
Abstract
Objective
To suggest different ultrasound-guided steroid injection (USI) techniques based on anatomical variations of the first extensor compartment (FEC), and to evaluate the usefulness of it, in patients with de Quervain’s disease.
Materials and methods
Twenty-eight patients who underwent USI for de Quervain’s disease were included. Anatomical variations were classified into complete sub-compartmentalization (n = 11), distal incomplete sub-compartmentalization (n = 5), and no sub-compartmentalization (n = 12) on ultrasound. Involved sub-compartments were recorded in patients with complete sub-compartmentalization. USIs were performed based on the anatomical variations: in both sub-compartments (n = 2) or only in the affected sub-compartment (n = 9) depending on the location of tenosynovitis involvement, in patients with complete sub-compartmentalization; in proximal FEC in patients with distal incomplete sub-compartmentalization (n = 5); in the common compartment in patients with no sub-compartmentalization (n = 12). Medical charts were retrospectively reviewed for evaluation of clinical outcome at follow-up visits.
Results
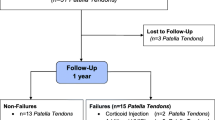
Twenty-three out of 28 patients were followed up with a mean period of 31.2 days after injection (6~87 days). Mean VAS was 7.96 before injection (range: 4 to 10), which was significantly reduced to 0.65 at rest and 1.57 during activity at follow-up visits (p < 0.05). Twenty-two out of 23 patients were satisfied with the results. The mean proportion of subjective pain reduction was 82.0% (median 95%).
Conclusion
Ultrasound-guided steroid injections using different injection techniques based on the anatomical variations of the FEC have shown to be beneficial in the management of de Quervain’s disease.




Similar content being viewed by others

References
Keyes HB. Stenosing tendovaginitis at the radial styloid process. Ann Surg. 1938;107(4):602–6.
Jeyapalan K, Choudhary S. Ultrasound-guided injection of triamcinolone and bupivacaine in the management of de Quervain’s disease. Skeletal Radiol. 2009;38(11):1099–103.
Altay MA, Erturk C, Isikan UE. De Quervain’s disease treatment using partial resection of the extensor retinaculum: a short-term results survey. Orthop Traumatol Surg Res. 2011;97(5):489–93.
Ta KT, Eidelman D, Thomson JG. Patient satisfaction and outcomes of surgery for de Quervain’s tenosynovitis. J Hand Surg Am. 1999;24(5):1071–7.
Di Sante L, Martino M, Manganiello I, Manganiello I, Santilli V. Ultrasound-guided corticosteroid injection for the treatment of de Quervain’s tenosynovitis. Am J Phys Med Rehabil. 2014;93(3):278.
McDermott JD, Ilyas AM, Nazarian LN, Leinberry CF. Ultrasound-guided injections for de Quervain’s tenosynovitis. Clin Orthop Relat Res. 2012;470(7):1925–31.
Zingas C, Failla JM, Van Holsbeeck M. Injection accuracy and clinical relief of de Quervain’s tendonitis. J Hand Surg Am. 1998;23(1):89–96.
McKenzie JM. Conservative treatment of de Quervain’s disease. Br Med J. 1972;4(5841):659–60.
Danda RS, Kamath J, Jayasheelan N, Kumar P. Role of guided ultrasound in the treatment of De Quervain tenosynovitis by local steroid infiltration. J Hand Microsurg. 2016;8(1):34–7.
Kume K, Amano K, Yamada S, Amano K, Kuwaba N, Ohta H. In de Quervain’s with a separate EPB compartment, ultrasound-guided steroid injection is more effective than a clinical injection technique: a prospective open-label study. J Hand Surg Eur Vol. 2012;37(6):523–7.
Jackson WT, Veigas SF, Coon TM, Stimpson KD, Frogameni AD, Simpson JM. Anatomic variations in the first extensor compartment of the wrist. J Bone Joint Surg Am. 1986;68(6):923–6.
Keon-Cohen B. De Quervain’s disease. J Bone Joint Surg Br. 1951;33-B(1):96–9.
De LL. Quervain’s disease—a clinical and anatomical study. J Bone Joint Surg Am. 1958;40-A(5):1063–70.
Minamikawa Y, Peimer CA, Cox WL, Sherwin FS. De Quervain’s syndrome—surgical and anatomical studies of the fibroosseous canal. Orthopedics. 1991;14(5):545–9.
Choi SJ, Ahn JH, Lee YJ, et al. De Quervain disease: US identification of anatomic variations in the first extensor compartment with an emphasis on sub-compartmentalization. Radiology. 2011;260(2):480–6.
Leslie BM, Ericson WB Jr, Morehead JR. Incidence of a septum within the first dorsal compartment of the wrist. J Hand Surg Am. 1990;15(1):88–91.
Hajder E, de Jonge MC, van der Horst CM, Obdeijn MC. The role of ultrasound-guided triamcinolone injection in the treatment of de Quervain’s disease: treatment and a diagnostic tool? Chir Main. 2013;32(6):403–7.
De Keating-Hart E, Touchais S, Kerjean Y, Ardouin L, Le Goff B. Presence of an intracompartmental septum detected by ultrasound is associated with the failure of ultrasound-guided steroid injection in de Quervain’s syndrome. J Hand Surg Eur Vol. 2016;41(2):212–9.
Kamel M, Moghazy K, Eid H, Mansour R. Ultrasonographic diagnosis of de Quervain’s tenosynovitis. Ann Rheum Dis. 2002;61(11):1034–5.
Orlandi D, Corazza A, Fabbro E, et al. Ultrasound-guided percutaneous injection to treat de Quervain’s disease using three different techniques: a randomized controlled trial. Eur Radiol. 2015;25(5):1512–9.
Yuasa K, Kiyoshige Y. Limited surgical treatment of de Quervain’s disease: decompression of only the extensor pollicis brevis sub-compartment. J Hand Surg Am. 1998;23(5):840–3.
Motoura H, Shiozaki K, Kawasaki K. Anatomical variations in the tendon sheath of the first compartment. Anat Sci Int. 2010;85(3):145–51.
Gilers KW. Anatomical variations affecting the surgery of de Quervain’s disease. Bone Joint Surg Br. 1960;42-B:352–5.
Rousset P, Vuillemin-Bodaghi V, Laredo JD, Parlier-Cuau C. Anatomic variations in the first extensor compartment of the wrist: accuracy of US. Radiology. 2010;257(2):427–33.
Kwon BC, Choi SJ, Koh SH, Shin DJ, Baek GH. Sonographic identification of the intracompartmental septum in de Quervain’s disease. Clin Orthop Relat Res. 2010;468(8):2129–34.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Conflicts of interest
The authors declare that they have no conflicts of interest.
Informed consent
The requirement for written informed consent was waived by the Institutional Review Board for this retrospective review.
Ethical approval
This study was approved by the institutional review board, which waived the requirement for informed patient consent.
Rights and permissions
About this article

Cite this article
Bing, JH., Choi, SJ., Jung, SM. et al. Ultrasound-guided steroid injection for the treatment of de Quervain’s disease: an anatomy-based approach. Skeletal Radiol 47, 1483–1490 (2018). https://doi.org/10.1007/s00256-018-2958-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-018-2958-9