
Abstract
Background
Peri-operative hemodynamic instability (HDI) may increase peri-operative morbidity in pheochromocytoma/paraganglioma (PPGL) patients.
Objective
This study aimed to determine which tumor-related risk factors could lead to peri-operative HDI in unilateral or single PPGL removal.
Methods
Before surgery, 66 PPGL patients had at least two sets of 24 h urine collected for fractionated catecholamine analysis. At surgery, an arterial line was inserted to record systolic blood pressure (SBP), diastolic BP, and mean arterial BP (MAP). Peri-operative HDI was defined as hypertension (SBP > 160 mmHg) and/or hypotension (SBP < 90 mmHg and/or MAP < 60 mmHg) for >10 consecutive minutes either intra-operatively or within the first 12 h after surgery. Urinary fractionated catecholamines and other variables were compared between those with peri-operative HDI (group I) and those without (group II).
Results
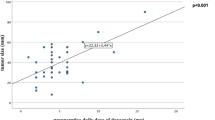
A total of 15 (22.7 %) patients belonged to group I, while 51 patients belonged to group II. One (1.5 %) patient died 9 days after surgery. Relative to group II, group I had significantly higher urinary norepinephrine (NE) (5,488.0 vs. 1,980.0 nmol/L, p < 0.001), urinary normetanephrine (5,130.9 vs. 3,853.4 nmol/L, p = 0.045), maximum SBP at operation (188.2 vs. 167.4 mmHg, p = 0.037), but lower MAP after operation (78.9 vs. 91.8 mmHg, p = 0.026). Urinary NE (OD 1.02, 95 % confidence interval [CI] 1.01–1.03, p = 0.046) was an independent risk factor for peri-operative HDI. The urinary NE level significantly correlated with maximum intra-operative SBP and MAP (r 0.692, p < 0.001; and r 0.669, p < 0.001, respectively) and inversely correlated with maximum post-operative MAP (r −0.305, p = 0.040).
Conclusions
High pre-operative urinary NE was an independent tumor-related factor for peri-operative HDI and significantly correlated with sustained intra-operative hypertension and post-operative hypotension.
Similar content being viewed by others


References
Lenders JW, Eisenhofer G, Mannelli M, Pacak K (2005) Phaeochromocytoma. Lancet 366(9486):665–675
Kercher KW, Novitsky YW, Park A, Matthews BD, Litwin DE, Heniford BT (2005) Laparoscopic curative resection of pheochromocytomas. Ann Surg 241(6):919–926 discussion 926–8
Plouin PF, Duclos JM, Soppelsa F, Boublil G, Chatellier G (2001) Factors associated with perioperative morbidity and mortality in patients with pheochromocytoma: analysis of 165 operations at a single center. J Clin Endocrinol Metab 86(4):1480–1486
Galetta F, Franzoni F, Bernini G, Poupak F, Carpi A, Cini G, Tocchini L, Antonelli A, Santoro G (2010) Cardiovascular complications in patients with pheochromocytoma: a mini-review. Biomed Pharmacother 64(7):505–509
Pacak K (2007) Preoperative management of the pheochromocytoma patient. J Clin Endocrinol Metab 92(11):4069–4079
Bruynzeel H, Feelders RA, Groenland TH, van den Meiracker AH, van Eijck CH, Lange JF, de Herder WW, Kazemier G (2010) Risk factors for hemodynamic instability during surgery for pheochromocytoma. J Clin Endocrinol Metab 95(2):678–685
Kinney MA, Warner ME, vanHeerden JA, Horlocker TT, Young WF Jr, Schroeder DR, Maxson PM, Warner MA (2000) Perianesthetic risks and outcomes of pheochromocytoma and paraganglioma resection. Anesth Analg 91(5):1118–1123
Agrawal R, Mishra SK, Bhatia E, Mishra A, Chand G, Agarwal G, Agarwal A, Verma AK (2014) Prospective study to compare peri-operative hemodynamic alterations following preparation for pheochromocytoma surgery by phenoxybenzamine or prazosin. World J Surg 38(3):716–723. doi:10.1007/s00268-013-2325-x
Ulchaker JC, Goldfarb DA, Bravo EL, Novick AC (1999) Successful outcomes in pheochromocytoma surgery in the modern era. J Urol 161(3):764–767
O’Callaghan CJ, Williams B (2002) The regulation of human vascular smooth muscle extracellular matrix protein production by alpha- and beta-adrenoceptor stimulation. J Hypertens 20(2):287–294
Faber JE, Yang N, Xin X (2001) Expression of alpha-adrenoceptor subtypes by smooth muscle cells and adventitial fibroblasts in rat aorta and in cell culture. J Pharmacol Exp Ther 298(2):441–452
Zhang H, Faber JE (2001) Trophic effect of norepinephrine on arterial intima-media and adventitia is augmented by injury and mediated by different alpha1-adrenoceptor subtypes. Circ Res 89(9):815–822
Higashi Y, Sasaki S, Nakagawa K, Kimura M, Sasaki S, Noma K, Matsuura H, Hara K, Goto C, Oshima T, Chayama K (2002) Excess norepinephrine impairs both endothelium-dependent and -independent vasodilation in patients with pheochromocytoma. Hypertension 39(2 Pt 2):513–518
Petrák O, Strauch B, Zelinka T, Rosa J, Holaj R, Vránková A, Kasalický M, Kvasnicka J, Pacák K, Widimský J Jr (2010) Factors influencing arterial stiffness in pheochromocytoma and effect of adrenalectomy. Hypertens Res 33(5):454–459
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Chang, R.Y.K., Lang, B.HH., Wong, K.P. et al. High Pre-Operative Urinary Norepinephrine is an Independent Determinant of Peri-Operative Hemodynamic Instability in Unilateral Pheochromocytoma/Paraganglioma Removal. World J Surg 38, 2317–2323 (2014). https://doi.org/10.1007/s00268-014-2597-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-014-2597-9