
Abstract
Background
The Tokyo Guidelines for the management of acute cholangitis and cholecystitis (TG07) were published in 2007 as the world’s first guidelines for acute cholangitis and cholecystitis. The diagnostic criteria and severity assessment of acute cholecystitis have since been widely used all over the world. A validation study of TG07 has shown that the diagnostic criteria for acute cholecystitis are highly reliable but that the definition of definite diagnosis is ambiguous. In addition, considerable new evidence referring to acute cholecystitis as well as evaluations of TG07 have been published. Consequently, we organized the Tokyo Guidelines Revision Committee to evaluate TG07, recognize new evidence, and conduct a multi-center analysis to revise the guidelines (TG13).
Methods and materials
We retrospectively analyzed 451 patients with acute cholecystitis from multiple tertiary care centers in Japan. All 451 patients were first evaluated using the criteria in TG07. The “gold standard” for acute cholecystitis in this study was a diagnosis by pathology. The validity of TG07 diagnostic criteria was investigated by comparing clinical with pathological diagnosis.
Results
Of 451 patients evaluated, a total of 227 patients were given a diagnosis of acute cholecystitis by pathological examination (prevalence 50.3 %). TG07 criteria provided a definite diagnosis of acute cholecystitis in 224 patients. The sensitivity of TG07 diagnostic criteria for acute cholecystitis was 92.1 %, and the specificity was 93.3 %. Based on the preliminary results, new diagnostic criteria for acute cholecystitis were proposed. Using the new criteria, the sensitivity of definite diagnosis was 91.2 %, and the specificity was 96.9 %. The accuracy rate was improved from 92.7 to 94.0 %. In regard to severity grading among 227 patients, 111 patients were classified as Mild (Grade I), 104 as Moderate (Grade II), and 12 as Severe (Grade III).
Conclusion
The proposed new diagnostic criteria achieved better performance than the diagnostic criteria in TG07. Therefore, the proposed criteria have been adopted as new diagnostic criteria for acute cholecystitis and are referred to as the 2013 Tokyo Guidelines (TG13). Regarding severity assessment, no new evidence was found to suggest that the criteria in TG07 needed major adjustment. As a result, TG07 severity assessment criteria have been adopted in TG13 with minor changes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Acute cholecystitis is a very common complication of cholelithiasis, and as such is frequently encountered in surgical practice [1–4]. There were no diagnostic criteria or severity assessment criteria for this common disease until 2007. In 2006, we conducted a systematic review and sponsored an international consensus conference in Tokyo, Japan. This meeting resulted in the development of the Tokyo Guidelines for the management of acute cholangitis and cholecystitis (TG07). These guidelines were the world’s first guidelines to include diagnostic criteria and severity assessment of acute cholecystitis [5] (Tables 1, 2).
Diagnostic and severity assessment criteria need to be updated periodically based on new information, criticisms, and suggestions for improvement. The diagnostic criteria in TG07 have been set to achieve high sensitivity in order to provide medical care suitable for a large number of patients. The sensitivity of TG07 diagnostic criteria has been reported to be 84.9 % [6] and TG07 diagnostic criteria are recognized as those to be recommended in current care for acute cholecystitis [1]. However, since its publication, we and others have found potential shortcomings in TG07 in clinical practice [6].
To update the Tokyo Guidelines for the management of acute cholangitis and cholecystitis, we organized the Tokyo Guidelines Revision Committee to evaluate TG07, recognize new evidence, and conduct a multi-center analysis to revise the guidelines (TG13). In the present study, we investigated the validity of the TG07 diagnostic criteria and severity assessment criteria by multi-center analysis. The limitations of TG07 were also investigated to develop tentative new diagnostic criteria and severity assessment criteria.
