
Abstract
Purpose
Many reports outline the benefits derived from using the direct anterior approach (DAA) in primary total hip arthroplasty (THA); however, the learning curve for the DAA has not been well documented, and the complications associated with the DAA during this learning curve seem relatively high. The aim of this study was to investigate implant positioning in primary THA, when the surgeon was a novice at the DAA, and had previously used the standard posterior approach (PA).
Patients and methods
We investigated implant positioning in the first 80 consecutive THA cases performed by two senior surgeons using the DAA (with fluoroscopic assistance), and compared them to the same two surgeons’ previous 80 respective THA cases performed using their previous standard posterior approach.
Results
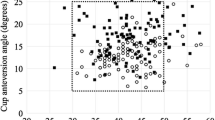
Cup positioning accuracy was higher for the DAA (p < 0.001) but greater cup anteversion (19.3° ± 11.0 using the PA vs 27.6° ± 6.3 using DAA, p < 0.0001) was also demonstrated. A total of 69.3 % of cups in the DAA group were positioned with an anteversion angle greater than their target angle. In the DAA group the stem was more frequently positioned in flexion and less frequently in neutral than for the PA group.
Conclusions
Although fluoroscopic assistance seemed to decrease complications such as femoral fracture, surgeons changing from PA to DAA for THA should consider potential excessive cup anteversion and flexion implantation of the stem in their early experience with DAA.





Similar content being viewed by others


References
Hueter C (1883) Funfte Abteilung: die Verletzung und Krankheiten des Hüftgelenkes, neun und zwanzigstes capitel. In: Hueter C (ed) Grundriss der Chirurgie, 2nd edn. FCW Vogel, Leipzig, pp 129–200
Judet J, Judet H (1985) Voie d’abord antérieur dans l’arthroplastie totale de la hanche. Presse Med 14:1031–1033
Chechik O, Khashan M, Lador R, Lador R, Salai M, Amar E (2013) Surgical approach and prosthesis fixation in hip arthroplasty worldwide. Arch Orthop Trauma Surg 133:1595–600
Matta JM, Shahrdar C, Ferguson T (2005) Single-incision anterior approach for total hip arthroplasty on an orthopaedic table. Clin Orthop Relat Res 441:115–124
Baba T, Shitoto K, Kaneko K (2013) Bipolar hemiarthroplasty for femoral neck fracture using the direct anterior approach. World J Orthop 4(2):85
Restrepo C, Parvizi J, Pour AE, Hozack WJ (2010) Prospective randomized study of two surgical approaches for total hip arthroplasty. J Arthroplasty 25(5):671–679
Seng BE, Berend KR, Ajluni AF, Lombardi AV (2009) Anterior-supine minimally invasive total hip arthroplasty: defining the learning curve. Orthop Clin N Am 40(3):343–350
Woolson ST, Pouliot MA, Huddleston JI (2009) Primary total hip arthroplasty using an anterior approach and a fracture table: short-term results from a community hospital. J Arthroplasty 24(7):999–1005
Poehling-Monaghan KL, Kamath AF, Taunton MJ, Pagnano MW (2015) Direct anterior versus miniposterior THA with the same advanced perioperative protocols: surprising early clinical results. Clin Orthop Relat Res 473(2):623–31
Rodriguez JA, Deshmukh AJ, Rathod PA, Greiz ML, Deshmane PP, Hepinstall MS, Ranawat AS. Does the direct anterior approach in THA offer faster rehabilitation and comparable safety to the posterior approach? Clin Orthop Relat Res 472(2):455–63
Lewinnek GE, Lewis JL, Tarr R, Compere CL, Zimmerman JR (1978) Dislocations after total hip-replacement arthroplasties. J Bone Joint Surg Am 60:217
Widmer KH (2004) A simplified method to determine acetabular cup anteversion from plain radiographs. J Arthroplast 19(3):387–390
