
Abstract
Purpose
To evaluate the diagnostic performance of a simulated twin-phase pancreatic protocol CT generated from a single portal venous phase (PVP) dual-energy CT (DECT) acquisition in patients with pancreatic ductal adenocarcinoma (PDAC).
Methods
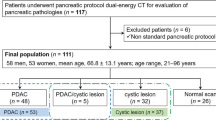
In this retrospective study, we included 63 patients with PDAC who underwent pancreatic protocol (pancreatic phase [PP] and PVP) DECT. Two data sets were created from this original acquisition—(1) Standard protocol (50 keV PP/65 keV PVP) and (2) Simulated protocol (40 keV/65 keV PVP). Using a 5-point scale, three readers scored image quality, tumor conspicuity, and arterial involvement by the PDAC. Signal-to-noise ratio (SNR) of the pancreas and tumor-to-pancreas contrast-to-noise ratio (CNR) were calculated. Qualitative scores, quantitative parameters, and radiation dose were compared between standard and simulated protocols.
Results
No significant difference in detection rate of PDAC was seen between the standard (58/63, 92.1%) and simulated protocols (56/63, 88.9%) (P = 0.76). Subjective scoring for arterial involvement for celiac (P = 0.86), superior mesenteric (P = 0.88), splenic (P = 0.86), common hepatic (P = 0.52), gastroduodenal (P = 0.95), first jejunal (P = 0.48) arteries, and aorta (P = 1.00) were comparable between two protocols. The image quality (P = 0.14), the SNR of the pancreas (P = 0.15), and CNR (P = 0.54) were comparable between two protocols. The projected mean dose-length product (DLP) (629.6 ± 148.3 mGy cm) in the simulated protocol showed a 44% reduction in radiation dose compared to the standard protocol (mean DLP, 1123.3 ± 268.9 mGy cm) (P < 0.0001).
Conclusions
Low keV images generated from a PVP DECT acquisition allows creation of a twin-phase pancreatic protocol CT with comparable diagnostic accuracy for detecting PDAC with significant reduction in radiation dose. Reduced radiation dose is desirable in surveillance and screening for pancreatic diseases.



Similar content being viewed by others


Abbreviations
- ASiR:
-
Adaptive statistical iterative reconstruction
- CNR:
-
Tumor-to-pancreas contrast-to-noise ratio
- CT:
-
Computed tomography
- DECT:
-
Dual-energy computed tomography
- DLP:
-
Dose-length product
- PDAC:
-
Pancreatic ductal adenocarcinoma
- PP:
-
Pancreatic phase
- PVP:
-
Portal venous phase
- SNR:
-
Signal-to-noise ratio
References
Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res 2014; 74:2913-2921
Klauss M, Schobinger M, Wolf I, et al. Value of three-dimensional reconstructions in pancreatic carcinoma using multidetector CT: initial results. World J Gastroenterol 2009; 15:5827-5832
NCCN clinical practice guidelines in oncology: pancreatic adenocarcinoma, version 3. 2019. https://www.nccnorg/professionals/physiciangls/pdf/pancreaticpdf;
Kulkarni NM, Soloff EV, Tolat PP, et al. White paper on pancreatic ductal adenocarcinoma from society of abdominal radiology's disease-focused panel for pancreatic ductal adenocarcinoma: Part I, AJCC staging system, NCCN guidelines, and borderline resectable disease. Abdom Radiol (NY) 2020; 45:716-728
Kulkarni NM, Hough DM, Tolat PP, Soloff EV, Kambadakone AR. Pancreatic adenocarcinoma: cross-sectional imaging techniques. Abdom Radiol (NY) 2018; 43:253-263
Singhi AD, Koay EJ, Chari ST, Maitra A. Early Detection of Pancreatic Cancer: Opportunities and Challenges. Gastroenterology 2019; 156:2024-2040
Noda Y, Goshima S, Kaga T, et al. Virtual monochromatic image at lower energy level for assessing pancreatic ductal adenocarcinoma in fast kV-switching dual-energy CT. Clin Radiol 2019;
Ohira S, Kanayama N, Wada K, et al. A Third-Generation Adaptive Statistical Iterative Reconstruction for Contrast-Enhanced 4-Dimensional Dual-Energy Computed Tomography for Pancreatic Cancer. J Comput Assist Tomogr 2019;
Aslan S, Camlidag I, Nural MS. Lower energy levels and iodine-based material decomposition images increase pancreatic ductal adenocarcinoma conspicuity on rapid kV-switching dual-energy CT. Abdom Radiol (NY) 2019; 44:568-575
Apfaltrer P, Sudarski S, Schneider D, et al. Value of monoenergetic low-kV dual energy CT datasets for improved image quality of CT pulmonary angiography. Eur J Radiol 2014; 83:322-328
Brook OR, Gourtsoyianni S, Brook A, Siewert B, Kent T, Raptopoulos V. Split-bolus spectral multidetector CT of the pancreas: assessment of radiation dose and tumor conspicuity. Radiology 2013; 269:139-148
Camacho A, Fang J, Cohen MP, Raptopoulos V, Brook OR. Split-bolus pancreas CTA protocol for local staging of pancreatic cancer and detection and characterization of liver lesions. Abdom Radiol (NY) 2018; 43:340-350
Noda Y, Goshima S, Kozaka K, et al. Optimal window settings in single-source dual-energy computed tomography of the abdomen. Eur J Radiol 2018; 109:204-209