Methods and materials
We retrospectively analyzed 451 patients from six tertiary care centers in Japan between November 2005 and November 2011: Sapporo Medical University, Tokyo Medical University, Tokyo Women’s Medical University, Nagoya Daini Red Cross Hospital, Ogaki Municipal Hospital, and Fukuoka University School of Medicine. Consecutive patients who were operated on for cholecystectomy were included during the study period. The “gold standard” for acute cholecystitis in this study was pathological diagnosis using standard gross and histological criteria. We therefore confirmed the final diagnosis by pathological examination of excised gallbladders after operation. If the pathological findings were chronic cholecystitis or other, those cases were considered to be “negative.”
All 451 patients were evaluated using TG07 criteria. The validity of the diagnostic criteria of TG07 was investigated by analyzing their sensitivity and specificity. The severity grading system of TG07 was evaluated by determining the distribution of severity among these patients. Through these data, the Tokyo Guidelines Revision Committee members discussed the quality of diagnostic criteria and severity assessment of acute cholecystitis in TG07 to reassess TG and propose new guidelines.
The literature was selected as follows: using “Tokyo Guidelines” AND “acute cholecystitis[MeSH]”, only 3 items were selected in PubMed since the publication of TG07 (1 April 2007 – 31 March 2012). These articles were screened with “human” and “English”. However, using “acute cholecystitis[MeSH]” AND “prognosis[MeSH]”, a total of 119 items were selected in PubMed over the same length of time. From these articles, the prognostic factors of acute cholecystitis to be utilized for the revision of TG07 were screened by the Tokyo Guidelines Revision Committee members. In addition, the distribution of severity grading was aggregated from the literature which reported the data based on the severity assessment of TG07.
The Tokyo Guidelines Revision Committee discussed the modification of TG07 diagnostic criteria and severity assessment of acute cholecystitis by analyzing the results of the present study and integrating the literature evidence.
Results
Assessment of TG07 diagnostic criteria and severity assessment criteria for acute cholecystitis
The 451 patients who were operated on for cholecystectomy comprised 255 male patients and 196 female patients with a mean age of 63.9 ± 14.0 years. 227 of the 451 patients enrolled were given a final pathological diagnosis of acute cholecystitis. The prevalence of acute cholecystitis in the cohort was 50.3 %. Based on the diagnostic criteria in TG07, a definite diagnosis of acute cholecystitis was made in 224 patients. Diagnostic criteria were not met in the remaining 227 patients.
We constructed 2 × 2 contingency tables between pathologically proven acute cholecystitis and acute cholecystitis diagnosed by TG07 criteria. There were 209 true-positive cases, 15 false-positive cases, 18 false-negative cases, and 209 true-negative cases (Table 3). The diagnostic sensitivity and specificity of TG07 were 92.1 % (209/227) and 93.3 % (209/224), respectively; the false-negative and false-positive rates were 7.9 % (18/227) and 6.7 % (15/224), respectively. The positive and negative predictive values were 93.3 and 92.1 %, respectively, and the positive and negative likelihood ratios were 13.75 and 0.08, respectively. The diagnostic accuracy was 92.7 %.
In terms of severity assessment, a total of 227 patients who were given a final pathological diagnosis of acute cholecystitis were retrospectively examined with TG07 severity assessment criteria for acute cholecystitis. Of them, 111 patients were classified as Grade I (48.9 %), 104 patients as Grade II (45.8 %), and 12 patients as Grade III (5.3 %), respectively.
Revision of TG07 diagnostic criteria and severity assessment criteria for acute cholecystitis
Several problems regarding the TG07 diagnostic criteria and severity assessment system were found during the analysis. The most important problem in TG07 was that the criteria for definite diagnosis were ambiguous and difficult to use. In TG07, there were two categories determining the definite diagnosis of acute cholecystitis (Table 1). Definite diagnosis 1: To obtain a definite diagnosis one item in A and one item in B had to be positive. Definite diagnosis 2: Imaging findings (Criterion C) confirmed the diagnosis when acute cholecystitis was suspected clinically. The Tokyo Guidelines Revision Committee concluded that the term “definite diagnosis” could not be supported in current practice without positive diagnostic imaging studies.
