
Abstract
Purpose
3′-Deoxy-3′-18F-fluorothymidine (FLT) positron emission tomography (PET) has limited utility in abdominal imaging due to high physiological hepatic uptake of tracer. We evaluated FLT PET/CT combined with a temporal-intensity information-based voxel-clustering approach termed kinetic spatial filtering (FLT PET/CTKSF) for early prediction of response and survival outcomes in locally advanced and metastatic pancreatic cancer patients receiving gemcitabine-based chemotherapy.
Methods
Dynamic FLT PET/CT data were collected before and 3 weeks after the first cycle of chemotherapy. Changes in tumour FLT PET/CT variables were determined. The primary end point was RECIST 1.1 response on contrast-enhanced CT after 3 months of therapy.
Results
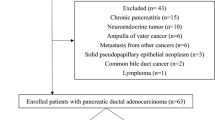
Twenty patients were included. Visual distinction between tumours and normal pancreas was seen in FLT PETKSF images. All target lesions (>2 cm), including all primary pancreatic tumours, were visualised. Of the 11 liver metastases, 3 (<2 cm) were not visible after kinetic filtering. Of the 20 patients, 7 progressed (35 %). Maximum standardised uptake value at 60 min post-injection (SUV60,max) significantly increased in patients with disease progression (p = 0.04). Receiver-operating characteristic curve analysis indicated that a threshold of SUV60,max increase of ≥ 12 % resulted in sensitivity, specificity and positive predictive value (PPV) of 71, 100 and 100 %, respectively [area under the curve (AUC) 0.90, p = 0.0001], to predict patients with disease progression. Changes in SUV60,max were not predictive of survival.
Conclusion
FLT PET/CT detected changes in proliferation, with early increase in SUV60,max predicting progressive disease with a high specificity and PPV. Therefore, FLT PET/CT could be used as an early response biomarker for gemcitabine-based chemotherapy, to select a poor prognostic group who may benefit from novel therapeutic agents in advanced and metastatic pancreatic cancer.



Similar content being viewed by others


References
Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin 2012;62:10–29. doi:10.3322/caac.20138.
Cartwright T, Richards DA, Boehm KA. Cancer of the pancreas: are we making progress? A review of studies in the US Oncology Research Network. Cancer Control 2008;15:308–13.
Sultana A, Smith CT, Cunningham D, Starling N, Neoptolemos JP, Ghaneh P. Meta-analyses of chemotherapy for locally advanced and metastatic pancreatic cancer. J Clin Oncol 2007;25:2607–15. doi:10.1200/JCO.2006.09.2551.
Ciliberto D, Botta C, Correale P, Rossi M, Caraglia M, Tassone P, et al. Role of gemcitabine-based combination therapy in the management of advanced pancreatic cancer: a meta-analysis of randomised trials. Eur J Cancer 2013;49:593–603. doi:10.1016/j.ejca.2012.08.019.
Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer 2009;45:228–47. doi:10.1016/j.ejca.2008.10.026.
Costello E, Greenhalf W, Neoptolemos JP. New biomarkers and targets in pancreatic cancer and their application to treatment. Nat Rev Gastroenterol Hepatol 2012;9:435–44. doi:10.1038/nrgastro.2012.119.
Zhu A, Lee D, Shim H. Metabolic positron emission tomography imaging in cancer detection and therapy response. Semin Oncol 2011;38:55–69. doi:10.1053/j.seminoncol.2010.11.012.
Choi M, Heilbrun LK, Venkatramanamoorthy R, Lawhorn-Crews JM, Zalupski MM, Shields AF. Using 18F-fluorodeoxyglucose positron emission tomography to monitor clinical outcomes in patients treated with neoadjuvant chemo-radiotherapy for locally advanced pancreatic cancer. Am J Clin Oncol 2010;33:257–61. doi:10.1097/COC.0b013e3181a76a0b.
Kuwatani M, Kawakami H, Eto K, Haba S, Shiga T, Tamaki N, et al. Modalities for evaluating chemotherapeutic efficacy and survival time in patients with advanced pancreatic cancer: comparison between FDG-PET, CT, and serum tumor markers. Intern Med 2009;48:867–75.
