 72 h following PC would receive prolonged antibiotic therapy and that antibiotic duration would not affect outcomes.
Methods
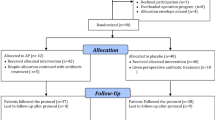
We performed a retrospective cohort analysis of 81 patients who underwent PC for acute cholecystitis at two hospitals during a 41-month period ending November 2014. Patients who received short (≤7 day) courses of post-procedural antibiotics were compared to patients who received long (>7 day) courses. Treatment response to PC was evaluated by systemic inflammatory response syndrome (SIRS) criteria. Logistic and linear regressions were used to evaluate associations between antibiotic duration and outcomes.
Results
Patients who received short (n = 30) and long courses (n = 51) of antibiotics had similar age, comorbidities, severity of cholecystitis, pre-procedural vital signs, treatment response, and culture results. There were no differences in recurrent cholecystitis (13 vs. 12%), requirement for open/converted to open cholecystectomy (23 vs. 22%), or 1-year mortality (20 vs. 18%). On logistic and linear regressions, antibiotic duration as a continuous variable was not predictive of any salient outcomes.
Conclusions
Patients who received short and long courses of post-PC antibiotics had similar baseline characteristics and outcomes. Antibiotic duration did not predict recurrent cholecystitis, interval open cholecystectomy, or mortality. These findings suggest that antibiotics may be safely discontinued within one week of uncomplicated PC.
Similar content being viewed by others


References
Lau WY, Yuen WK, Chu KW et al (1990) Systemic antibiotic regimens for acute cholecystitis treated by early cholecystectomy. Aust N Z J Surg 60(7):539–543
Regimbeau JM, Fuks D, Pautrat K et al (2014) Effect of postoperative antibiotic administration on postoperative infection following cholecystectomy for acute calculous cholecystitis: a randomized clinical trial. JAMA 312(2):145–154
Solomkin JS, Mazuski JE, Bradley JS et al (2010) Diagnosis and management of complicated intra-abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Clin Infect Dis 50(2):133–164
Venara A, Carretier V, Lebigot J et al (2014) Technique and indications of percutaneous cholecystostomy in the management of cholecystitis in 2014. J Visc Surg 151(6):435–439
Merriam LT, Kanaan SA, Dawes LG et al (1999) Gangrenous cholecystitis: analysis of risk factors and experience with laparoscopic cholecystectomy. Surgery 126(4):680–685 discussion 685–686
Winbladh A, Gullstrand P, Svanvik J et al (2009) Systematic review of cholecystostomy as a treatment option in acute cholecystitis. HPB (Oxford) 11(3):183–193
Mcgowan JE (1983) Antimicrobial resistance in hospital organisms and its relation to antibiotic use. Rev Infect Dis 5(6):1033–1048
Arnold HM, Micek ST, Skrupky LP et al (2011) Antibiotic stewardship in the intensive care unit. Semin Respir Crit Care Med 32(2):215–227
de Man P, Verhoeven BA, Verbrugh HA et al (2000) An antibiotic policy to prevent emergence of resistant bacilli. Lancet 355(9208):973–978
Feazel LM, Malhotra A, Perencevich EN et al (2014) Effect of antibiotic stewardship programmes on Clostridium difficile incidence: a systematic review and meta-analysis. J Antimicrob Chemother 69(7):1748–1754
Dik JW, Vemer P, Friedrich AW et al (2015) Financial evaluations of antibiotic stewardship programs-a systematic review. Front Microbiol 6:317
Geissler A, Gerbeaux P, Granier I et al (2003) Rational use of antibiotics in the intensive care unit: impact on microbial resistance and costs. Intensive Care Med 29(1):49–54
Yokoe M, Takada T, Strasberg SM et al (2012) New diagnostic criteria and severity assessment of acute cholecystitis in revised Tokyo Guidelines. J Hepatobiliary Pancreat Sci 19(5):578–585
Saad WE, Wallace MJ, Wojak JC et al (2010) Quality improvement guidelines for percutaneous transhepatic cholangiography, biliary drainage, and percutaneous cholecystostomy. J Vasc Interv Radiol 21(6):789–795
Davies MG, Hagen PO (1997) Systemic inflammatory response syndrome. Br J Surg 84(7):920–935
Welschbillig-Meunier K, Pessaux P, Lebigot J et al (2005) Percutaneous cholecystostomy for high-risk patients with acute cholecystitis. Surg Endosc 19(9):1256–1259