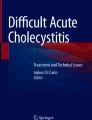
For acute cholecystitis, abdominal ultrasonography, computed tomography (CT), and hepatobiliary scintigraphy (HIDA scan) are the imaging studies most commonly used in diagnosis. In particular, ultrasonography is a test that should be performed first of all in every case for which acute cholecystectomy is suspected. Sonography should be the screening test of choice in acute cholecystitis because it is cost-effective, prospectively highly accurate and fast [7]. The sensitivity of ultrasonography in detecting acute inflammation of the gallbladder has been reported to be 90–95 % [8]. Therefore, emergency room clinicians and surgeons currently prefer ultrasonography for the initial evaluation of suspected acute cholecystitis, because it is a simple, safe, fast and cost-effective tool [9–11]. Acute calculous cholecystitis is diagnosed radiologically by the concomitant presence of thickening of the gallbladder wall (5 mm or greater), pericholecystic fluid, or direct tenderness when the probe is pushed against the gallbladder (ultrasonographic Murphy’s sign) [1] (Fig. 1). CT findings of acute cholecystitis were reported as gallbladder distention (41 %), gallbladder wall thickening (59 %), pericholecystic fat density (52 %), pericholecystic fluid collection (31 %), subserosal edema (31 %) and high-attenuation gallbladder bile (24 %) [12].

Typical US image of acute cholecystitis, demonstrating gallbladder swelling, wall thickening with sonolucent layers, massive debris, and the stone impaction in the cystic duct
As a result, the importance of diagnostic imaging was emphasized for the diagnosis of acute cholecystitis by the Committee, and new criteria were proposed (Table 4). In the proposed criteria a “suspected” diagnosis is achieved when one item from section A and one item from section B are present. A “definite” diagnosis is achieved when imaging findings characteristic of acute cholecystitis (Item C) are also present.
Regarding severity assessment criteria, a thorough literature search was performed and variables reported in the literature as predictive of poor prognosis in acute cholecystitis were summarized [13–25] (Table 5). The Tokyo Guidelines Revision Committee discussed whether these newly reported severity or prognostic factors such as diabetes mellitus, old age, and male sex should be adopted for revision. However, the Committee concluded that these factors were not supported by sufficient levels of evidence and so the factors were not adopted as assessment criteria. However, minor changes were made to the description of Grade III severity, i.e. dopamine and norepinephrine were both considered as evidence of cardiovascular dysfunction consistent with the SOFA score system [26] (Table 6).
Assessment of TG13 diagnostic criteria and severity assessment for acute cholecystitis
Of 227 patients with a definite diagnosis of acute cholecystitis based on the proposed new diagnostic criteria, a final diagnosis of acute cholecystitis by pathology was made in 207 patients. We constructed 2 × 2 contingency tables between patients with acute cholecystitis by pathology and the cases with definite diagnosis using the proposed new diagnostic criteria, with 207 true-positive cases, 7 false-positive cases, 20 false-negative cases, and 217 true-negative cases (Table 7).
The diagnostic sensitivity and specificity of definite diagnosis were 91.2 % (207/227) and 96.9 % (217/224), respectively. The false-negative and false-positive rates were 8.8 % (20/227) and 3.1 % (7/224), respectively. The positive and negative predictive values were 96.7 and 91.6 %, respectively. The positive and negative likelihood ratios were 29.18 and 0.09, respectively. The diagnostic accuracy was 94.0 %. On the other hand, of the 219 patients with a suspected or definite diagnosis of acute cholecystitis based on the proposed new diagnostic criteria, a final diagnosis of acute cholecystitis was made in 208 patients. We constructed 2 × 2 contingency tables between patients with acute cholecystitis by pathology and the cases with suspected or definite diagnosis using the proposed new diagnostic criteria, with 208 true-positive cases, 11 false-positive cases, 19 false-negative cases, and 213 true-negative cases (Table 8). The diagnostic sensitivity and specificity of suspected or definite diagnosis were 91.6 % (208/227) and 95.1 % (213/224), respectively. The false-negative and false-positive rates were 8.4 % (19/227) and 4.9 % (11/224), respectively. The positive and negative predictive values were 95.0 and 91.8 %, respectively. The positive and negative likelihood ratios were 18.66 and 0.09, respectively. The diagnostic accuracy was 93.3 %.
