
Abstract
Background
Size can predict malignancy in adrenocortical tumors, but the same extrapolation for pheochromocytomas (PCC) is controversial. The goal of this study was to find a correlation between the tumor size and malignant potential of PCC and determine whether the “Pheochromocytoma of the adrenal gland scaled score” (PASS) proposed by Thompson can be applied to predict malignancy.
Methods
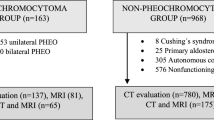
A retrospective analysis of patients with PCC operated on from 1991 to 2007 revealed 98 PCC removed from 93 patients. Tumor size was available for 90 tumors. Six (6.4%) patients had proven malignancy. Five familial cases were excluded from the PASS analysis.
Results
Of the benign cases, none developed recurrence or metastasis. There were 54 (60%) tumors > 6 cm and 36 (40%) tumors ≤ 6 cm. All 12 PASS parameters were individually present in higher frequency in the >6-cm group; but the difference was not statistically significant except cellular monotony (p = 0.02). Overall, a PASS ≤ 4 was found in 57 patients. Mean PASS was statistically significantly higher in the >6-cm group (4.4 vs. 3.3, p = 0.04). Of the sporadic benign cases, 21 (41%) patients with tumor size > 6 cm had a PASS of >4, and none of them developed metastasis. PASS ≤ 4 was found in 25 (81%) PCC in the ≤6-cm group, and none developed metastases. PASS ≥ 4 was found in six (19%) patients in the ≤6-cm group, and none developed metastases. 68 patients completed 5-year follow-up, and the remaining had a mean follow-up of 28.7 months. No correlation was found between tumor size and PASS > 4 and PASS ≤ 4 (7.8 cm vs. 7.1 cm; p = 0.23).
Conclusions
Presently there is not enough evidence to indict a large (>6 cm) PCC as malignant. Furthermore, PASS cannot be reliably applied to PCC for predicting malignancy.
Similar content being viewed by others


References
Kim HH, Kim GH, Sung GT (2004) Laparoscopic adrenalectomy for pheochromocytoma: comparison with conventional open adrenalectomy. J Endourol 18(3):251–255
Davies MJ, McGlade DP, Banting SW (2004) A comparison of open and laparoscopic approaches to adrenalectomy in patients with phaeochromocytoma. Anaesth Intensive Care 32(2):224–229
Miskulin J, Shulkin BL, Doherty GM, Sisson JC, Burney RE, Gauger PG (2003) Is preoperative iodine 123 meta-iodobenzylguanidine scintigraphy routinely necessary before initial adrenalectomy for pheochromocytoma? Surgery 134(6):918–922 discussion 922–923
Thompson LD (2002) Pheochromocytoma of the Adrenal Gland Scaled Score (PASS) to separate benign from malignant neoplasms: a clinicopathologic and immunophenotypic study of 100 cases. Am J Surg Pathol 26(5):551–566
Wu D, Tischler AS, Lloyd RV, DeLellis RA, de Krijger R, van Nederveen F et al (2009) Observer variation in the application of the Pheochromocytoma of the Adrenal Gland Scaled Score. Am J Surg Pathol 33(4):599–608
Strong VE, Kennedy T, Al-Ahmadie H, Tang L, Coleman J, Fong Y et al (2008) Prognostic indicators of malignancy in adrenal pheochromocytomas: clinical, histopathologic, and cell cycle/apoptosis gene expression analysis. Surgery 143(6):759–768
Harrison LE, Gaudin PB, Brennan MF (1999) Pathologic features of prognostic significance for adrenocortical carcinoma after curative resection. Arch Surg 134(2):181–185
Goldstein RE, O’Neill JA Jr, Holcomb GW 3rd, Morgan WM 3rd, Neblett WW III, Oates JA et al (1999) Clinical experience over 48 years with pheochromocytoma. Ann Surg 229(6):755–764 discussion 764-766
Remine WH, Chong GC, Van Heerden JA, Sheps SG, Harrison EG Jr (1974) Current management of pheochromocytoma. Ann Surg 179(5):740–748
van Heerden JA, Roland CF, Carney JA, Sheps SG, Grant CS (1990) Long-term evaluation following resection of apparently benign pheochromocytoma(s)/paraganglioma(s). World J Surg 14(3):325–329
Proye C, Vix M, Goropoulos A, Kerlo P, Lecomte-Houcke M (1992) High incidence of malignant pheochromocytoma in a surgical unit. 26 cases out of 100 patients operated from 1971 to 1991. J Endocrinol Invest 15(9):651–663
Proye CA, Vix M, Jansson S, Tisell LE, Dralle H, Hiller W (1994) “The” pheochromocytoma: a benign, intra-adrenal, hypertensive, sporadic unilateral tumor. Does it exist? World J Surg 18(4):467–472
O'Riordain DS, Young WF Jr, Grant CS, Carney JA, van Heerden JA (1996) Clinical spectrum and outcome of functional extraadrenal paraganglioma. World J Surg 20(7):916–921
Linnoila RI, Keiser HR, Steinberg SM, Lack EE (1990) Histopathology of benign versus malignant sympathoadrenal paragangliomas: clinicopathologic study of 120 cases including unusual histologic features. Hum Pathol 21(11):1168–1180
Nativ O, Grant CS, Sheps SG, O’Fallon JR, Farrow GM, van Heerden JA et al (1992) Prognostic profile for patients with pheochromocytoma derived from clinical and pathological factors and DNA ploidy pattern. J Surg Oncol 50(4):258–262
John H, Ziegler WH, Hauri D, Jaeger P (1999) Pheochromocytomas: can malignant potential be predicted? Urology 53(4):679–683
Agarwal A, Gupta S, Mishra AK, Singh N, Mishra SK (2005) Normotensive pheochromocytoma: institutional experience. World J Surg 29(9):1185–1188
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
Amit Agarwal and Prateek K. Mehrotra are joint first authors.
Rights and permissions
About this article
Cite this article
Agarwal, A., Mehrotra, P.K., Jain, M. et al. Size of the Tumor and Pheochromocytoma of the Adrenal Gland Scaled Score (PASS): Can They Predict Malignancy?. World J Surg 34, 3022–3028 (2010). https://doi.org/10.1007/s00268-010-0744-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-010-0744-5