Rose DM, Delbeke D, Beauchamp RD, Chapman WC, Sandler MP, Sharp KW, et al. 18Fluorodeoxyglucose-positron emission tomography in the management of patients with suspected pancreatic cancer. Ann Surg 1999;229:729–37. discussion 37–8.
Bang S, Chung HW, Park SW, Chung JB, Yun M, Lee JD, et al. The clinical usefulness of 18-fluorodeoxyglucose positron emission tomography in the differential diagnosis, staging, and response evaluation after concurrent chemoradiotherapy for pancreatic cancer. J Clin Gastroenterol 2006;40:923–9. doi:10.1097/01.mcg.0000225672.68852.05.
Buck AC, Schirrmeister HH, Guhlmann CA, Diederichs CG, Shen C, Buchmann I, et al. Ki-67 immunostaining in pancreatic cancer and chronic active pancreatitis: does in vivo FDG uptake correlate with proliferative activity? J Nucl Med 2001;42:721–5.
Higashi T, Saga T, Nakamoto Y, Ishimori T, Fujimoto K, Doi R, et al. Diagnosis of pancreatic cancer using fluorine-18 fluorodeoxyglucose positron emission tomography (FDG PET)–usefulness and limitations in "clinical reality". Ann Nucl Med 2003;17:261–79.
Klein WM, Hruban RH, Klein-Szanto AJ, Wilentz RE. Direct correlation between proliferative activity and dysplasia in pancreatic intraepithelial neoplasia (PanIN): additional evidence for a recently proposed model of progression. Mod Pathol 2002;15:441–7. doi:10.1038/modpathol.3880544.
van Waarde A, Cobben DC, Suurmeijer AJ, Maas B, Vaalburg W, de Vries EF, et al. Selectivity of 18F-FLT and 18F-FDG for differentiating tumor from inflammation in a rodent model. J Nucl Med 2004;45:695–700.
Barwick T, Bencherif B, Mountz JM, Avril N. Molecular PET and PET/CT imaging of tumour cell proliferation using F-18 fluoro-L-thymidine: a comprehensive evaluation. Nucl Med Commun 2009;30:908–17. doi:10.1097/MNM.0b013e32832ee93b.
Quon A, Chang ST, Chin F, Kamaya A, Dick DW, Loo Jr BW, et al. Initial evaluation of 18F-fluorothymidine (FLT) PET/CT scanning for primary pancreatic cancer. Eur J Nucl Med Mol Imaging 2008;35:527–31. doi:10.1007/s00259-007-0630-z.
Herrmann K, Eckel F, Schmidt S, Scheidhauer K, Krause BJ, Kleeff J, et al. In vivo characterization of proliferation for discriminating cancer from pancreatic pseudotumors. J Nucl Med 2008;49:1437–44. doi:10.2967/jnumed.108.052027.
Herrmann K, Erkan M, Dobritz M, Schuster T, Siveke JT, Beer AJ, et al. Comparison of 3'-deoxy-3'-[(18)F]fluorothymidine positron emission tomography (FLT PET) and FDG PET/CT for the detection and characterization of pancreatic tumours. Eur J Nucl Med Mol Imaging 2012;39:846–51. doi:10.1007/s00259-012-2061-8.
Shields AF, Grierson JR, Muzik O, Stayanoff JC, Lawhorn-Crews JM, Obradovich JE, et al. Kinetics of 3'-deoxy-3'-[F-18]fluorothymidine uptake and retention in dogs. Mol Imaging Biol 2002;4:83–9.
Zasadny KR, Wahl RL. Enhanced FDG-PET tumor imaging with correlation-coefficient filtered influx-constant images. J Nucl Med 1996;37:371–4.
Contractor K, Challapalli A, Tomasi G, Rosso L, Wasan H, Stebbing J, et al. Imaging of cellular proliferation in liver metastasis by [18F]fluorothymidine positron emission tomography: effect of therapy. Phys Med Biol 2012;57:3419–33. doi:10.1088/0031-9155/57/11/3419.