From those results the diagnostic validities were compared between the definite diagnosis of TG07 and that of the proposed new diagnostic criteria (Table 9).
This comparison of the two diagnostic criteria in terms of diagnostic precision shows that the proposed new diagnostic criteria achieved better performance than TG07. These diagnostic criteria have therefore been chosen as the new diagnostic criteria of acute cholecystitis referred to as the Tokyo Guidelines (TG13).
On the other hand, the TG07 severity assessment criteria for acute cholecystitis did not have significant problems that required major revision of the definitions or structures. The TG07 severity assessment criteria have been adopted in the updated Tokyo Guidelines (TG13) with minor changes in descriptions as above (Table 6).
Discussion
The most important role of diagnostic criteria and severity assessment is to allow early diagnosis and to provide the most appropriate treatment for the disease depending on its severity. TG07 of acute cholecystitis aimed at this by systematic literature search and integration of expert opinions through a consensus conference held in Tokyo in 2006 [27]. The guidelines should reflect the current clinical practice but they need periodic assessment and revision. However, in the case of TG07 this was particularly so because of shortcomings that became evident through application in clinical practice and as a result of new information in the literature.
For the diagnosis of acute cholecystitis, clinicians all over the world have provided treatment for acute cholecystitis based on Murphy’s sign. However, Murphy’s sign has been reported in previous studies to have a sensitivity of 50–60 % and a high specificity of 79 % [28] or 96 % [2] for the diagnosis of acute cholecystitis. The sensitivity of Murphy’s sign was once reported to be as low as 20.5 %, while the specificity was 87.5 % [6]. In the same study, the sensitivity and specificity of TG07 were as high as 84.9 and 50.0 %, respectively [6]. In this study, a sign test, which detects the difference in accuracy, was also performed to analyze statistically the diagnostic criteria of TG07 for acute cholecystitis and the rate of diagnostic accuracy of Murphy’s sign. The diagnostic accuracy was significantly higher when the TG07 were used than when Murphy’s sign was used [6]. TG07 can be used with more confidence among clinicians. However, the shortcomings of TG07 were recognized by the Tokyo Guidelines Revision Committee in that the definite diagnosis of TG07 had two categories. These two categories were ambiguous and the schema was difficult to use for many clinicians.
In addition to clinical and laboratory assessments, radiological and nuclear imaging techniques are widely used to identify individuals with complications of gallbladder disease [21]. Ultrasonographic diagnosis of acute cholecystitis was made when thickening and/or edema of gallbladder wall, distension of the gallbladder by gallstones, and pericholecystic fluid collection were seen [29].
Based on the above understanding, tentative new diagnostic criteria of acute cholecystitis were developed and their validity was analyzed among the patients from multiple institutions in Japan. Better diagnostic accuracy was obtained with the new criteria, with high sensitivity and high specificity on definite diagnosis. The new criteria validated by a retrospective analysis have been adopted as the revised diagnostic criteria of TG13 for acute cholecystitis.
The severity assessment criteria were reconsidered by the Tokyo Guidelines Revision Committee with new information, evidence, and evaluations of TG07. Lee et al. [14] revealed that there was a significantly shorter mean length of hospital stay in the patient group for whom the Tokyo guidelines (TG07) were utilized compared with those without compliance with TG07. Asai et al. [30] suggested that more precise severity grades may need to be established, including age and C-reactive protein as additional parameters.
The distribution of severity grading varies as follows: 39.3–68.5 % of the cases were classified as Grade I, 25.5–59.5 % as Grade II, and 1.2–6 % as Grade III [14, 30]. The present study shows that 48.9 % of the cases were classified as Grade I, 45.8 % as Grade II, and 5.3 % as Grade III. The proportions in the present study were not different from the proportions in other TG07 studies (Table 10).
