
Abstract
Purpose
The purpose of this study was to evaluate whether the bone morphology of the hip affects the range of motion (ROM) in total hip arthroplasty (THA).
Methods
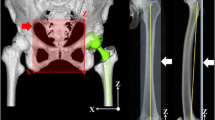
Using the CT data of 63 patients who underwent THA, we calculated the ROM of flexion (Flex), internal rotation (Int-R) and external rotation (Ext-R) using 3D dynamic analysis software. We measured the distance between the anterior surface of the stem and anterior aspect of the greater trochanter (GTa length) at the cutting point and between the tip of the antero-inferior iliac spine (AIIS) and coronal plane of both femoral heads (AIIS length), as a parameter of the femur and pelvis, respectively. The relationship between the ROM, bone anatomy and impingement site was evaluated.
Results
We found a significant decrease in the ROM of Flex and the Int-R to be inversely proportional to the GTa and AIIS length. In Flex and Int-R, the anterior intertrochanteric region often impinges on the AIIS in patients with larger bone anatomy.
Conclusions
We demonstrated that the bone morphology of the hip substantially affects the ROM of Flex and Int-R, especially in patients with large bone anatomy. For these patients we should consider bony impingement in THA.





Similar content being viewed by others


References
Courpied JP, Caton JH (2011) Total hip arthroplasty, state of the art for the 21st century. Int Orthop 35:149–150
D’Lima DD, Urquhart AG, Buehler KO, Walker RH, Colwell CW Jr (2000) The effect of the orientation of the acetabular and femoral components on the range of motion of the hip at different head–neck ratios. J Bone Joint Surg Am 82:315–321
Nadzadi ME, Pedersen DR, Yack HJ, Callaghan JJ, Brown TD (2003) Kinematics, kinetics, and finite element analysis of commonplace maneuvers at risk for total hip dislocation. J Biomech 36(5):77–91
Caton J, Prudhon JL (2011) Over 25 years survival after Charnley’s total hip arthroplasty. Int Orthop 35:185–188
Morrey BF (1997) Difficult complications after hip joint replacement. Dislocation. Clin Orthop Relat Res 344:179–187
Jolles BM, Zangger P, Leyvraz PF (2002) Factors predisposing to dislocation after primary total hip arthroplasty. A multivariate analysis. J Arthroplasty 17:282–288
Bartz RL, Nobel PC, Kadakia NR, Tullos HS (2000) The effect of femoral component head size on posterior dislocation of the artificial hip joint. J Bone Joint Surg Am 82:1300–1307
Heithoff BE (2001) Dislocation after total hip arthroplasty: a single surgeon’s experience. Orthop Clin North Am 32:587–591
Malik A, Maheshwari A, Dorr LD (2007) Impingement with total hip replacement. J Bone Joint Surg Am 89:1832–1842
Crowninshield RD, Maloney WJ, Wentz DH, Humphrey SM, Blanchard CR (2004) Biomechanics of large femoral heads: what they do and don’t do. Clin Orthop 429:102–107
Widmer KH, Zurfluh B (2004) Compliant positioning of total hip components for optimal range of motion. J Orthop Res 22:815–821
Kessler O, Patil S, Stefan W, Mayr E, Colwell CW, D’Lima DD (2008) Bony impingement affects range of motion after total hip arthroplasty: a subject-specific approach. J Orthop Res 26:443–452
Rousseau MA, Lazennec JY, Boyer P, Mora N, Gorin M, Catonné Y (2009) Optimization of total hip arthroplasty implantation: is the anterior pelvic plane concept valid? J Arthroplasty 24:22–26
Incavo SJ, Thompson MT, Gold JE, Patel RV, Icenogle KD, Noble PC (2011) Which procedure better restores intact hip range of motion: total hip arthroplasty or resurfacing? A combined cadaveric and computer simulation study. J Arthroplasty 26:391–397
Tsukeoka T, Hyun Lee T (2012) Sagittal flexion of the femoral component affects flexion gap and sizing in total knee arthroplasty. J Arthroplasty 27:1094–1099
Lachiewicz PF, Soileau ES (2013) Low early and late dislocation rates with 36- and 40-mm heads in patients at high risk for dislocation. Clin Orthop Relat Res 471:439–443
Garbuz DS, Masri BA, Duncan CP, Greidanus NV, Bohm ER, Petrak MJ, Della Valle CJ, Gross AE (2012) Dislocation in revision THA: do large heads (36 and 40 mm) result in reduced dislocation rates in a randomized clinical trial? Clin Orthop Relat Res 470:351–356
Rodriguez JA, Rathod PA (2012) Large diameter heads: is bigger always better? J Bone Joint Surg Br 94(11 Suppl A):52–54
Suzuki K, Matsubara M, Morita S, Muneta T, Shinomiya K (2002) CT image evaluation of the internal rotation limit prior to bony impingement after total hip arthroplasty. J Orthop Sci 7:433–438
Dorr LD, Wan Z (1998) Causes of and treatment protocol for instability of total hip replacement. Clin Orthop Relat Res 335:144–151
Dorr LD, Wolf AW, Chandler R, Conaty JP (1983) Classification and treatment of dislocations of total hip arthroplasty. Clin Orthop Relat Res 173:151–158
Lewinnek GE, Lewis JL, Tarr R, Compere CL, Zimmerman JR (1978) Dislocations after total hip-replacement arthroplasties. J Bone Joint Surg Am 60:217–220
Burroughs BR, Hallstrom B, Golladay GJ, Hoeffel D, Harris WH (2005) Range of motion and stability in total hip arthroplasty with 28-, 32-, 38-, and 44-mm femoral head sizes. J Arthroplasty 20:11–19
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Shoji, T., Yasunaga, Y., Yamasaki, T. et al. Bony impingement depends on the bone morphology of the hip after total hip arthroplasty. International Orthopaedics (SICOT) 37, 1897–1903 (2013). https://doi.org/10.1007/s00264-013-1979-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-013-1979-1