Gray KR, Contractor KB, Kenny LM, Al-Nahhas A, Shousha S, Stebbing J, et al. Kinetic filtering of [(18)F]Fluorothymidine in positron emission tomography studies. Phys Med Biol 2010;55:695–709. doi:10.1088/0031-9155/55/3/010.
Cleij MC, Steel CJ, Brady F, Ell PJ, Pike VW, Luthra SK. An improved synthesis of 3′-deoxy-3′-[18F]fluorothymidine ([18F]FLT) and the fate of the precursor 2,3′-anhydro-5′-O-(4,4′-dimethoxytrityl)-thymidine. J Label Compd Radiopharm 2001;44:S871–3.
Contractor KB, Kenny LM, Stebbing J, Rosso L, Ahmad R, Jacob J, et al. [18F]-3'Deoxy-3'-fluorothymidine positron emission tomography and breast cancer response to docetaxel. Clin Cancer Res 2011;17:7664–72. doi:10.1158/1078-0432.CCR-11-0783.
Wahl RL, Jacene H, Kasamon Y, Lodge MA. From RECIST to PERCIST: evolving considerations for PET response criteria in solid tumors. J Nucl Med 2009;50 Suppl 1:122S–50S. doi:10.2967/jnumed.108.057307.
de Langen AJ, Klabbers B, Lubberink M, Boellaard R, Spreeuwenberg MD, Slotman BJ, et al. Reproducibility of quantitative 18F-3'-deoxy-3'-fluorothymidine measurements using positron emission tomography. Eur J Nucl Med Mol Imaging 2009;36:389–95. doi:10.1007/s00259-008-0960-5.
Kenny L, Coombes RC, Vigushin DM, Al-Nahhas A, Shousha S, Aboagye EO. Imaging early changes in proliferation at 1 week post chemotherapy: a pilot study in breast cancer patients with 3'-deoxy-3'-[18F]fluorothymidine positron emission tomography. Eur J Nucl Med Mol Imaging 2007;34:1339–47. doi:10.1007/s00259-007-0379-4.
Tehrani OS, Shields AF. PET imaging of proliferation with pyrimidines. J Nucl Med 2013;54:903–12. doi:10.2967/jnumed.112.112201.
Weber WA. Monitoring tumor response to therapy with 18F-FLT PET. J Nucl Med 2010;51:841–4. doi:10.2967/jnumed.109.071217.
Farrell JJ, Elsaleh H, Garcia M, Lai R, Ammar A, Regine WF, et al. Human equilibrative nucleoside transporter 1 levels predict response to gemcitabine in patients with pancreatic cancer. Gastroenterology 2009;136:187–95. doi:10.1053/j.gastro.2008.09.067.
Paproski RJ, Young JD, Cass CE. Predicting gemcitabine transport and toxicity in human pancreatic cancer cell lines with the positron emission tomography tracer 3'-deoxy-3'-fluorothymidine. Biochem Pharmacol 2010;79:587–95. doi:10.1016/j.bcp.2009.09.025.
Dittmann H, Dohmen BM, Kehlbach R, Bartusek G, Pritzkow M, Sarbia M, et al. Early changes in [18F]FLT uptake after chemotherapy: an experimental study. Eur J Nucl Med Mol Imaging 2002;29:1462–9. doi:10.1007/s00259-002-0925-z.
Contractor KB, Kenny LM, Stebbing J, Challapalli A, Al-Nahhas A, Palmieri C, et al. Biological basis of [11C]choline-positron emission tomography in patients with breast cancer: comparison with [18F]fluorothymidine positron emission tomography. Nucl Med Commun 2011;32:997–1004. doi:10.1097/MNM.0b013e328349567b.
Acknowledgments
The authors would like to thank Ms. Kozlowski for patient recruitment and editorial assistance and Dr. Petrides for reviewing the NUTH scans for incidental findings. We also thank the radiographers, radiochemists, blood lab staff and finally all the patients who have taken part in this study.