In summary, TG13 presents new diagnostic and severity assessment criteria based on a large patient base and a reasonable “gold standard”. These criteria allow early diagnosis and severity assessment of the disease and should be clinically very useful in the management of acute cholecystitis.
Conclusion
The updated Tokyo Guidelines (TG13) introduce a new standard for the diagnosis and severity assessment of acute cholecystitis. In the TG13 diagnostic criteria, a “suspected” diagnosis is achieved when one item from section A and one item from section B are present. A “definite” diagnosis is achieved when imaging findings characteristic of acute cholecystitis (Item C) are also present. Compared with TG07, the validity of the diagnostic criteria has been improved and the severity assessment criteria of TG07 have been adopted with minor changes from TG07.
References
Strasberg SM. Acute calculous cholecystitis. N Engl J Med 2008; 358: 2804–11.
Eskelinen M, Ikonen J, Lipponen P. Diagnostic approaches in acute cholecystitis; a prospective study of 1333 patients with acute abdominal pain. Theor Surg. 1993;8:15–20.
Halasz NA. Counterfeit cholecystitis, a common diagnostic dilemma. Am J Surg. 1975;130:189–93.
Johnson H Jr, Cooper B. The value of HIDA scans in the initial evaluation of patients for cholecystitis. J Natl Med Assoc. 1995;87:27–32.
Hirota M, Takada T, Kawarada Y, Nimura Y, Miura F, Hirata K, Mayumi T, Yoshida M, Strasberg S, Pitt H, Gadacz TR, de Santibanes E, Gouma DJ, Solomkin JS, Belghiti J, Neuhaus H, Büchler MW, Fan ST, Ker CG, Padbury RT, Liau KH, Hilvano SC, Belli G, Windsor JA, Dervenis C. Diagnostic criteria and severity assessment of acute cholecystitis: TokyoGuidelines. J Hepatobiliary Pancreat Surg. 2007;14(1):78–82 (Epub 2007 Jan 30).
Yokoe M, Takada T, Mayumi T, Yoshida M, Hasegawa H, Norimizu S, Hayashi K, Umemura S, Orito E. Accuracy of the Tokyo Guidelines for the diagnosis of acute cholangitis and cholecystitis taking into consideration the clinical practice pattern in Japan. J Hepatobiliary Pancreat Sci. 2011;18:250–7.
Ralls PW, Colletti PM, Lapin SA, Chandrasoma P, Boswell WD Jr, Ngo C, Radin DR, Halls JM. Real-time sonography in suspected acute cholecystitis. Prospective evaluation of primary and secondary signs. Radiology. 1985; 155(3):767–71.
Hunt DR, Chu FC. Gangrenous cholecystitis in the laparoscopic era. Aust NZ J Surg. 2000;70:428–30.
Alobaidi M, Gupta R, Jafri SZ, Fink-Bennet DM. Current trends in imaging evaluation of acute cholecystitis. Emerg Radiol. 2004;10:256–8.
Rosen Cl, Brown DF, Chang Y, Moore C, Averill NJ, Arkoff LJ, Mccabe CJ, Wolfe RE. Ultrasonography by emergency physicians in patients with suspected cholecystitis. Am J Emerg Med 2001; 19: 32–36.
Kendall JL, Shimp RJ. Performance and interpretation of focused right upper quadrant ultrasound by emergency. J Emerg Med. 2001;21:7–13.
Fidler J, Paulson EK, Layfield L. CT evaluation of acute cholecystitis: findings and usefulness in diagnosis. AJR. 1996;166:1085–8.
Gruber PJ, Silverman RA, Gottesfeld S, Flaster E. Presence of fever and leukocytosis in acute cholecystitis. Ann Emerg Med. 1996;28:273–7.
Lee SW, Yang SS, Chang CS, Yeh HJ. Impact of the Tokyo guidelines on the management of patients with acute calculous cholecystitis. J Gastroenterol Hepatol. 2009; 24(12):1857–61 (Epub).