Spira RM, Nissan A, Zamir O et al (2002) Percutaneous transhepatic cholecystostomy and delayed laparoscopic cholecystectomy in critically ill patients with acute calculus cholecystitis. Am J Surg 183(1):62–66
Chopra S, Dodd GD 3rd, Mumbower AL et al (2001) Treatment of acute cholecystitis in non-critically ill patients at high surgical risk: comparison of clinical outcomes after gallbladder aspiration and after percutaneous cholecystostomy. AJR Am J Roentgenol 176(4):1025–1031
Berber E, Engle KL, String A et al (2000) Selective use of tube cholecystostomy with interval laparoscopic cholecystectomy in acute cholecystitis. Arch Surg 135(3):341–346
Darkahi B, Sandblom G, Liljeholm H et al (2014) Biliary microflora in patients undergoing cholecystectomy. Surg Infect (Larchmt) 15(3):262–265
Galili O, Eldar S Jr, Matter I et al (2008) The effect of bactibilia on the course and outcome of laparoscopic cholecystectomy. Eur J Clin Microbiol Infect Dis 27(9):797–803
Thompson JE Jr, Bennion RS, Doty JE et al (1990) Predictive factors for bactibilia in acute cholecystitis. Arch Surg 125(2):261–264
Skillings JC, Kumai C, Hinshaw JR (1980) Cholecystostomy: A place in modern biliary surgery? Am J Surg 139(6):865–869
McKay A, Abulfaraj M, Lipschitz J (2012) Short- and long-term outcomes following percutaneous cholecystostomy for acute cholecystitis in high-risk patients. Surg Endosc 26(5):1343–1351
Jang WS, Lim JU, Joo KR et al (2015) Outcome of conservative percutaneous cholecystostomy in high-risk patients with acute cholecystitis and risk factors leading to surgery. Surg Endosc 29(8):2359–2364
Chang YR, Ahn YJ, Jang JY et al (2014) Percutaneous cholecystostomy for acute cholecystitis in patients with high comorbidity and re-evaluation of treatment efficacy. Surgery 155(4):615–622
Granlund A, Karlson BM, Elvin A et al (2001) Ultrasound-guided percutaneous cholecystostomy in high-risk surgical patients. Langenbecks Arch Surg 386(3):212–217
Eggermont AM, Lameris JS, Jeekel J (1985) Ultrasound-guided percutaneous transhepatic cholecystostomy for acute acalculous cholecystitis. Arch Surg 120(12):1354–1356
Berger H, Pratschke E, Arbogast H et al (1989) Percutaneous cholecystostomy in acute acalculous cholecystitis. Hepatogastroenterology 36(5):346–348
Shirai Y, Tsukada K, Kawaguchi H et al (1993) Percutaneous transhepatic cholecystostomy for acute acalculous cholecystitis. Br J Surg 80(11):1440–1442
Kirkegard J, Horn T, Christensen SD et al (2015) Percutaneous cholecystostomy is an effective definitive treatment option for acute acalculous cholecystitis. Scand J Surg 104(4):238–243
Shea JA, Berlin JA, Escarce JJ et al (1994) Revised estimates of diagnostic test sensitivity and specificity in suspected biliary tract disease. Arch Intern Med 154(22):2573–2581
Ambe PC, Zirngibl H (2015) The fate of patients managed with percutaneous cholecystostomy for acute cholecystitis. Surgery 159(5):1479–1480
Akyurek N, Salman B, Yuksel O et al (2005) Management of acute calculous cholecystitis in high-risk patients: percutaneous cholecystotomy followed by early laparoscopic cholecystectomy. Surg Laparosc Endosc Percutaneous Tech 15(6):315–320
Acknowledgements
This manuscript has not been submitted or published elsewhere, and the authors have nothing to disclose. The authors acknowledge Drs. Loretta Coady-Fariborzian, MD and Elisha Collins, MD for their assistance in obtaining IRB approval. This work was supported in part by R01 GM113945-01 (PAE), R01 GM105893-01A1 (AMM), P50 GM111152–01 (SCB, FAM, PAE, AMM) awarded by the National Institute of General Medical Sciences (NIGMS). TJL was supported by a post-graduate training Grant (T32 GM-08721) in burns, trauma and perioperative injury by NIGMS. Research reported in this publication was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under Award Number UL1TR001427. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Loftus, T.J., Brakenridge, S.C., Dessaigne, C.G. et al. Antibiotics May be Safely Discontinued Within One Week of Percutaneous Cholecystostomy. World J Surg 41, 1239–1245 (2017). https://doi.org/10.1007/s00268-016-3861-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-016-3861-y