Min BW, Song KS, Bae KC, Cho CH, Kang CH, Kim SY (2008) The effect of stem alignment on results of total hip arthroplasty with a cementless tapered-wedge femoral component. J Arthroplast 23(3):418–423
Abe H, Sakai T, Takao M, Nishii T, Nakamura N, Sugano N (2015) Difference in stem alignment between the direct anterior approach and the posterolateral approach in total hip arthroplasty. J Arthroplast 30(10):1761–6
Rathod PA, Bhalla S, Deshmukh AJ, Rodriguez JA (2014) Does fluoroscopy with anterior hip arthoplasty decrease acetabular cup variability compared with a nonguided posterior approach? Clin Orthop Relat Res 472(6):1877–1885
Deshmukh AJ, Rathod PA, Rodriguez JA (2014) Fluoroscopic imaging of acetabular cup position during THA through a direct anterior approach. Orthopedics 37(1):12–12
Epstein NJ, Woolson ST, Giori NJ (2011) Acetabular component positioning using the transverse acetabular ligament: can you find it and does it help? Clin Orthop Relat Res 469:412–416
Nishikubo Y, Fujioka M, Ueshima K, Saito M, Kubo T (2011) Preoperative fluoroscopic imaging reduces variability of acetabular component positioning. J Arthroplast 26(7):1088–1094
Ali Khan MA, Brakenbury PH, Reynolds IS (1981) Dislocation following total hip replacement. J Bone Joint Surg (Br) 63(2):214–8
Jolles BM, Zangger P, Leyvraz PF (2002) Factors predisposing to dislocation after primary total hip arthroplasty: a multivariate analysis. J Arthroplasty 17(3):282–8
McCollum DE, Gray WJ (1990) Dislocation after total hip arthroplasty. Causes and prevention. Clin Orthop Relat Res Dec (261):159–70
Barrack RL, Krempec JA, Clohisy JC, McDonald DJ, Ricci WM, Ruh EL, Nunley RM (2013) Accuracy of acetabular component position in hip arthroplasty. J Bone Joint Surg Am 95(19):1760–1768
Vresilovic EJ, Hozack WJ, Rothman RH (1994) Radiographic assessment of cementless femoral components. Correlation with intraoperative mechanical stability. J Arthroplasty 9:137
Vaughan PD, Singh PJ, Teare R, Kucheria R, Singer GC (2007) Femoral stem tip orientation and surgical approach in total hip arthroplasty. Hip Int 17:212
Khalily C, Lester K (2002) Results of a tapered cementless femoral stem implanted in varus. J Arthroplasty 17:463
McArthur BA, Schueler BA, Howe BM, Trousdale RT, Taunton MJ (2015) Radiation exposure during fluoroscopic guided direct anterior approach for total hip arthroplasty. J Arthroplast 30(9):1565–8
Hirata M, Nakashima Y, Itokawa T, Ohishi M, Sato T, Akiyama M, Hara D, Iwamoto Y (2014) Influencing factors for the increased stem version compared to the native femur in cementless total hip arthroplasty. Int Orthop 38:1341–6
Reichert JC, Volkmann MR, Koppmair M, Rackwitz L, Lüdemann M, Rudert M, Nöth U (2015) Comparative retrospective study of the direct anterior and transgluteal approaches for primary total hip arthroplasty. Int Orthop 39(12):2309–13
Homma Y, Baba T, Sano K, Ochi H, Matsumoto M, Kobayashi H, Yuasa T, Maruyama Y, Kaneko K (2015) Lateral femoral cutaneous nerve injury with the direct anterior approach for total hip arthroplasty. Int Orthop. Jul 30. [Epub ahead of print]
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Kobayashi, H., Homma, Y., Baba, T. et al. Surgeons changing the approach for total hip arthroplasty from posterior to direct anterior with fluoroscopy should consider potential excessive cup anteversion and flexion implantation of the stem in their early experience. International Orthopaedics (SICOT) 40, 1813–1819 (2016). https://doi.org/10.1007/s00264-015-3059-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-015-3059-1