Lee SW, Chang CS, Lee TY, Tung CF, Peng YC. The role of the Tokyo guidelines in the diagnosis of acute calculous cholecystitis. J Hepatobiliary Pancreat Sci. 2010; 17(6): 879–84 (Epub 2010 Apr 24).
Juvonen T, Kiviniemi H, Niemela O, Kairaluoma MI. Diagnostic accuracy of ultrasonography and C reactive protein concentration in acute cholecystitis: a prospective clinical study. Eur J Surg. 1992;158:365–9.
Nguyen L, Fagan SP, Lee TC, Aoki N, Itani KM, Berger DH, Awad SS. Use of a predictive equation for diagnosis of acute gangrenous cholecystitis. Am J Surg. 2004;188(5):463–6.
Contini S, Corradi D, Busi N, Alessandri L, Pezzarossa A, Scarpignato C. Can gangrenous cholecystitis be prevented?: a plea against a “wait and see” attitude. J Clin Gastroenterol. 2004;38(8):710–6.
Girgin S, Gedik E, Taçyildiz IH, Akgün Y, Baç B, Uysal E. Factors affecting morbidity and mortality in gangrenous cholecystitis. Acta Chir Belg. 2006; 106(5):545–9.
Fagan SP, Awad SS, Rahwan K, Hira K, Aoki N, Itani KM, Berger DH. Prognostic factors for the development of gangrenous cholecystitis. Am J Surg. 2003;186(5):481–5.
Aydin C, Altaca G, Berber I, Tekin K, Kara M, Titiz I. Prognostic parameters for the prediction of acute gangrenous cholecystitis. J Hepatobiliary Pancreat Surg. 2006;13(2):155–9.
Yacoub WN, Petrosyan M, Sehgal I, Ma Y, Chandrasoma P, Mason RJ. Prediction of patients with acute cholecystitis requiring emergent cholecystectomy: a simple score. Gastroenterol Res Pract. 2010; 2010:901739 (Epub 2010 Jun 8).
Wang AJ, Wang TE, Lin CC, Lin SC, Shih SC. Clinical predictors of severe gallbladder complications in acute acalculous cholecystitis. World J Gastroenterol. 2003;9(12):2821–3.
McChesney JA, Northup PG, Bickston SJ. Acute acalculous cholecystitis associated with systemic sepsis and visceral arterial hypoperfusion: a case series and review of pathophysiology. Dig Dis Sci. 2003;48(10):1960–7.
Young AL, Cockbain AJ, White AW, Hood A, Menon KV, Toogood GJ. Index admission laparoscopic cholecystectomy for patients with acute biliary symptoms: results from a specialist centre. HPB (Oxford). 2010;12(4):270–6.
Vincent JL, Moreno R, Takala J, Willatts S, De Mendonça A, Bruining H, Reinhart CK, Suter PM, Thijs LG. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996;22(7):707–10.
Mayumi T, Takada T, Kawarada Y, Nimura Y, Yoshida M, Sekimoto M, et al. Results of the Tokyo Consensus Meeting Tokyo Guidelines. J Hepatobiliary Pancreat Surg. 2007;14:114–21.
Trowbridge RL, Rutkowski NK, Shojania KG. Does this patient have acute cholecystitis? JAMA. 2003;289:80–6.
Weiss CA III, Schwartz RW. Current diagnosis and treatment of cholecystitis. Curr Surg. 2002;59:51–4.
Asai K, Watanabe M, Kusachi S, Tanaka H, Matsukiyo H, Osawa A, Saito T, Kodama H, Enomoto T, Nakamura Y, Okamoto Y, Saida Y, Nagao J. Bacteriological analysis of bile in acute cholecystitis according to the Tokyo guidelines. J Hepatobiliary Pancreat Sci. 2011 (Epub ahead of print).
Open Access
This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Yokoe, M., Takada, T., Strasberg, S.M. et al. New diagnostic criteria and severity assessment of acute cholecystitis in revised Tokyo guidelines. J Hepatobiliary Pancreat Sci 19, 578–585 (2012). https://doi.org/10.1007/s00534-012-0548-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00534-012-0548-0