Noda Y, Goshima S, Takai Y, et al. Detection of pancreatic ductal adenocarcinoma and liver metastases: comparison of Gd-EOB-DTPA-enhanced MR imaging vs. extracellular contrast materials. Abdom Radiol (NY) 2020; 45:2459–2468
Noda Y, Goshima S, Koyasu H, et al. Renovascular CT: comparison between adaptive statistical iterative reconstruction and model-based iterative reconstruction. Clin Radiol 2017; 72:901 e913–901 e919
Hong SB, Lee SS, Kim JH, et al. Pancreatic Cancer CT: Prediction of Resectability according to NCCN Criteria. Radiology 2018; 289:710-718
Al-Hawary MM, Francis IR, Chari ST, et al. Pancreatic ductal adenocarcinoma radiology reporting template: consensus statement of the Society of Abdominal Radiology and the American Pancreatic Association. Radiology 2014; 270:248-260
Uhrig M, Simons D, Kachelriess M, Pisana F, Kuchenbecker S, Schlemmer HP. Advanced abdominal imaging with dual energy CT is feasible without increasing radiation dose. Cancer Imaging 2016; 16:15
Noda Y, Goshima S, Miyoshi T, et al. Determination of the least amount of iodine load required for the detection of pancreatic adenocarcinoma at 80-kVp CT. Eur J Radiol 2016; 85:901-905
Christner JA, Kofler JM, McCollough CH. Estimating effective dose for CT using dose-length product compared with using organ doses: consequences of adopting International Commission on Radiological Protection publication 103 or dual-energy scanning. AJR Am J Roentgenol 2010; 194:881-889
Noda Y, Goshima S, Kaga T, et al. Virtual monochromatic image at lower energy level for assessing pancreatic ductal adenocarcinoma in fast kV-switching dual-energy CT. Clin Radiol 2020; 75:320 e317–320 e323
Yin Q, Zou X, Zai X, et al. Pancreatic ductal adenocarcinoma and chronic mass-forming pancreatitis: Differentiation with dual-energy MDCT in spectral imaging mode. Eur J Radiol 2015; 84:2470-2476
Gupta S, Wagner-Bartak N, Jensen CT, et al. Dual-energy CT of pancreatic adenocarcinoma: reproducibility of primary tumor measurements and assessment of tumor conspicuity and margin sharpness. Abdom Radiol (NY) 2016; 41:1317-1324
Wu R, Watanabe Y, Satoh K, et al. Quantitative Comparison of Virtual Monochromatic Images of Dual Energy Computed Tomography Systems: Beam Hardening Artifact Correction and Variance in Computed Tomography Numbers: A Phantom Study. J Comput Assist Tomogr 2018; 42:648-654
Sugawara H, Suzuki S, Katada Y, et al. Comparison of full-iodine conventional CT and half-iodine virtual monochromatic imaging: advantages and disadvantages. Eur Radiol 2019; 29:1400-1407
Sugawara H, Takayanagi T, Ishikawa T, et al. New Fast kVp Switching Dual-Energy CT: Reduced Severity of Beam Hardening Artifacts and Improved Image Quality in Reduced-Iodine Virtual Monochromatic Imaging. Acad Radiol 2019;
Han WK, Na JC, Park SY. Low-dose CT angiography using ASiR-V for potential living renal donors: a prospective analysis of image quality and diagnostic accuracy. Eur Radiol 2020; 30:798-805
Tang H, Liu Z, Hu Z, et al. Clinical value of a new generation adaptive statistical iterative reconstruction (ASIR-V) in the diagnosis of pulmonary nodule in low-dose chest CT. Br J Radiol 2019; 92:20180909
Chen Y, Liu Z, Li M, et al. Reducing both radiation and contrast doses in coronary CT angiography in lean patients on a 16-cm wide-detector CT using 70 kVp and ASiR-V algorithm, in comparison with the conventional 100-kVp protocol. Eur Radiol 2019; 29:3036-3043
Chen LH, Jin C, Li JY, et al. Image quality comparison of two adaptive statistical iterative reconstruction (ASiR, ASiR-V) algorithms and filtered back projection in routine liver CT. Br J Radiol 2018; 91:20170655
Tamm EP, Loyer EM, Faria SC, Evans DB, Wolff RA, Charnsangavej C. Retrospective analysis of dual-phase MDCT and follow-up EUS/EUS-FNA in the diagnosis of pancreatic cancer. Abdom Imaging 2007; 32:660-667
DeWitt J, Devereaux B, Chriswell M, et al. Comparison of endoscopic ultrasonography and multidetector computed tomography for detecting and staging pancreatic cancer. Ann Intern Med 2004; 141:753-763
1990 Recommendations of the International Commission on Radiological Protection. Ann ICRP 1991; 21:1-201
Kanal KM, Butler PF, Sengupta D, Bhargavan-Chatfield M, Coombs LP, Morin RL. U.S. Diagnostic Reference Levels and Achievable Doses for 10 Adult CT Examinations. Radiology 2017; 284:120-133
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
AK: Grant support for research activities from Philips, GE Healthcare, and PanCAN. Other authors report no relevant disclosures or conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Noda, Y., Tochigi, T., Parakh, A. et al. Simulated twin-phase pancreatic CT generated using single portal venous phase dual-energy CT acquisition in pancreatic ductal adenocarcinoma. Abdom Radiol 46, 2610–2619 (2021). https://doi.org/10.1007/s00261-020-02921-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00261-020-02921-9