Compliance with ethical standards
ᅟ
Funding
This study was supported by UK Medical Research Council (MRC) grant MC-A652-5PY80, Joint Cancer Research-UK (CRUK) and Engineering and Physical Sciences Research Council Cancer Imaging Centre, Imperial College London (ICL), in association with MRC and Department of Health grant C2536/A10337, Experimental Cancer Medicine Centres' grant C37/A7283 and National Institute for Health Research Biomedical Research Centre award to Imperial College Healthcare NHS Trust and ICL. In Newcastle it was supported by CRUK Award C29821/A10348.
Conflicts of interest
None.
Ethical approval
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Statement on welfare of animals
This article does not contain any studies with animals performed by any of the authors.
Informed consent
Informed consent was obtained from all individual participants included in this study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Amarnath Challapalli and Tara Barwick contributed equally to this work and are joint first authors.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Online Resource 1
Performance of KSF in patients scanned at ICHNT and NUTH (a, b) and decay-corrected time-activity curves, normalised by injected activity (tissue activity) of the three liver metastases not visualised on KSF (c). Data are average tissue activity values and error bars represent one SD. Average reduction in SUV in the primary tumours (a) was 18 % and in the liver metastases (b) was 28 %. (GIF 27 kb)
Online Resource 2
Voxel representations depicting tumour heterogeneity, in pancreatic tumours (a, b) and liver metastases (c, d) in a tumours of size < 30 mm (homogeneous tumour on filtered images) and in a tumour of size > 55 mm (heterogeneous tumour on filtered images). The dotted line on the X-axis corresponds to SUV of 2. Note different scales of Y-axis. (GIF 34 kb)
Online Resource 3
Changes in voxel intensities with therapy, in pancreatic tumour (a, b) and liver metastases (c, d) in an NP and P, respectively. The dotted line on the X-axis corresponds to SUV 2. Note different scales of Y-axis. (GIF 38 kb)
Online Resource 4
Waterfall plots (a) and box and whisker plots (b) of summed lesions for measures of HiVox showing some degree of reduction in the HiVox, but no significant changes in the HiVox between NP and P on group analysis of the data. (GIF 18 kb)
Online Resource 5
Changes in imaging variables, application of KSF and influence of single agent gemcitabine or combination chemotherapy. There was no difference in response with single agent vs combination chemotherapy. NP non-progressors (patients with PR or SD), P progressors. (GIF 44 kb)
Online Resource 6
Group analysis of the imaging data showing the difference between baseline and post-treatment histogram parameters in the summed lesions in non-progressors (NP) and progressors (P): box and whisker plots for the measures of median (a), mode (b), skewness (c), kurtosis (d), 10th (e), 90th (f), 50th (g) and 75th (h) percentiles . Note different scales of Y-axis. (GIF 47 kb)
Online Resource 7
Group analysis of imaging data showing the difference between baseline and post-treatment FLT uptake in the summed lesions in non-progressors (NP) and progressors (P): box and whisker plots for the measures of a SUV60,ave and b SUV60,max. Note different scales of Y-axis. * denotes p < 0.05 (GIF 40 kb)
Online Resource 8
Expression of hENT1 (a) and Ki-67 (b) in pancreatic cancer by immunohistochemistry. Representative section of a case of pancreatic cancer showing high expression of hENT1 with a diffuse cytoplasmic and nuclear pattern is seen in a. A representative case showing moderate expression of Ki-67 nuclear expression in pancreatic cancer is shown in b. Magnification ×400. (PPT 229 kb)
ESM 9
(DOCX 27 kb)
Rights and permissions
About this article

Cite this article
Challapalli, A., Barwick, T., Pearson, R.A. et al. 3′-Deoxy-3′-18F-fluorothymidine positron emission tomography as an early predictor of disease progression in patients with advanced and metastatic pancreatic cancer. Eur J Nucl Med Mol Imaging 42, 831–840 (2015). https://doi.org/10.1007/s00259-015-3000-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-015-3000-2